
Abstract
Keywords
Introduction
Recently, exercise transcutaneous oximetry (Ex-TcpO2) has gained popularity both in France and internationally for the management of patients with intermittent claudication (IC).1,2 The European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Asymptomatic Lower Limb Peripheral Arterial Disease and Intermittent Claudication has proposed the use of Ex-TcpO2 as an additional noninvasive method in cases of doubtful arterial origin to confirm or reject the diagnosis of peripheral artery disease (PAD). 3 From a diagnostic perspective, exercise testing can provide an argument for the presence of ischemia as the cause of walking limitation in patients with PAD. 4 Ex-TcpO2 is a dynamic noninvasive diagnostic test that provides indirect skin perfusion. 5 Therefore, it adds significant insight into the treatment algorithm for patients presenting with IC. The technique has been used to diagnose IC in France since 2003 and has been validated against arteriography and computed tomography angiography (CTA).6,7 Furthermore, it has been demonstrated that Ex-TcpO2 exhibits accuracy in noncompressible arteries and diabetic patients.8,9 Therefore, an objective assessment of walking distance and possible nonvascular disease-induced exertional limb pain may be necessary when assessing vascular IC in order to better select those patients who benefit from a surgical intervention. We hypothesized that positive Ex-TcpO2 results would help in the surgical decision, and that patients with positive Ex-TcpO2 results would have improved clinically 1 month after successful revascularization.
Methods
Participants
This study was a single-center, prospective, nonrandomized study designed to assess the perioperative outcomes after Ex-TcpO2 and revascularization in patients with IC for doubtful arterial origin (atypical claudication) or walking distance. Patients were referred by vascular surgeons from January to December 2022 in an outpatient clinic. The exclusion criterion was inability to perform a treadmill test (owing to the presence of leg ulcers or severe cardiopulmonary disease). All patients were offered the best medical treatment according to the guidelines from the European Society for Vascular Surgery (ESVS) 2024. 3 After Ex-TcpO2 and resting ankle–brachial index (ABI) tests, all patients were seen again by their vascular surgeons to decide on their therapeutic plan. The clinician performing the hemodynamic evaluations was not informed about the patient’s eventual surgical treatment perspectives. The decision to use either endovascular technique, open (conventional) surgical or hybrid approach, was left at the discretion of the vascular surgeon. Written informed consent was obtained from all patients. The study complied with the Declaration of Helsinki in research ethics and was approved by the Ethics Committee.
Exercise transcutaneous oxygen pressure
Ex-TcpO2 was carried out using the PeriFlux 6000 Combined System (Perimed, Järfälla, Sweden). The standard technique has been published previously and validated.10,11 Briefly, it consists of using at least four TcpO2 probes simultaneously. A reference electrode was placed on the chest and three other electrodes were positioned on each thigh, buttock, or calf, depending on the location of symptoms. The treadmill walking test was performed with a standardized exercise protocol (3.2 km/h, 10% slope) over 10 min or until maximum pain in the limb was reached. Throughout the test, the decrease from rest of oxygen pressure (DROP) index, which was expressed in mmHg, was calculated automatically as previously described using validated in-house free software (OxyMonitor; https://imagemed.univ-rennes1.fr/fr/oxymonitor/download). 11 During exercise tests, the lowest value for DROP is used to assess for a regional blood flow impairment (RBFI). It was found that a DROP ≤ –15 mmHg was highly predictive of the presence of exercise-induced regional blood flow impairment (RBFI) and sufficiently accurate to diagnose arterial stenoses of ≥ 50% assessed by CTA as the gold standard.6,12–15 Therefore, for the analysis of this study, Ex-TcpO2 results were classified as positive for a minimal DROP value of ≤ –15 mmHg (at least one limb) and negative results if the minimal DROP value is > –15 mmHg (bilateral limb).
Study endpoints and definitions
The main objective of this study was to describe the association between the Ex-TcpO2 results and the perioperative clinical and morphological outcomes after revascularization in patients with IC, including primary sustained clinical improvement and patency rate. Primary sustained clinical improvement was defined as an improvement in Rutherford classification by one or more categories compared with baseline without the need for repeat target lesion revascularization (TLR). The patency rate was defined per the reporting standards of the Society for Vascular Surgery (SVS). 16 A positive Ex-TcpO2 is defined as a DROP ≤ –15 mmHg and is negative for a DROP > –15 mmHg. The ABI was measured as described previously. 17 The Rutherford–Becker classification was used to assess the perioperative clinical outcomes after revascularization. 18 For the morphological perioperative outcomes, a duplex ultrasound examination was realized before the procedure and at 1 month (± 2 weeks) following the index procedure for patency assessment, and was classified according to the following vascular tree: iliac artery (common iliac, external iliac, and internal iliac), femoropopliteal segment (up to P1), and infra-popliteal (P2 and underlying). Revascularization technical success was defined according to the applied procedural technique, the success of the endovascular revascularization procedure was defined by the absence of residual stenosis greater than 30% on the final arteriography, and in open revascularization it was defined as a patent revascularization without any secondary interventions.
