
Abstract
The association between fibromuscular dysplasia (FMD) and spontaneous cervical artery dissection (SCeAD) has been recognized, but the available evidence on this relationship is scant. Therefore, the main goal of our study was to systematically evaluate FMD frequency, clinical characteristics and vascular bed involvement in patients with SCeAD. Among 230 patients referred to the ARCADIA-POL study, 43 patients (mean age 44.1 ± 8.9 years; 15 men and 28 women) with SCeAD were referred. Also, 135 patients with FMD were compared to patients with and without SCeAD. Patients underwent: ambulatory blood pressure measurements, biochemical evaluation, echocardiographic examination, and whole body computed tomographic angiography. FMD changes were found in 39.5% of patients with SCeAD. There were no differences in clinical characteristics between patients with SCeAD and FMD and those without FMD, except for a tendency towards a higher female ratio in SCeAD patients with FMD. There were no differences in other parameters describing target organ and SCeAD characteristics. Patients with SCeAD and FMD compared to those without SCeAD were characterized by a lower frequency of hypertension and a higher frequency of hyperlipidemia and history of contraceptive hormone use. Our study indicates a high incidence (39.5%) of FMD in subjects with SCeAD. Since there are no distinctive discriminating factors between patients with SCeAD and FMD and those without FMD, FMD should be suspected in all patients with SCeAD.
Introduction
Spontaneous cervical artery dissection (SCeAD) has been increasingly recognized as a major cause of ischemic stroke in young and middle-aged adults. Of note, the clinical course may be asymptomatic and only discovered incidentally when imaging is performed for another clinical indication. Also, the clinical presentation may vary from mild with non-specific symptoms to fatal cerebrovascular complications. Depending on the affected vessel, SCeAD may be divided into spontaneous internal carotid artery dissection (SICAD) and spontaneous vertebral artery dissection (SVAD).1–4
The pathophysiology of SCeAD is poorly understood and includes both constitutional and environmental factors. A causal association is often difficult to establish, so other predisposing factors may also play a part in the development of SCeAD. An association between underlying vasculopathy, such as fibromuscular dysplasia (FMD) and spontaneous cervical (carotid and vertebral) artery dissection, was recognized but the available evidence on this relationship is scant.1–3,5
Therefore, the aim of our study was to evaluate the frequency of FMD in any vascular bed in patients with SCeAD and systematically evaluate clinical characteristics and vascular bed involvement. We compared the clinical characteristics of patients with SCeAD and coexisting FMD to those without FMD. Then, we analyzed if there are differences in clinical characteristics between patients with FMD with and without history of SCeAD.
Methods
The prospective ARCADIA-POL study was instituted in January 2015, based on Polish–French collaboration at the Institute of Cardiology in Warsaw, Poland. The main goal was to provide clinical characteristics of patients with FMD in Poland. 6 Beginning in July 2015, the coordinating committee of our study, based on previous reports, decided to extend the referral pattern with the aim to include consecutive subjects with SICAD and SVAD. Inclusion criteria were also extended for patients with coronary artery dissection. The protocol was approved by the ethics committee of the Institute of Cardiology in Warsaw, and all participants provided written informed consent.
From July 2015 until December 2017, 42 consecutive patients with SCeAD were referred from six departments of neurology participating in the ARCADIA-POL study. In one female patient with newly diagnosed renal FMD, asymptomatic spontaneous SICAD was found during evaluation, giving a total number of 43 patients with SCeAD. All patients were assessed in the Department of Hypertension at the Institute of Cardiology 3 months after the SCeAD diagnosis.
