
Abstract

What is renal artery stenosis (RAS)?
The kidneys are responsible for regulating the body’s fluid balance and blood pressure. Renal artery stenosis (RAS) involves a narrowing (stenosis) of the arteries that supply blood to the kidneys. If blood flow to the kidneys decreases due to stenosis, hormones called renin and aldosterone are released. These hormones cause blood pressure to increase. RAS is a common cause of high blood pressure after the most common essential hypertension, which is high blood pressure that has no specific cause, but it is thought to be related to genetics, diet, and obesity.
What causes RAS and who is at risk?
The three main causes of RAS are atherosclerosis, fibromuscular dysplasia (FMD), and vasculitis.
Renal atherosclerotic disease
Atherosclerosis is the leading cause of RAS, accounting for over 90% of cases. 1 This condition involves the narrowing of the portion of the renal artery closest to the aorta, known as the proximal renal artery, as seen in Figure 1. This narrowing is due to the buildup of plaque. When patients have risk factors for atherosclerosis, including high cholesterol, plaque can accumulate in the walls of the various arteries, known as peripheral artery disease. Plaque buildup may stiffen the vessels and cause stenosis that restricts blood flow to the kidneys in RAS.

Computed tomographic angiography scan: abdomen image showing atherosclerotic narrowing of the left renal artery. The white arrow designates the narrowing of the proximal portion of the artery, which is closest to the aorta.
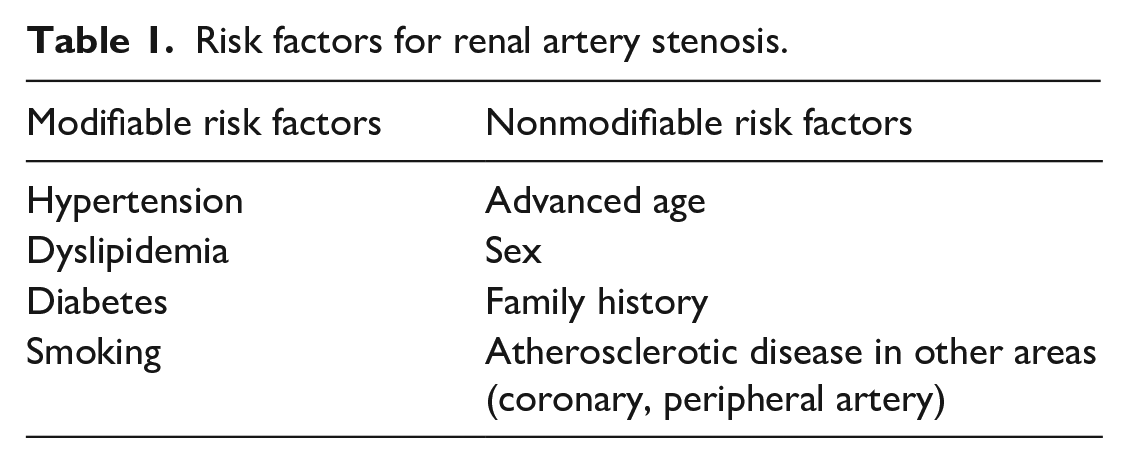
Risk factors that can increase the risk of developing RAS are shown in Table 1. Patients with diabetes, hypertension, hyperlipidemia, and a history of smoking are at increased risk of atherosclerotic RAS. 2
Risk factors for renal artery stenosis.