Statistical analysis
All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria). Numerical variables were presented as mean ± SD if normally distributed. If not normally distributed, they were presented as median (IQR) based on the Shapiro–Wilk test of normality. Categorical variables were reported as absolute numbers and percentages. Quantitative variable comparisons were conducted using the independent sample t-test or Wilcoxon rank-sum test, as appropriate. For categorical variables, we used the chi-squared test or Fisher’s exact test. A two-tailed p < 0.05 was used to indicate statistical significance. For the association between the results of Ex-TcpO2 with the results of ABI, Fisher’s exact test and the Wilcoxon rank-sum test were used. The primary patency rate was determined by the Kaplan–Meier test and it was used to estimate the proportion of patients with patent vessels through 1 month which is based on duplex ultrasound measurement. To assess the association between maximum pain intensity (MPI) and duplex ultrasound examination lesions with the results of Ex-TcpO2, a univariate analysis was used, and subsequently we performed a multivariate analysis using logistic regression modeling.
Results
Patient characteristics, ABI, and Ex-TcpO2
During the study period, a total of 82 patients with a mean (SD) age of 62 (± 15) years, comprising 53 men, underwent Ex-TcpO2 and were enrolled in the study. At presentation, 53 (65%) of those were Rutherford classification category III, 15 (18%) were category I, and 14 (17%) were category II. None of the patients were categories IV, V, or VI. In this population, indications for the realization of Ex-TcpO2 were to assess the etiology of claudication symptoms (atypical claudication and suspicious or known peripheral neurological or osteoarthritis diseases) accounting for 65% of the cases and in 35% to assess the maximum walking distance (MWD). Out of 82 patients in our cohort, 67 patients (100 limbs) had a positive Ex-TcpO2 and 15 patients had a negative Ex-TcpO2 results, with a majority of those patients being Rutherford category III in both groups (positive group: 66% [n = 44/67] vs negative group: 60% [n = 9/15], p = 0.81). In the Ex-TcpO2 positive group, we observed a higher proportion of men (67% [n = 45/67] vs 53% [n = 8/15], p = 0.31), older patients (65 ±13 vs 58 ± 20, p = 0.43), a higher rate of current smokers (70% [n = 47/67] vs 66% [n = 10/15], p > 0.90), and a significantly lower ABI (0.65 ± 0.2 vs 0.92 ± 0.2, p < 0.001) compared with the Ex-TcpO2 negative group. Previous peripheral revascularization and comorbidities were more common in the Ex-TcpO2 positive group. However, none of these differences was found to be statistically significant. Demographic information, comorbidities, medications, and duplex scan characteristics are reported in Table 1. A flow diagram of the study showing the distribution of 82 patients throughout the course of the study is shown in Figure 1. The distribution of the ABI categories among the two groups is shown in Figure 2 per limb analysis (164 limbs).
Comparison of the distribution of baseline characteristics between Ex-TcpO2 groups (N = 82).
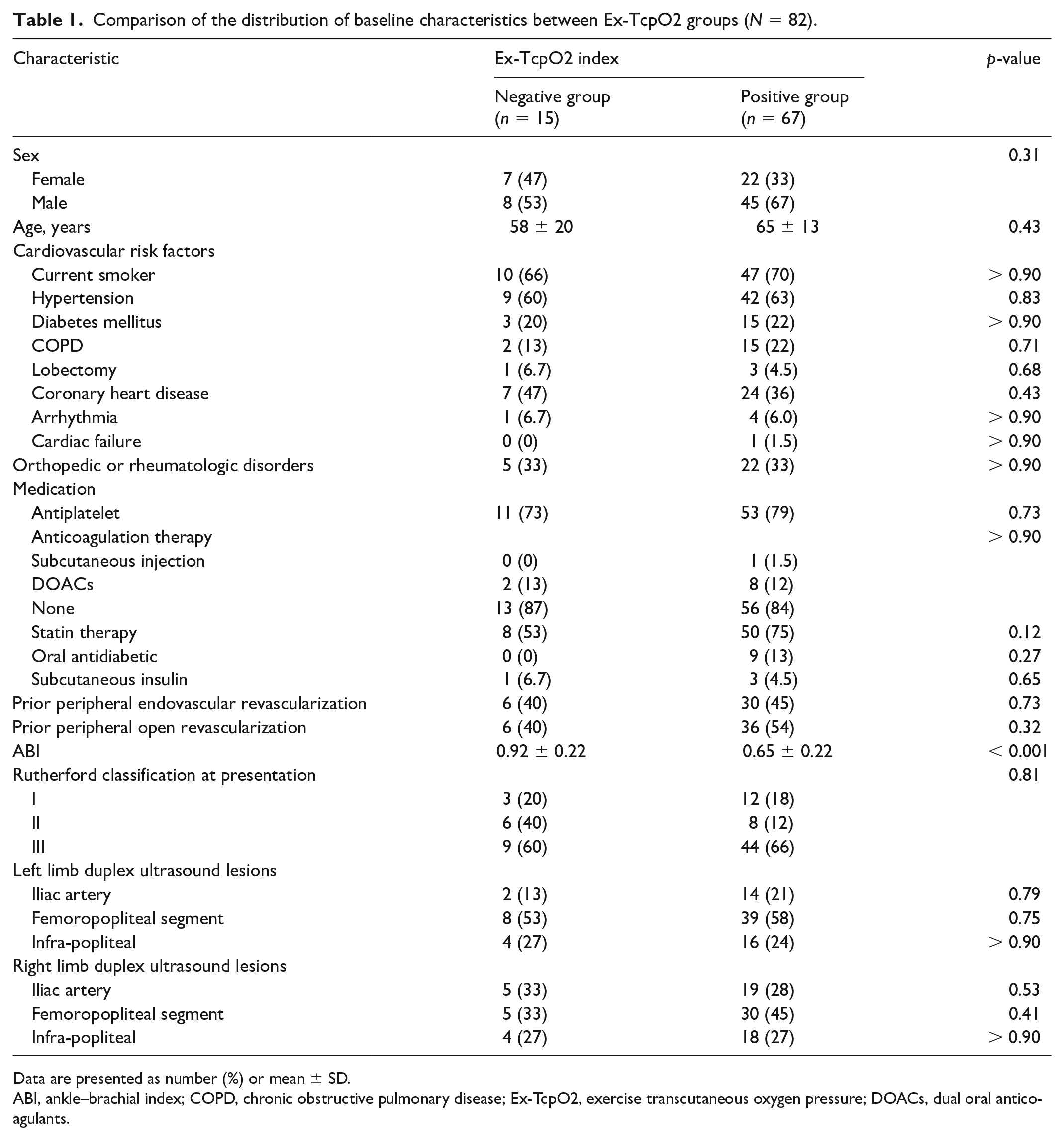
Data are presented as number (%) or mean ± SD.
ABI, ankle–brachial index; COPD, chronic obstructive pulmonary disease; Ex-TcpO2, exercise transcutaneous oxygen pressure; DOACs, dual oral anticoagulants.
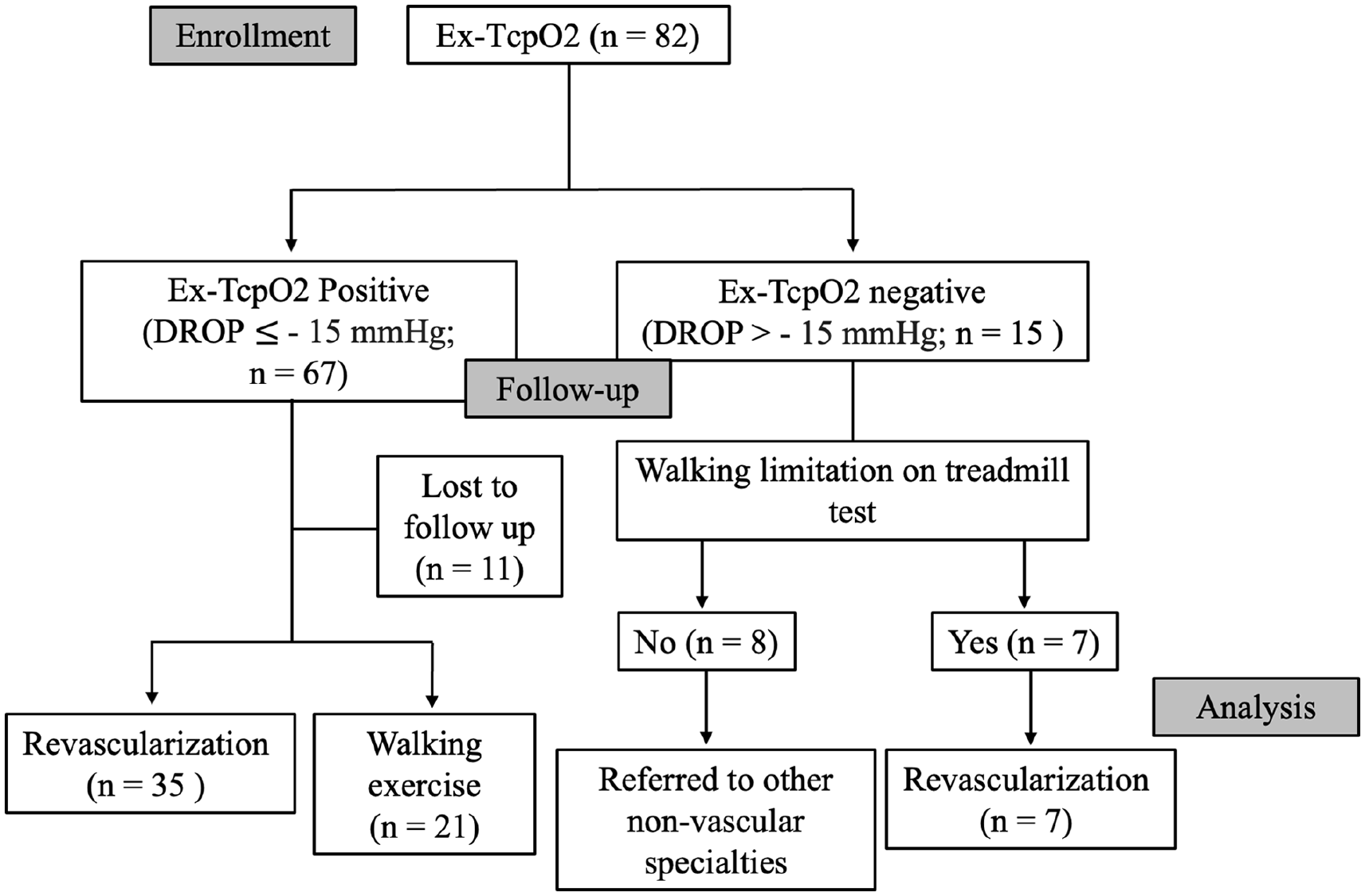