Also, 135 patients with FMD and no history of SCeAD and no SCeAD on current computed tomographic angiography (CTA) of cervical arteries were included in the study and were compared to SCeAD patients with FMD (Figure 1). Patients without confirmed FMD and those with a history of arterial dissection (not cervical) were excluded from the study. There were no patients with SCeAD and dissection in other arteries.
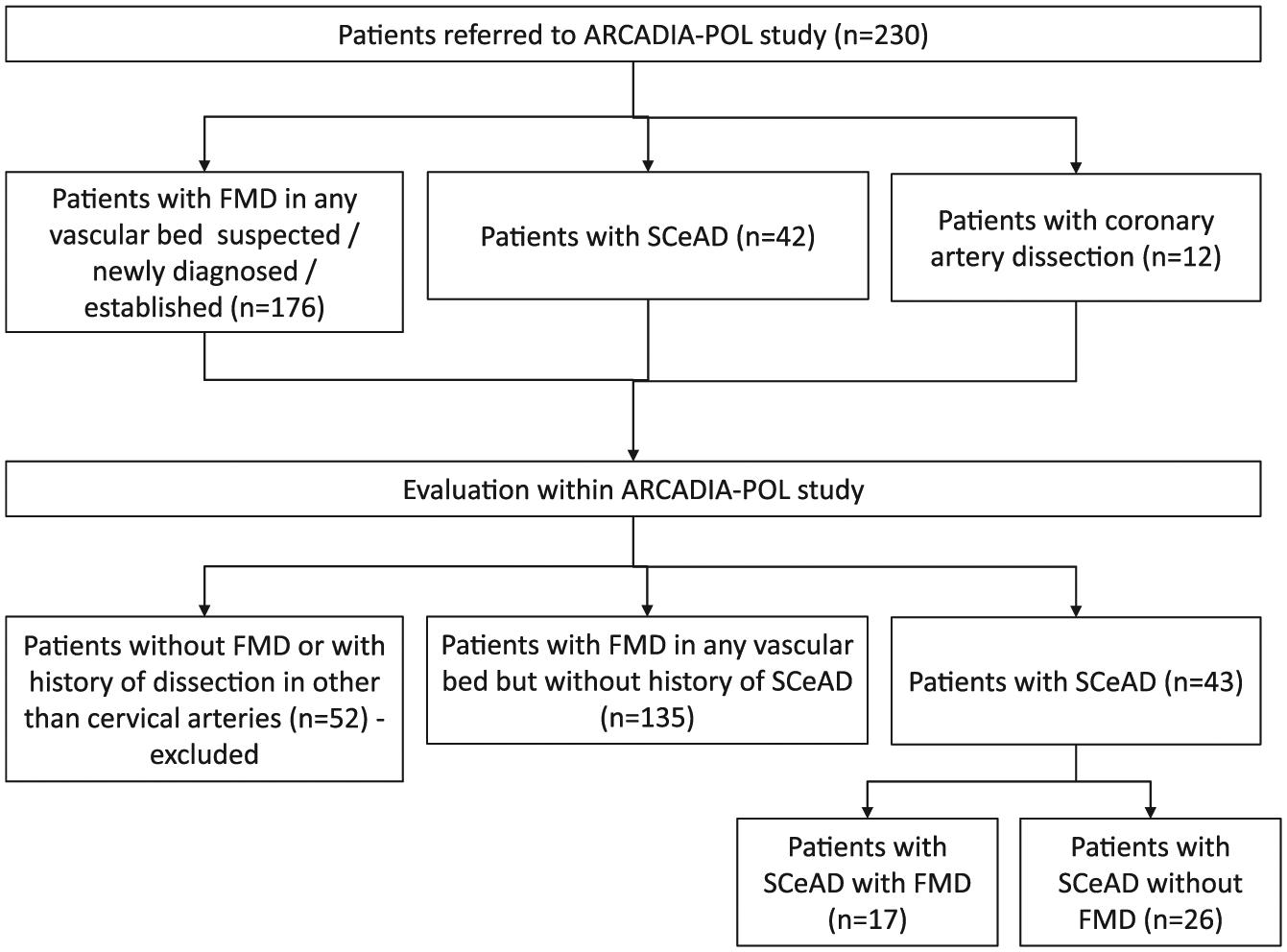
Flow chart showing the selection of patients with SCeAD and FMD in the ARCADIA-POL Registery.
All patients underwent detailed clinical evaluation including office and ambulatory blood pressure measurements (ABPM), biochemical evaluation, biobanking, echocardiographic examination, duplex Doppler of carotid and abdominal arteries, and whole body CTA. Hypertension was defined as office blood pressure ⩾ 140/90 mmHg or 24-hour ABPM levels of ⩾ 130/80 mmHg and/or current antihypertensive medication. 7
Based on structured interviewing, the potential risk factors and characteristics of SCeAD were assessed (see the online supplementary material). In case of stroke, the National Institutes of Health Stroke Scale (NIHSS) score and Rankin Scale were assessed at admission and after 3 months.
SCeAD was defined as occurring spontaneously or after physical exertion or minor trauma. 8 A diagnosis of SCeAD was made by (1) cervical or cerebral CTA/MRI (magnetic resonance imaging) showing wall hematoma or (2) CTA, ultrasound, or intra-arterial digital subtraction angiography demonstrating double lumen, a string sign, an intimal flap, or a dissecting aneurysm at a non-bifurcation site. Multiple SCeAD was defined as dissection of at least two cervical arteries. All images were re-examined by two independent radiologists (MJ and IM) to confirm the diagnosis.
Computed tomographic angiography
In all patients, CTAs of the cerebrovascular, upper and lower extremities, and renal and mesenteric arteries were performed. Arterial phase contrast-enhanced CTA images were obtained using a dual-source CT scanner, SOMATOM Force (collimation 192 × 0.6 mm, spatial resolution 0.24 mm, rotation time 0.25 s, slice thickness 0.6–1 mm; Siemens Healthcare Erlangen, Germany).
FMD was diagnosed as non-atherosclerotic arterial encroachment or stenosis affecting the trunk or branches of medium-sized arteries, in the absence of aortic wall thickening and biochemical evidence of inflammation. FMD was divided into multifocal and focal types. Multifocal FMD was diagnosed when characteristic sequential areas of dilation greater in dimension than the adjacent normal vessel and separated by areas of narrowing were identified.9–11 Focal FMD was defined as focal concentric stenosis. 12 The evaluated arteries were divided into vascular beds as follows: (1) renal, (2) cerebrovascular, (3) mesenteric, (4) upper extremity, and (5) lower extremity. Multisite FMD was defined as the presence of FMD changes (multifocal or focal disease) in two or more of the vascular beds. The diagnosis of FMD and its types was established based on CTA examination by two independent investigators (MJ and IM). Suspected significant artery stenosis was defined as signs of significant stenosis on duplex Doppler examination (including increased velocity and/or turbulence) or on CTA, and it was verified in most cases by renal angiography.9–11
Evaluation of blood pressure values, biochemical parameters, and target organ damage
The material and methodology of blood pressure measurements, including ABPM, biochemical evaluations, echocardiography, renal Doppler ultrasound, and carotid intima–media thickness (IMT) by carotid artery ultrasound has been published previously and is discussed in the online supplementary material. 6
Statistical analysis
Data are presented as mean ± SD, median (interquartile range (IQR)), or number and frequency. The values of variables were compared between the groups. Continuous and discrete variables were compared using Student’s t-test and the Mann–Whitney test, and categorical variables as well as the prevalence rates were compared using the chi-squared test or Fisher’s exact test. All statistical analyses were performed with PASW Statistics 18 (SPSS Inc., Chicago, IL, USA); p ⩽ 0.05 was considered statistically significant.