Fibromuscular dysplasia
A less common cause of RAS is FMD. In the case of RAS due to renal FMD, blood flow to the kidney is limited by abnormalities in the structure of the artery wall with alternating areas of stenosis (narrowing) and dilation (enlargement). FMD accounts for less than 10% of RAS, and usually affects women typically around the age of 50. 1 Unlike RAS due to atherosclerotic disease, RAS due to FMD has a characteristic ‘string-of-beads’ appearance on imaging, as seen in Figure 2, and tends to involve the more distal portion of the renal artery that is closer to the kidney. RAS due to renal FMD may cause hypertension, especially among younger women. 3
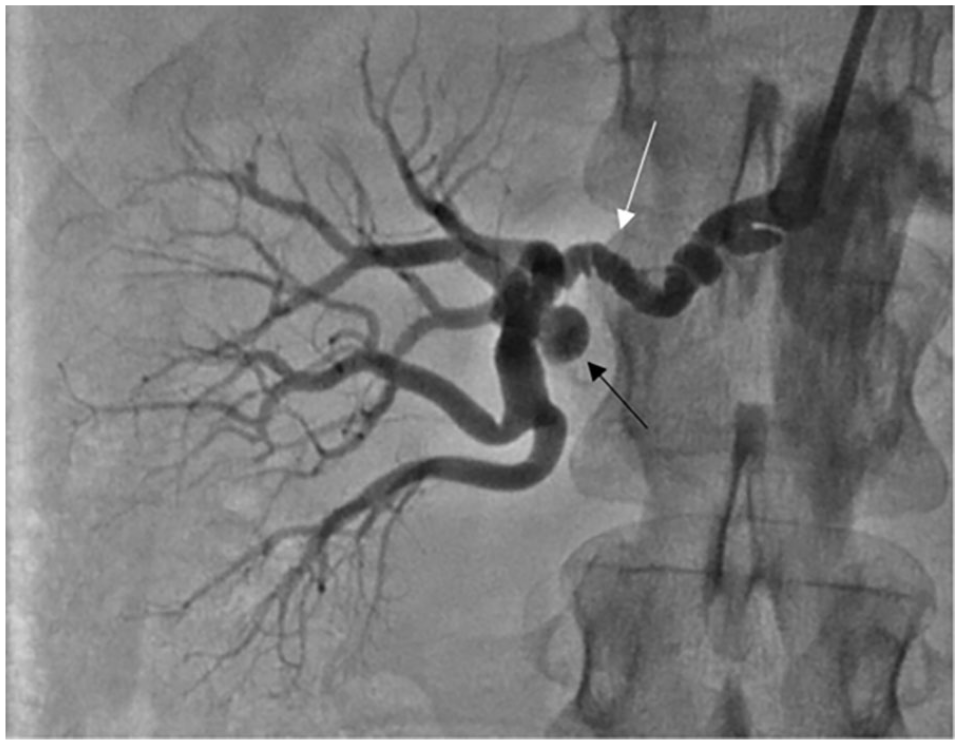
Typical angiogram findings of the ‘string-of-beads’ (white arrow) characteristic of multifocal fibromuscular dysplasia. The patient also has a small right renal aneurysm (black arrow).
Vasculitis
Vasculitis is an uncommon cause of RAS that is due to inflammation and wall thickening of the renal arteries. Some examples of vasculitis that could contribute to RAS include Takayasu’s arteritis, polyarteritis nodosa, and granulomatosis with polyangiitis. 1
What are the symptoms of RAS?
Patients with RAS often have no symptoms, so it is commonly underdiagnosed. Some cases of RAS are found incidentally during imaging studies for other conditions. However, RAS can cause high blood pressure and kidney problems. Patients with RAS may experience an increase in creatinine, a blood test used to measure kidney function which, when high, indicates kidney issues. A common manifestation of RAS is severe or resistant hypertension. Severe hypertension is when the blood pressure is > 180/120 mmHg; resistant hypertension is when the blood pressure is > 140/90 mmHg despite taking three or more blood pressure medicines, including a diuretic. The presence of severe or resistant hypertension typically prompts an evaluation for an underlying cause. Symptoms of severe high blood pressure may include blurry vision, stroke, chest pain, difficulty breathing, headache, or confusion and should prompt immediate evaluation at the emergency room.
How is RAS diagnosed?
Routine screening for RAS is not recommended. However, when a patient has severe or resistant hypertension, particularly in the setting of kidney damage or other risk factors, a renal duplex ultrasound is often recommended as the first-line imaging test. An ultrasound is a noninvasive technique that provides information about the blood flow to the kidney; it can identify the location and severity of stenosis. It is important to note that there are limitations to obtaining a diagnostic image, such as the skill level of the technician and physical characteristics of the patient. Therefore, if there is a high suspicion for RAS, other imaging studies might be needed.