Flow diagram of the study showing the distribution of 82 patients with Ex-TcpO2 measurement.
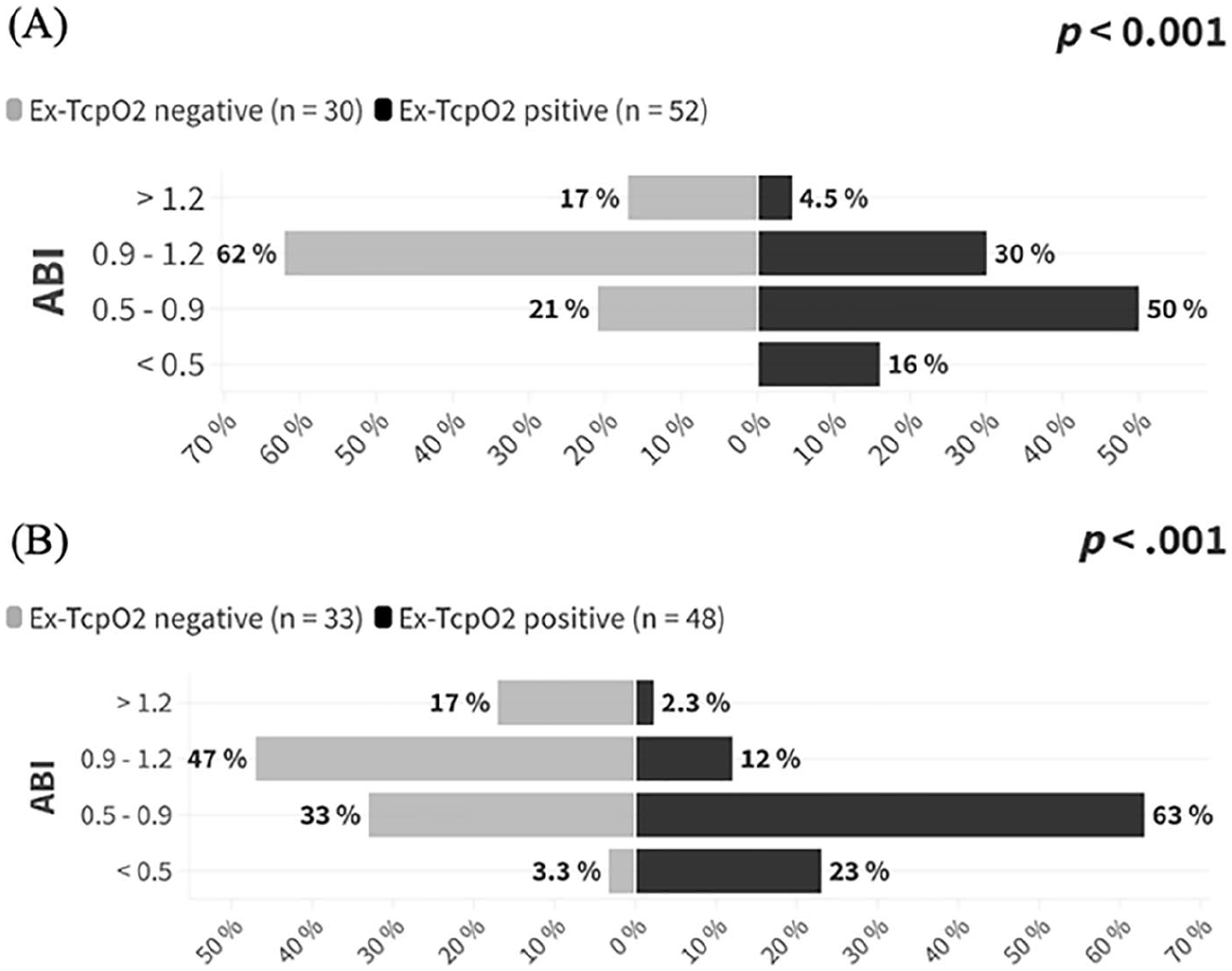
Distribution of patients with positive and negative results of Ex-TcpO2 for each category of ankle–brachial index (n = 82) per symptomatic limb:
Walking distance and walking time on treadmill
As illustrated in Figure 3, the comparisons between groups revealed a significant disparity in the variation of the MWD and maximum walking time (MWT). The Ex-TcpO2 positive group had a significantly lower median MWD than the negative group (200 m [IQR: 150, 300] vs 525 m [IQR: 500, 872], p < 0.001) and a significant lower median MWT (300 s [IQR: 232, 377] vs 540 s [IQR: 300, 600], p = 0.001). Table 2 illustrates a subgroup analysis addressing various patient characteristics that could influence the treadmill speed protocol. A significant association was observed between reduced standard speed in elderly patients (p = 0.01), patients with cardiopulmonary diseases (p 0.02), and orthopedic or rheumatologic disorders (p = 0.038).
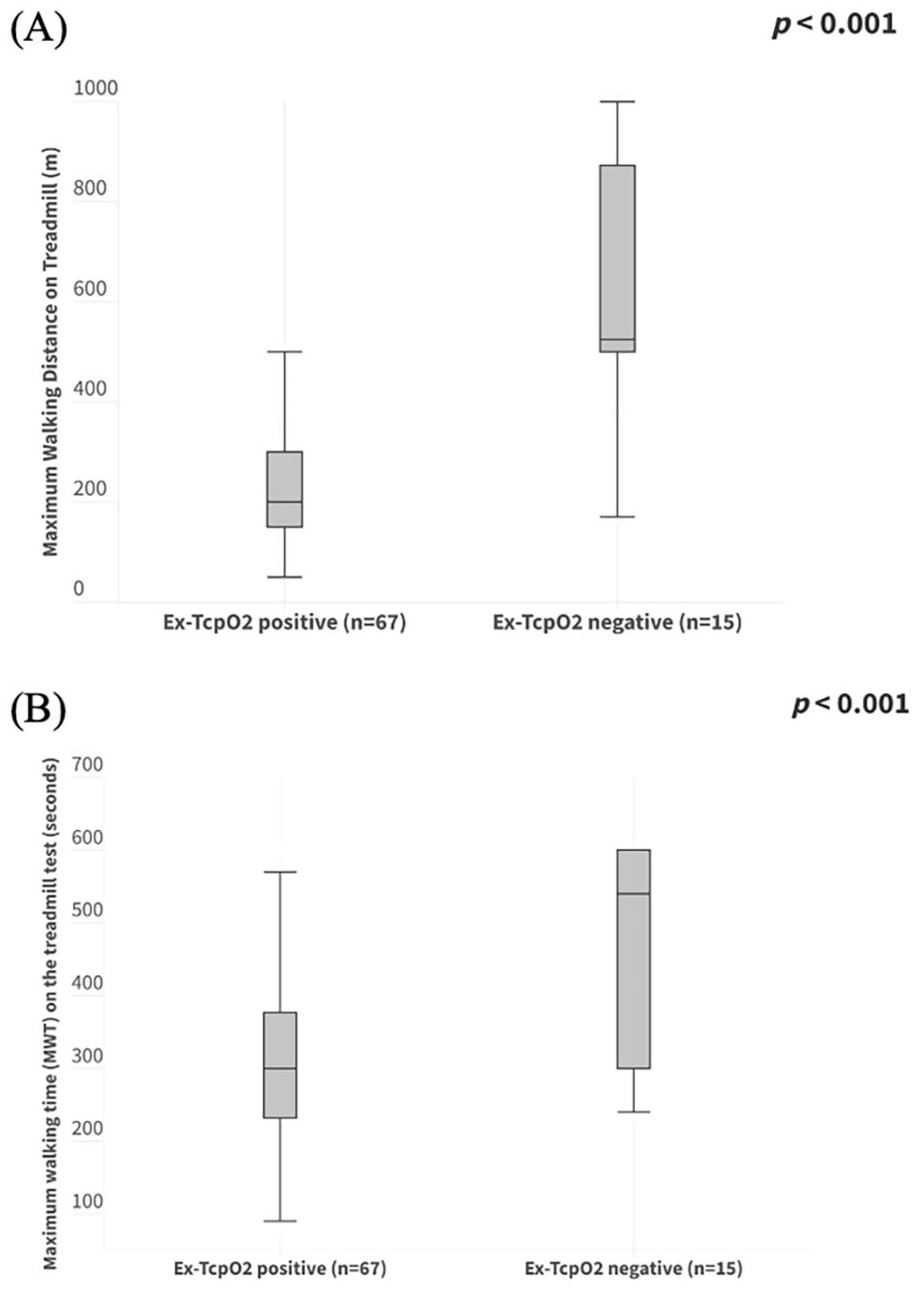
Median
Comparison of reduced treadmill speed protocol according to patient baseline characteristics.