Results
We included 43 patients (mean age 44.1 ± 8.9 years; 15 males and 28 females) with confirmed SCeAD. There were 29 patients with SICAD, 12 patients with SVAD, and two patients with concomitant SICAD and SVAD. FMD changes were found in 17 patients (39.5%). FMD was found in the following vascular beds: renal in nine patients (20.9%), cerebrovascular in 10 patients (23.3%; Supplementary Table 1), and upper extremity arteries (one patient with FMD in the subclavian artery). FMD was not found in other vascular beds in any patients. Multisite FMD was found in four patients. Among patients with renal FMD, one significant renal artery stenosis was found and proven on renal angiography. Evaluation of renal arteries by duplex Doppler examination and CTA in patients with SCeAD and renal FMD has been described in Supplementary Table 2. There were 10 patients with multiple SCeAD. Patients with multiple SCeAD were characterized by a higher frequency of FMD compared to patients with single SCeAD, but the difference did not reach statistical significance (60.0% vs 33.3%; p = 0.13). Hypertension was present in 27 patients with SCeAD; it was newly diagnosed hypertension in eight patients (29.6%) and most patients (44.4%) were treated with one antihypertensive drug. Febrile infection did not precede SCeAD nor were connective tissue disorders found in any patients. In patients with SCeAD and FMD, there was no family history of connective tissue diseases, aneurysms, dissections, sudden death, or FMD.
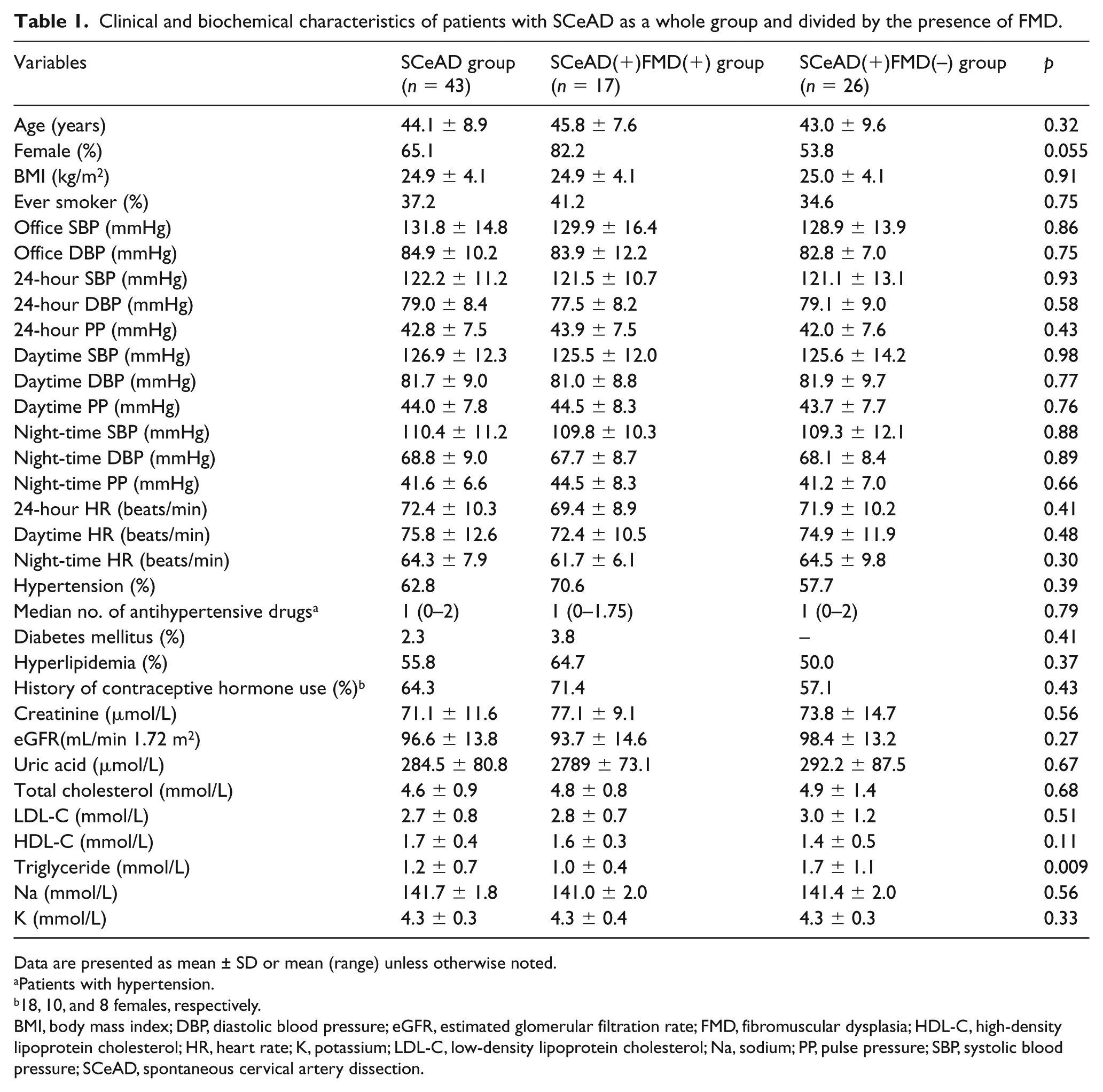
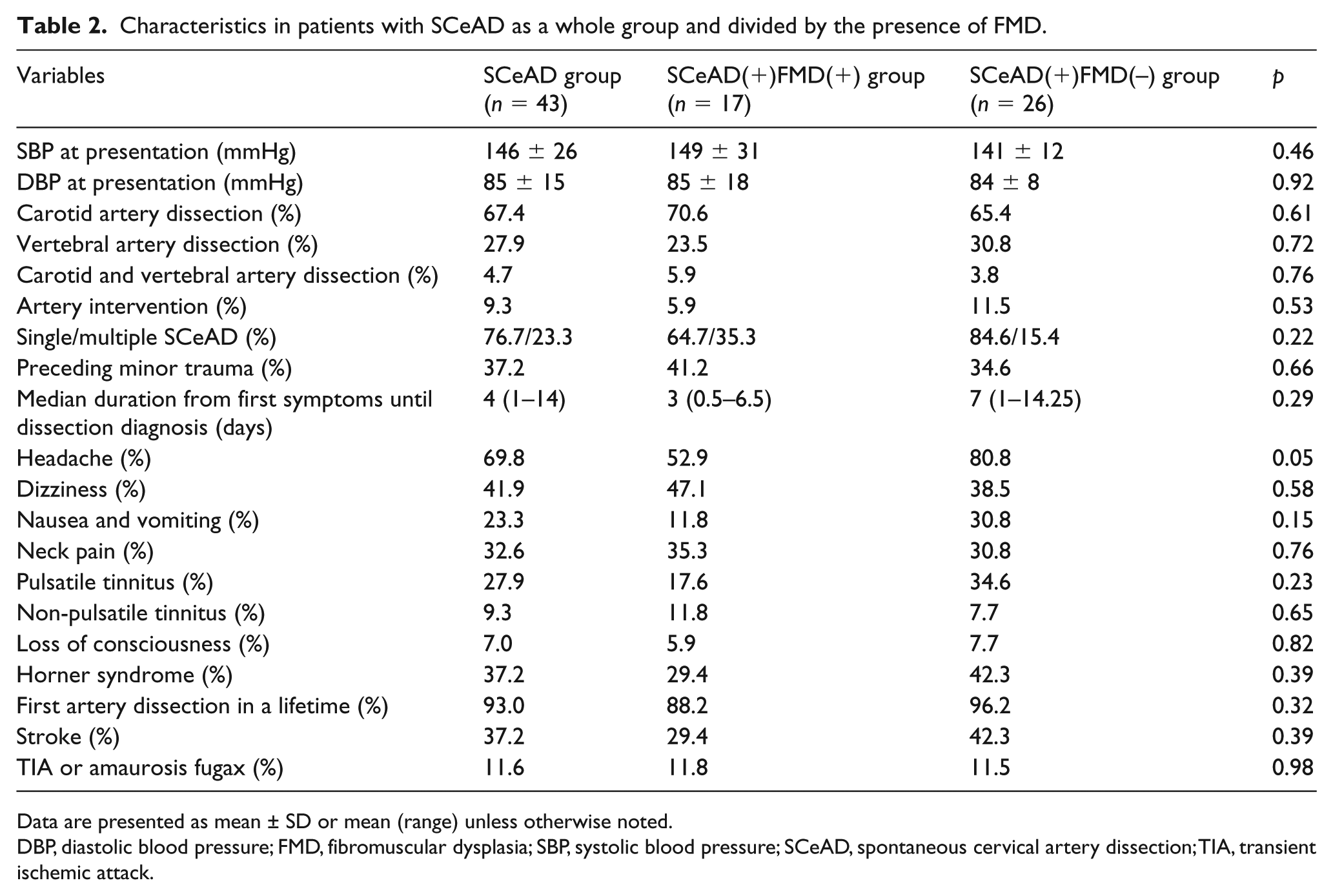
Patients with SCeAD were divided into two groups based on the presence or absence of FMD in any vascular bed – patients with SCeAD and FMD: SCeAD(+)FMD(+) (n = 17); patients with SCeAD without FMD: SCeAD(+)FMD(–) (n = 26). There were no differences in clinical characteristics between the SCeAD(+)FMD(+) and