Other imaging tests, such as computed tomographic angiography (CTA) or magnetic resonance angiography (MRA), can provide better visualization of the arteries to determine the location and severity of RAS. CTA is particularly useful for detecting RAS due to FMD. CTA and MRA can also help assess the abdominal aorta and guide the approach for restoring blood flow to the renal artery if needed. However, there are risks associated with both imaging modalities. Repeated exposure to radiation with CTA may increase the risk of cancer or have other negative effects. The intravenous contrast can cause damage to the kidneys, especially in patients with preexisting chronic kidney disease. 4 Gadolinium-based contrast agents in MRA have rarely been associated with nephrogenic systemic fibrosis, the thickening and hardening of skin and other organs, in patients with severe chronic kidney disease. 5 Additionally, CTA and MRA may miss RAS. Thus, invasive angiography, a catheter-based method, remains the gold standard to detect RAS. 6 Angiography involves a minimally invasive procedure in which a catheter is placed through the groin or arm, and is advanced to the renal arteries. Contrast material is then released into the blood, which allows visualization of blood flow through the renal artery with an X-ray. This procedure provides high-quality images that can be used for diagnosis and treatment.
How is RAS treated?
Lifestyle modifications
Lifestyle modifications can affect the progression of RAS. Adopting healthy lifestyle habits, including quitting smoking, maintaining a regular exercise regimen, and following a heart-healthy diet, can help lower blood pressure and manage risk factors related to RAS.
Medical treatment
If a patient with RAS has high blood pressure, they are typically prescribed blood pressure medications, such as angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs), to control blood pressure per current guidelines. If a patient has RAS due to atherosclerosis, statins can help to delay the progression of plaque in the arteries and reduce the risk of heart attack and stroke. An antiplatelet agent is often prescribed for patients with RAS (such as aspirin) to prevent clot formation in the renal arteries. It is also important to treat diabetes to minimize cardiovascular risk.
Endovascular treatment
If high blood pressure persists despite taking three or more blood pressure medications, medical treatment may not be adequate and endovascular (minimally invasive) treatment is considered. Endovascular treatment can be considered when patients are experiencing high blood pressure that is difficult to control, progressive decline in kidney function, or complications related to RAS including heart failure or fluid in the lungs, known as pulmonary edema. 6