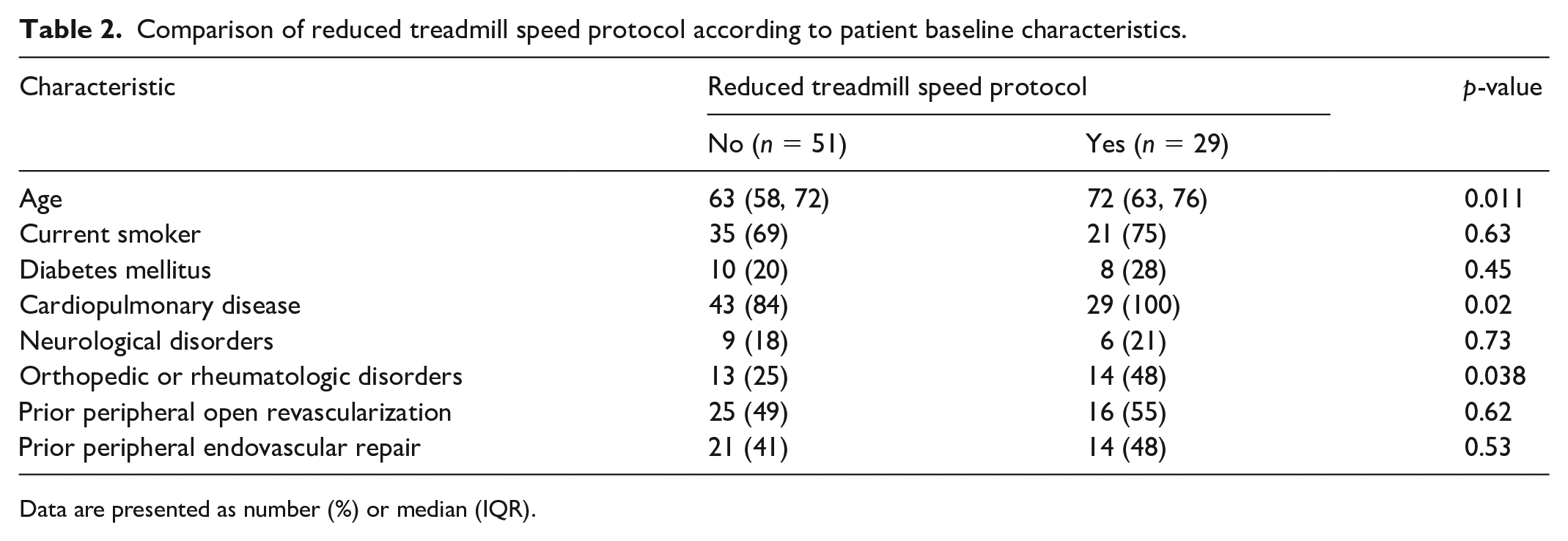
Data are presented as number (%) or median (IQR).
Association between Ex-TcpO2, arterial lesions, and maximum pain intensity (MPI) location
The univariate analysis showed a significant association between the presence of iliac artery lesions and MPI at the level of the buttock (right-limb: p < 0.001; left-limb: p = 0.004) and the DROP positive results (right limb: p = 0.002; left limb: p = 0.006). No significant relationship has been found between other arterial lesions and MPI. This suggested that the presence of iliac lesions is likely associated with pain in the buttock as well as a DROP ≤ –15 mmHg at the buttock. Moreover, performing a multivariate analysis, including all the variables, confirms a strong positive association of the presence of iliac lesions in the setting of pain at the buttock and a DROP ≤ –15 mmHg at the level of the buttock.