SCeAD(+)FMD(–) groups, except for a tendency towards a higher female ratio in the SCeAD(+)FMD(+) group (Table 1). The SCeAD(+)FMD(–) group was characterized by a higher left ventricular mass index (LVMI) compared to the SCeAD(+)FMD(+) group (Supplementary Table 3). There were no differences in other parameters describing target organ damage between the two groups. There were also no differences in parameters describing SCeAD characteristics, including event presentation and frequency of cerebral ischemia in the SCeAD(+)FMD(+) and SCeAD(+)FMD(–) groups (Table 2). In patients with SCeAD, we observed significant improvement both in NIHSS score (median 4 vs 1; p = 0.001) and in Rankin Scale score (median 1 vs 0; p = 0.002) at 3 months as compared to baseline. There were no differences in both scores between the SCeAD(+)FMD(+) and SCeAD(+)FMD(–) groups at baseline and at 3 months. In both groups, SCeAD events were more frequent in cold months (autumn and winter) than warm months (spring and summer) (Figure 2).
Clinical and biochemical characteristics of patients with SCeAD as a whole group and divided by the presence of FMD.
Data are presented as mean ± SD or mean (range) unless otherwise noted.
Patients with hypertension.
18, 10, and 8 females, respectively.
BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FMD, fibromuscular dysplasia; HDL-C, high-density lipoprotein cholesterol; HR, heart rate; K, potassium; LDL-C, low-density lipoprotein cholesterol; Na, sodium; PP, pulse pressure; SBP, systolic blood pressure; SCeAD, spontaneous cervical artery dissection.
Characteristics in patients with SCeAD as a whole group and divided by the presence of FMD.
Data are presented as mean ± SD or mean (range) unless otherwise noted.
DBP, diastolic blood pressure; FMD, fibromuscular dysplasia; SBP, systolic blood pressure; SCeAD, spontaneous cervical artery dissection; TIA, transient ischemic attack.