Endovascular treatment can include balloon angioplasty, which involves the inflation of a balloon with or without a stent in the renal artery, as shown in Figure 3. The goal is to open the narrowed vessel and restore blood flow to the kidney. Stenting is more effective and durable than angioplasty alone in patients with atherosclerotic RAS, in terms of keeping the blood vessel open and improving blood pressure and kidney function. 7 However, patients with RAS due to renal FMD typically undergo angioplasty without a stent. Endovascular treatment carries risks, such as acute kidney injury, bleeding, infection, and direct injury to a renal artery, among other things.
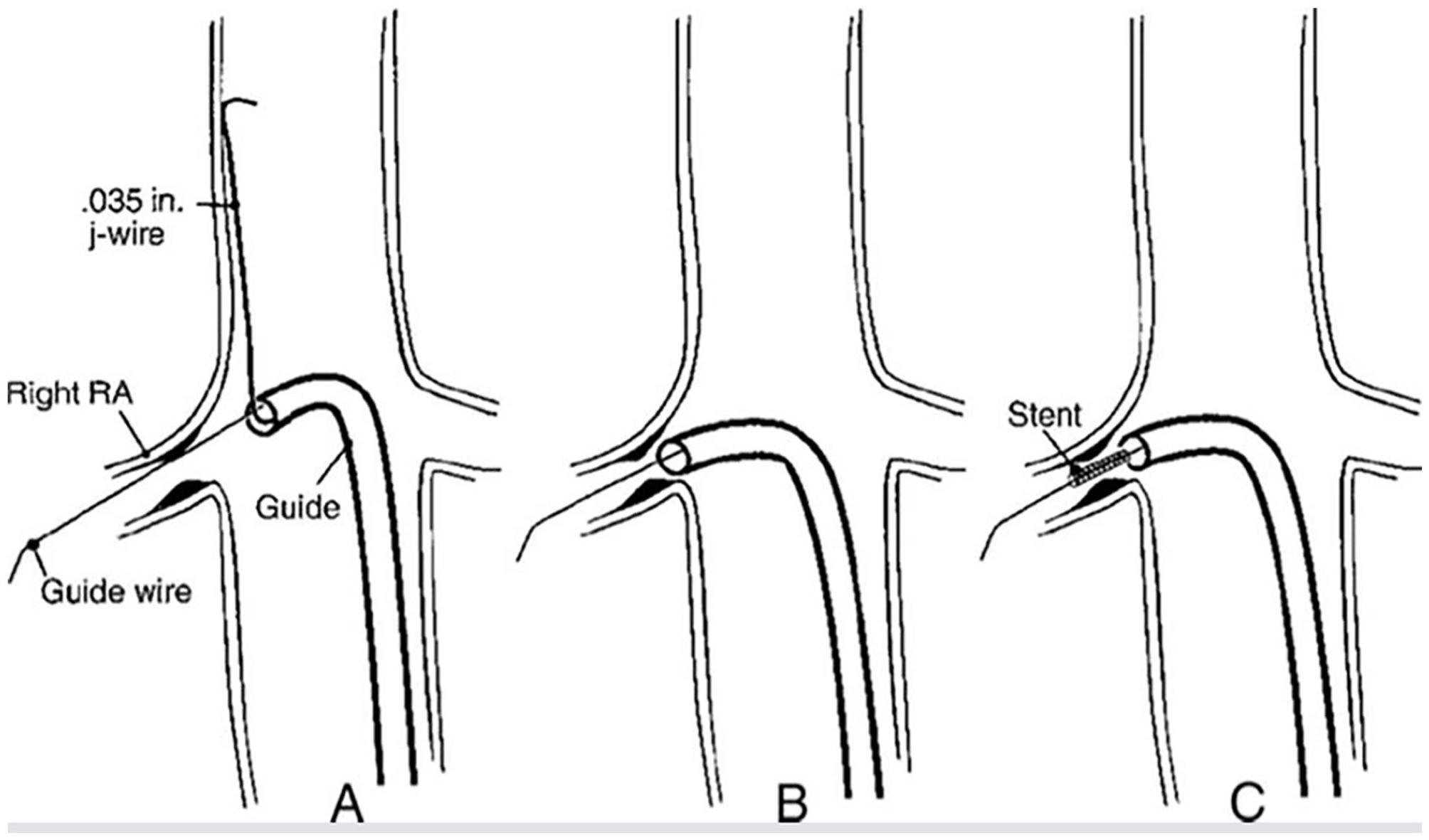
With endovascular treatment, a guidewire is advanced until it reaches the renal artery
Several studies have looked at renal artery revascularization, primarily with endovascular treatment, to lower blood pressure and/or to slow the progression of kidney disease in patients with atherosclerotic RAS. However, the evidence is controversial, as revascularization showed no significant reduction in occurrence of renal events, major cardiovascular events, or death in two randomized clinical trials, suggesting that medical treatment and revascularization provide similar clinical outcomes for patients with RAS.6,8 Further research about the effects of revascularization on blood pressure and major adverse cardiac events (MACE) is required. That said, revascularization is still considered in carefully selected patients when optimal medical therapy is not adequate to control blood pressure.
For patients with RAS due to renal FMD, the likelihood of ‘curing’ hypertension with revascularization depends on age, duration of hypertension, and type of FMD. 9 The best candidates for revascularization are younger patients with FMD, a short duration of hypertension, and no underlying kidney disease. 9
Surgical treatment
Endovascular treatment may not be possible if a patient has RAS and complex anatomy that cannot be well treated with balloon angioplasty and stenting or in the presence of a renal artery aneurysm, for example, which occurs when the vessel wall is weakened and expands. Other indications for surgical treatment could include severe RAS, a blockage in the renal artery, or progressive decline in kidney function. Additionally, if a patient does not respond to medical management and cannot receive endovascular treatment, then open surgical treatment may be recommended to restore the blood flow. There are two surgical procedures typically performed in such cases: aortorenal bypass surgery and endarterectomy.
Summary
RAS is narrowing of the kidney arteries; it may be caused by atherosclerosis or, less commonly, fibromuscular dysplasia or vasculitis. Lifestyle modifications, including smoking cessation, healthy diet, exercise, and treatment adherence, can reduce the risk for RAS and associated complications such as cardiovascular events. Treatment involves medical management to control high blood pressure and other treatments to reduce overall cardiovascular risk. If the blood pressure remains elevated or kidney function worsens despite blood pressure treatment, then revascularization (endovascular or surgical) is considered.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.