Perioperative outcomes and follow-up
Out of a total of 15 patients with negative Ex-TcpO2, eight did not experience any walking limitations during the treadmill test. Because of this, they were referred to other non-vascular specialties. The remaining seven patients, despite the absence of an obvious cause of their walking limitation and a failed walking program for 3 months after the initial presentation, underwent an attempt at revascularization. Among the 67 patients with positive Ex-TcpO2, 21 underwent walking program rehabilitation and medical treatment only due to an acceptable MWD, 35 patients underwent revascularization due to a failed walking program for 3 months after their initial presentation and a severely limited MWD, and 11 patients were lost to follow-up. As demonstrated in Table 3, a total of 42 patients underwent revascularizations and all of those completed 1 month of follow up. Twenty-nine and seven patients underwent endovascular procedures in the Ex-TcpO2 positive and negative groups, respectively. The remaining six patients from the Ex-TcpO2 positive group underwent, in equal proportion, either open or hybrid procedures. The revascularization technical success rate and primary patency rate were 100% for each group. One patient had residual stenosis of 50% and a nonflow-limiting dissection at 1 month of follow up in the positive group and none in the negative group. Primary sustained clinical improvement was significantly greater in the Ex-TcpO2 positive group; none of the patients in the Ex-TcpO2 negative group have demonstrated clinical improvement (97% [n = 34/35] vs 0% [n = 0/7], p < 0.001, respectively).
Comparison of revascularization type and postrevascularization outcomes at 1 month of follow up.
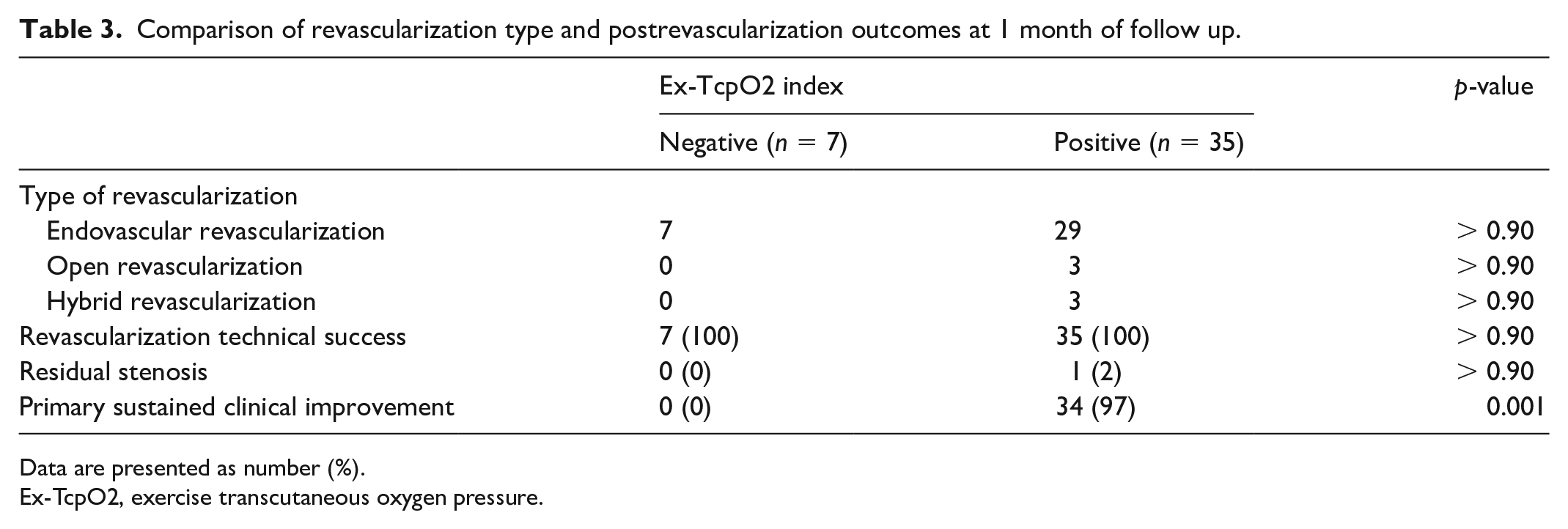
Data are presented as number (%).
Ex-TcpO2, exercise transcutaneous oxygen pressure.