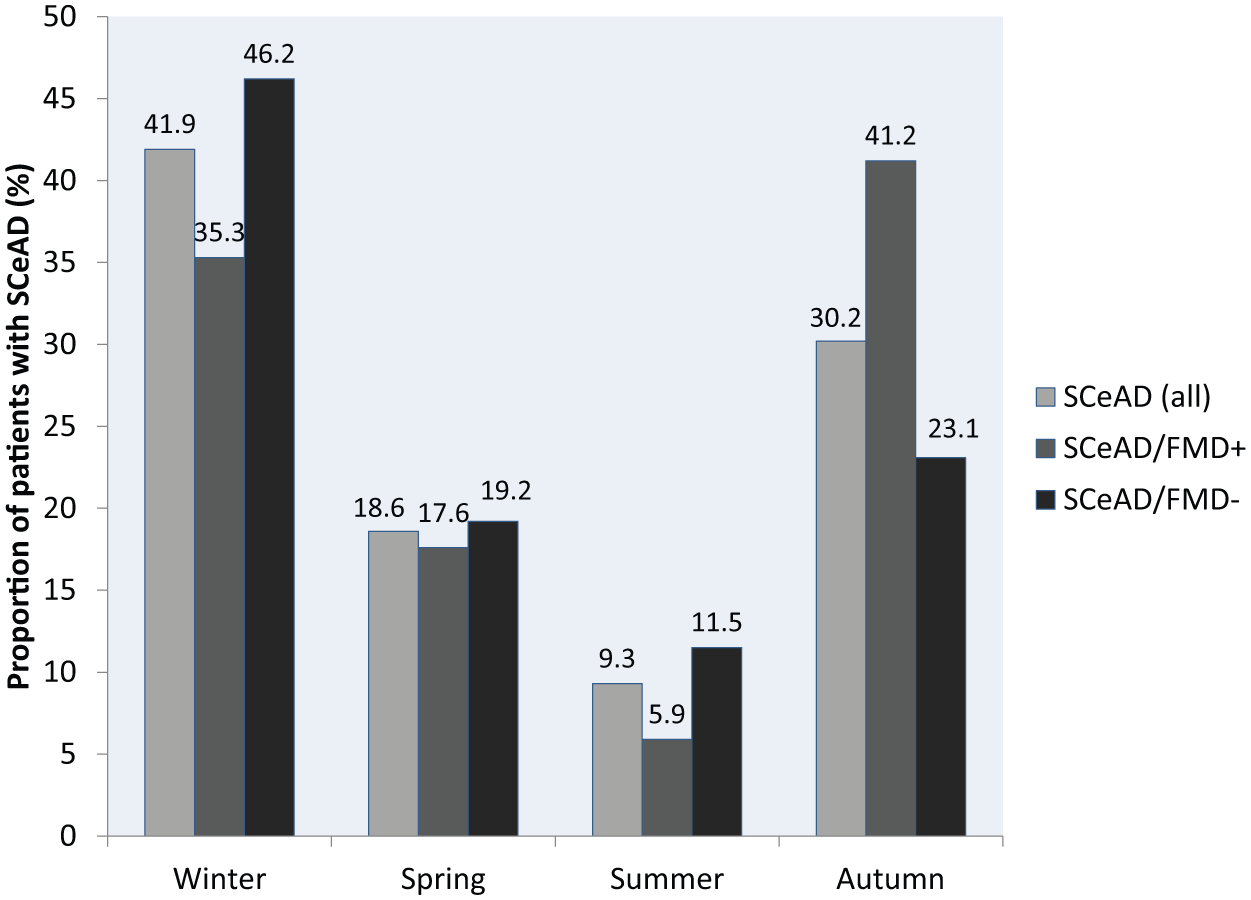
Seasonal variation in the occurrence of SCeAD.
We also compared the SCeAD(+)FMD(+) group to patients with FMD and no history of SCeAD and no SCeAD on current CTA of cervical arteries: SCeAD(–)FMD(+).
Patients in the SCeAD(+)FMD(+) group, as compared to the SCeAD(–)FMD(+) group, were characterized by a lower frequency of hypertension and lower (median) antihypertensive drug use but a higher frequency of hyperlipidemia and history of contraceptive hormone use (Supplementary Table 4). There were also no differences in parameters describing subclinical target organ damage in the SCeAD(+)FMD(+) and SCeAD(+)FMD(–) groups (data not shown). Patients in the SCeAD(+)FMD(+) group were characterized by a higher frequency of FMD in carotid or vertebral arteries and by a lower frequency of FMD in renal arteries as compared to the SCeAD(–)FMD(+) group (Table 3). No differences were found in the frequency of multifocal FMD, number of aneurysms, or involvement of two and more vascular beds between the compared groups.
FMD characteristics with or without history of SCeAD.
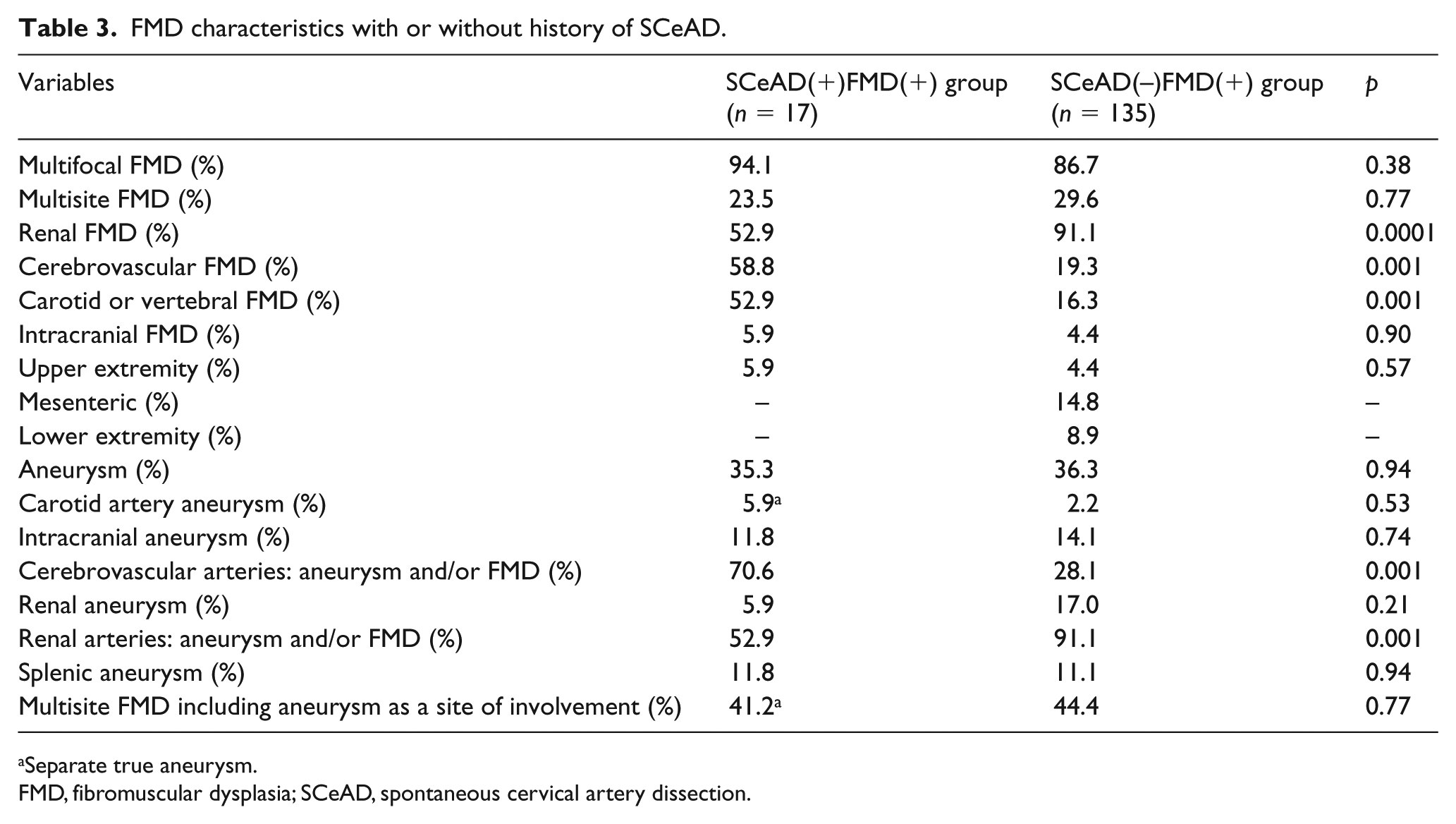
Separate true aneurysm.
FMD, fibromuscular dysplasia; SCeAD, spontaneous cervical artery dissection.
Discussion
To the very best of our knowledge, the ongoing ARCADIA-POL is the first study to systematically analyze the frequency of FMD in various vascular beds in subjects with SCeAD. One of the most important findings of our study was to document that, in evaluated patients, the frequency of FMD was higher than previously reported and was found in 39.5% of subjects with SCeAD.
The association between FMD and cervical (carotid and vertebral) artery dissection has been recognized.1,2 The association between SCeAD and FMD and its risk factors may indicate that both conditions reflect generalized arteriopathy. This may also suggest that impairment of stability of the arterial wall is involved in the pathogenesis of SCeAD.1–3,13
It is difficult to compare the frequency of FMD in patients with SCeAD in our study to previous reports. First, in the reports published so far, the frequency of FMD in patients with SCeAD ranged from 5.6% to 14%8,14–20; however, in these studies, only cerebrovascular arteries were evaluated. In our study, the frequency of cerebrovascular FMD in patients with SCeAD was higher (23.3%). Second, FMD in other vascular territories was not systemically assessed in those reports. In two studies, FMD in renal arteries was evaluated angiographically in some patients.15,18 Therefore, to the best of our knowledge, the present study is the first to systematically evaluate patients with SCeAD for FMD in vascular beds other than cerebrovascular arteries, revealing FMD in renal arteries in 20.9% of patients with SCeAD.
On the other hand, the rate of patients with a history of SCeAD among FMD patients in the ARCADIA-POL cohort (17 out of 152, 11%) is lower than reported in the US Registry (19%). This might be explained by the different referral pattern and higher rate of patients with cerebrovascular FMD presentation included in the US Registry. 21
Bejot and colleagues reported that FMD was more frequent in patients with multiple SCeAD as compared to single SCeAD. 14 Also in the US Registry, multiple SCeAD was common in patients with FMD. 21 In our study, multiple SCeAD in patients with FMD was more than twice that observed in patients without FMD, but this difference was not significant, most likely due to the small sample size.
The demographics of our patient population indicate that mean age at the time of the initial dissection was 44.1 years, which is similar to those found in other reports showing a distinct peak in the fifth decade of life. No difference in age at the time of SCeAD diagnosis was found between patients with and without FMD.1–3,22–24
In contrast to previous studies, patients with SCeAD in our study were more often women, and there was a tendency towards a higher rate of women in the SCeAD(+)FMD(+) group compared to the SCeAD(+)FMD(–) group. In a North American population-based study, and in two large hospital-based CAD series, 50–52% of the patients were women, whereas a slight predominance in men was reported in the European multicenter hospital-based series (53–57%).20,24,25 This difference is difficult to explain. Although selection bias cannot be ruled out, the referring neurology centers were asked to refer all consecutive patients. It should be also noted that in patients with SCeAD, a vast female predominance has been reported. 26
In our study, the incidence of hypertension was higher than in other reports but there was no difference in the rate of hypertension between patients with SCeAD and with or without FMD. This may be explained by the fact that ABPM was performed in all patients, allowing better characterization of blood pressure (BP) levels as compared with previous studies, which were based only on office BP measurements. A higher prevalence of hypertension in patients with FMD without SCeAD as compared to those with SCeAD might be partially explained by the differences in FMD distribution (less frequent renal involvement in the latter).