Discussion
This study shows that patients with positive Ex-TcpO2 tests experienced significant improvement in their clinical symptoms subsequent to a successful revascularization regardless of the operative technique, whereas patients who had negative Ex-TcpO2 tests and underwent a successful revascularization did not experience any benefit or improvement in their initial symptoms during follow up. Furthermore, patients in the Ex-TcpO2 positive group had significantly less MWD and MWT, and average ABI than patients in the negative group. Mahe et al. have reported their first case report in the United States from utilizing Ex-TcpO2 in diagnosing IC of doubtful arterial origin with improved clinical symptoms after endovascular revascularization in a patient with positive Ex-TcpO2 results. 19 For patients with a normal resting ABI suspected to have PAD, the American Heart Association (AHA) recommends performing an ABI using two different diagnostic criteria: either an ABI decrease > 20% or a pressure decrease > 30 mmHg. 20 However, a previous study has shown a discordance between these two proposed criteria. 14 Ex-TcpO2 holds significant interest in cases where the lower-limb arteries are incompressible, in which the ABI measurement can be falsely negative. It has been demonstrated that one out of seven individuals suffering from proximal claudication has a resting ABI > 0.90. 21 These reports seem consistent with our results, where 30% of limbs with positive Ex-TcpO2 had an ABI above 0.90. These findings could suggest that proximal ischemia may be an underestimated cause of exercise-related low back pain, and this argument has been addressed. 22 These discrepancies could call into question the widely accepted high positive predictive value of a resting ABI under 0.90 for proving the arterial origin of calf pain in patients with claudication. 23 Furthermore, recent studies have found a discrepancy between Ex-TcpO2 results and postexercise ankle pressure criteria proposed by the AHA, and confirming that exercise tests are not equivalent.24,25 One of the advantages of Ex-TcpO2 over postexercise ABI is its ability to provide evidence of exercise-induced regional blood flow impairment (RBFI) during and after exercise. 5
Proximal ischemia can cause buttock, hip, or lower back pain or pseudo-sciatica. 26 Furthermore, the ability to estimate exercise-induced proximal ischemia is becoming of greater interest due to both isolated internal iliac stenosis and in patients with aorto-bi-femoral bypasses. 27 We observed a significant association between a DROP ≤ –15 mmHg at the level of the buttock and iliac artery stenosis and MPI at the buttock. Therefore, a greater comprehension of the correlation between symptoms and ischemia is imperative for a more precise diagnosis. In our practice, we have implemented the utilization of Ex-TcpO2 to bridge the gap between imaging and patients’ symptoms to identify proximal ischemia and to obtain an objective rationale to support the surgical decision in treating patients with IC.
The National CINEY-SOFT trial, including more than 600 Ex-TcpO2 investigations, has led to a significant change in the diagnostic hypothesis for pre- and posttest diagnosis in 44.1% of patients with suspected vascular disease. In particular, the investigators identified that IC-like symptoms were of nonvascular origin in 45 patients, whereas in 41 patients the results of Ex-TcpO2 confirmed exercise-induced lower-limb ischemia as the most likely cause of walking limitation in patients where the pretest diagnosis was not vascular IC. 28
A combination of modified post-exercise ABI criteria (postexercise ABI decrease ≥ 18.5%, or postexercise ABI < 0.90) and Ex-TcpO2 for evaluating PAD has been proposed and showed a better diagnostic ability. However, an external validation remains to be performed. 29 It is recognized that Ex-TcpO2 is time-consuming and requires a dedicated vascular medicine laboratory. Nevertheless, Ex-TcpO2 contributes to the reach of an eventual diagnosis for many patients in complex situations with atypical claudication. Furthermore, it has been demonstrated to be cost-effective from a clinical standpoint and applicable in various vascular institutions. 28
Study limitations
The current study is a single-center study with a selective patient cohort, as not all the patients who presented with IC at our department had received Ex-TcpO2 because the decision was left to the surgeon. This may suggest a potential selection bias, although it also reflects a real-life cohort of patients. Second, the postexercise ABI was not assessed in this study. However, this has been addressed previously in the literature.24,25,29 Lastly, numerous clinical aspects still require clarification regarding the utilization of Ex-TcpO2. It would be interesting to compare the results of preoperative Ex-TcpO2 with postrevascularization Ex-Tcpo2 in patients with IC to show its potential ability to predict the clinical outcome of revascularization.
Conclusion
We believe that this is the first prospective study to evaluate the clinical improvement postrevascularization for patients who have had Ex-TcpO2 that guided the operative decision in a vascular surgical department. Our study highlights the potential benefit of using Ex-TcpO2 in the diagnosis of patients with IC, especially in patients with atypical claudication or claudication of doubtful arterial origin. The Ex-TcpO2 test seems to improve diagnostic performance, specifically for proximal claudication. The results do not invalidate the value of ABI for evaluation of PAD, but further support the value of treadmill exercise testing for providing accurate MWD and MPI and confirming the vascular origin of walking limitations.
Footnotes
Acknowledgements
We thank Sara Chaouki (data analyst, Paris, France) for her contribution in statistical analysis.
Data availability statement
The data presented in this study are available on request from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.