In patients with SCeAD, the most common clinical presentation was headache, dizziness, Horner syndrome, neck pain, and pulsatile tinnitus. Still, cerebral ischemic events, including stroke and transient ischemic attack (TIA) or amaurosis fugax, occurred in 37.2% and 11.6% of patients, respectively. Most patients with SCeAD have at least two symptoms, although symptoms may occur in isolation, and some dissections may remain asymptomatic.
There was no difference in the clinical presentation of SCeAD between patients with and without FMD, except for a higher frequency of headaches in patients without FMD compared to patients with FMD. Of note, the incidence of stroke, the most serious SCeAD manifestation, was relatively lower than in previously reported SCeAD cohorts. This difference is difficult to explain and might be related, among other factors, to geographic differences and/or underdiagnosis of SCeAD.
Our study also documented that, in our group of patients with SCeAD, recurrent dissection within the first 3 months did not occur in any of the subjects. We observed significant improvement in NIHSS and Rankin Scale scores in the 3-month follow-up. All subjects received medical therapy (antiplatelet therapy) according to current recommendations at the discretion of the treating facility. 27
Our patients were characterized by a relatively high incidence of smokers, hypertension, hyperlipidemia, and the use of oral contraceptives, which remains in accordance with other reports, suggesting the potential link between SCeAD and common risk factors for vascular disease. No differences in those factors or in the indices of target organ damage were found between patients with SCeAD and FMD and those without FMD.
The present study showed mild seasonal variation in the occurrence of SCeAD, with a peak in autumn and winter. Our results are in agreement with other studies indicating that SCeAD occurs more frequently in cooler months regardless of the geographical location, suggesting that transient seasonal causes may be important in the underlying pathophysiology.1,28,29 Of note, this relationship was slightly more pronounced for the internal carotid artery compared to the vertebral artery, suggesting different triggering mechanisms for these two dissection sites.28,29 The reported seasonal pattern has been mainly attributed to an increased occurrence of infection and weather-related changes in BP, coagulation parameters, and physical activity, which have been postulated as triggers.1,28–30 None of the evaluated patients in the present study reported febrile infection preceding SCeAD.
There are little data concerning the characteristics of patients with FMD and SCeAD. Recently, Kadian-Dodov et al. compared patients with FMD and dissection of any artery (including cervical: 37.2% of patients in this group) to patients with FMD and no history of dissection. Patients with dissection were younger at presentation and had a lower prevalence of hypertension. There was a tendency towards a higher prevalence of history of contraceptive hormone use in patients with FMD and dissection as compared to those without dissection. 21 In our study, although hypertension was less prevalent among patients with FMD and SCeAD as compared to those without SCeAD, there were no differences in office BP and ABPM levels. Of note, patients with FMD and SCeAD were characterized by a higher frequency of hyperlipidemia and lower triglycerides levels (which might be explained by more common treatment in this group).
Our results also showed a relatively high rate of aneurysms (35.3%), including intracranial aneurysms (11.8%) in patients with SCeAD and FMD. There is growing evidence that FMD patients are characterized by a high frequency of vascular complications including presence of aneurysms. Kadian-Dodov et al. reported that aneurysms were present in 21.7% of patients with FMD, and that intracranial aneurysms were the third most common after renal and carotid aneurysms. 21 In the ARCADIA-POL Registry, aneurysms were present in 26% of patients. Intracranial aneurysms were found in 6% of patients with FMD, mostly characterized by the presence of FMD in extracranial cervical arteries. 31 Therefore, our study strengthens previous data showing that, in patients with FMD, intracranial aneurysms might be relatively frequent and might be related to FMD or dissection of extracranial cervical arteries.
Strengths and limitations
A strength of our study is that ARCADIA-POL is the first to systematically analyze the frequency of FMD in various vascular beds in subjects with SCeAD, which enabled us to obtain significant results over a relatively short time. In addition, all subjects had a 3-month follow-up after referral for SCeAD.
There was a relatively small number of patients with SCeAD in our study but, on the other hand, each of the participants of the ARCADIA-POL study were subjected to a detailed clinical investigation.
Because of the low incidence of SCeAD in the general population, we had to include patients from six different centers representing only university hospitals. It is difficult to determine if our results are representative for patients with SCeAD in the general population. Selection bias may have occurred; however, collaborating neurological centers referred consecutive patients. The lower frequency of stroke in our series as compared to other series of SCeAD patients may be partially explained by the fact that SCeAD is probably recognized more frequently than in the past. Since multi-modality imaging is more available and more frequently performed than in the past, SCeAD is diagnosed more frequently in patients with presentations other than stroke.
Conclusions
Our study indicates a high frequency (39.5%) of FMD in patients with SCeAD. There are no distinctive discriminating factors between patients with SCeAD with and without FMD, so FMD should be suspected in all patients with SCeAD. Our data support performing CTA or MRI from head-to-pelvis for FMD screening and associated aneurysm/dissection in patients with SCeAD.
Moreover, there were no distinctive features characterizing patients with FMD and SCeAD from patients with FMD with no history of this serious vascular complication; however, our study might lack power to detect the differences. Future studies should be focused on identifying risk factors for SCeAD in patients with FMD.
Supplemental Material
10.1177_1358863X18811596_Supplementary_material_table1 – Supplemental material for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study
Supplemental material, 10.1177_1358863X18811596_Supplementary_material_table1 for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study by Paulina Talarowska, Piotr Dobrowolski, Anna Klisiewicz, Anna Kostera-Pruszczyk, Anna Członkowska, Iwona Kurkowska-Jastrzębska, Dariusz Gąsecki, Ewa Warchoł-Celińska, Łukasz Światłowski, Elżbieta Florczak, Magdalena Januszewicz, Ilona Michałowska, Katarzyna Józwik-Plebanek, Piotr Szczudlik, Beata Błażejewska-Hyżorek, Marcin Protasiewicz, Piotr Odrowąż-Pieniążek, Łukasz Tekieli, Katarzyna Michel-Rowicka, Katarzyna Hanus, Krystyna Widecka, Marta Sołtysiak, Andrzej Tykarski, Łukasz Stryczyński, Małgorzata Szczerbo-Trojanowska, Piotr Hoffman, Aleksander Prejbisz and Andrzej Januszewicz in Vascular Medicine
Supplemental Material
10.1177_1358863X18811596_Supplementary_material_table2 – Supplemental material for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study
Supplemental material, 10.1177_1358863X18811596_Supplementary_material_table2 for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study by Paulina Talarowska, Piotr Dobrowolski, Anna Klisiewicz, Anna Kostera-Pruszczyk, Anna Członkowska, Iwona Kurkowska-Jastrzębska, Dariusz Gąsecki, Ewa Warchoł-Celińska, Łukasz Światłowski, Elżbieta Florczak, Magdalena Januszewicz, Ilona Michałowska, Katarzyna Józwik-Plebanek, Piotr Szczudlik, Beata Błażejewska-Hyżorek, Marcin Protasiewicz, Piotr Odrowąż-Pieniążek, Łukasz Tekieli, Katarzyna Michel-Rowicka, Katarzyna Hanus, Krystyna Widecka, Marta Sołtysiak, Andrzej Tykarski, Łukasz Stryczyński, Małgorzata Szczerbo-Trojanowska, Piotr Hoffman, Aleksander Prejbisz and Andrzej Januszewicz in Vascular Medicine
Supplemental Material
10.1177_1358863X18811596_Supplementary_material_table3 – Supplemental material for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study
Supplemental material, 10.1177_1358863X18811596_Supplementary_material_table3 for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study by Paulina Talarowska, Piotr Dobrowolski, Anna Klisiewicz, Anna Kostera-Pruszczyk, Anna Członkowska, Iwona Kurkowska-Jastrzębska, Dariusz Gąsecki, Ewa Warchoł-Celińska, Łukasz Światłowski, Elżbieta Florczak, Magdalena Januszewicz, Ilona Michałowska, Katarzyna Józwik-Plebanek, Piotr Szczudlik, Beata Błażejewska-Hyżorek, Marcin Protasiewicz, Piotr Odrowąż-Pieniążek, Łukasz Tekieli, Katarzyna Michel-Rowicka, Katarzyna Hanus, Krystyna Widecka, Marta Sołtysiak, Andrzej Tykarski, Łukasz Stryczyński, Małgorzata Szczerbo-Trojanowska, Piotr Hoffman, Aleksander Prejbisz and Andrzej Januszewicz in Vascular Medicine
Supplemental Material
10.1177_1358863X18811596_Supplementary_material_table4 – Supplemental material for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study
Supplemental material, 10.1177_1358863X18811596_Supplementary_material_table4 for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study by Paulina Talarowska, Piotr Dobrowolski, Anna Klisiewicz, Anna Kostera-Pruszczyk, Anna Członkowska, Iwona Kurkowska-Jastrzębska, Dariusz Gąsecki, Ewa Warchoł-Celińska, Łukasz Światłowski, Elżbieta Florczak, Magdalena Januszewicz, Ilona Michałowska, Katarzyna Józwik-Plebanek, Piotr Szczudlik, Beata Błażejewska-Hyżorek, Marcin Protasiewicz, Piotr Odrowąż-Pieniążek, Łukasz Tekieli, Katarzyna Michel-Rowicka, Katarzyna Hanus, Krystyna Widecka, Marta Sołtysiak, Andrzej Tykarski, Łukasz Stryczyński, Małgorzata Szczerbo-Trojanowska, Piotr Hoffman, Aleksander Prejbisz and Andrzej Januszewicz in Vascular Medicine
Supplemental Material
10.1177_1358863X18811596_Supplementary_material_text – Supplemental material for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study
Supplemental material, 10.1177_1358863X18811596_Supplementary_material_text for High incidence and clinical characteristics of fibromuscular dysplasia in patients with spontaneous cervical artery dissection: The ARCADIA-POL study by Paulina Talarowska, Piotr Dobrowolski, Anna Klisiewicz, Anna Kostera-Pruszczyk, Anna Członkowska, Iwona Kurkowska-Jastrzębska, Dariusz Gąsecki, Ewa Warchoł-Celińska, Łukasz Światłowski, Elżbieta Florczak, Magdalena Januszewicz, Ilona Michałowska, Katarzyna Józwik-Plebanek, Piotr Szczudlik, Beata Błażejewska-Hyżorek, Marcin Protasiewicz, Piotr Odrowąż-Pieniążek, Łukasz Tekieli, Katarzyna Michel-Rowicka, Katarzyna Hanus, Krystyna Widecka, Marta Sołtysiak, Andrzej Tykarski, Łukasz Stryczyński, Małgorzata Szczerbo-Trojanowska, Piotr Hoffman, Aleksander Prejbisz and Andrzej Januszewicz in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was funded by a research grant from the Institute of Cardiology, Warsaw, Poland (no. 2.46/VII/15).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.