
Abstract
Fibromuscular dysplasia (FMD), a non-inflammatory arterial disease, may lead to renovascular hypertension (HTN) and cerebrovascular disease. Little is known about medication use in FMD. Clinical features and medication use were reviewed in a national FMD registry (12 US sites). Medication usage was assessed in raw and adjusted analyses. Covariates included demographic characteristics, co-morbid conditions and vascular bed involvement. A total of 874 subjects (93.6% female) were included in the analysis. Mean age was 55.6±13.1 years, 74.5% had HTN, 25.4% had a history of transient ischemic attack or stroke, and 7.5% had a history of coronary artery disease (CAD). Renal and cerebrovascular arteries were affected in 70.4% and 74.7%, respectively. Anti-platelet agents were administered to 72.9% of patients. In multivariate analyses, factors associated with a greater likelihood of anti-platelet agent use were older age (OR=1.02 per year, p=0.005), CAD (OR=3.76, p=0.015), cerebrovascular artery FMD involvement in isolation (OR=2.31, p<0.0001) or a history of previous intervention for FMD (OR=1.52, p=0.036). A greater number of anti-HTN medications was evident in isolated renal versus isolated cerebrovascular FMD patients. Factors associated with a greater number of anti-HTN medications were older age (OR=1.03 per year, p<0.0001), history of HTN (OR=24.04, p<0.0001), history of CAD (OR=2.71, p=0.0008) and a history of a previous therapeutic procedure (OR=1.72, p=0.001). In conclusion, in FMD, medication use varies based on vascular bed involvement. Isolated renal FMD patients receive more anti-HTN agents and there is greater anti-platelet agent use among patients with cerebrovascular FMD. Further studies correlating medication use in FMD with clinically meaningful patient outcomes are necessary.
Background
Fibromuscular dysplasia (FMD) is a non-inflammatory, non-atherosclerotic arterial disease that most commonly occurs in women aged 20 to 60 years.1,2 FMD has been described in men, children and the elderly. 3 According to the United States Registry for Fibromuscular Dysplasia, renal arteries are affected in 79% and the extracranial carotid arteries in 74% of patients with FMD. 1
While FMD may present with non-specific symptoms, discovered after investigating a bruit heard over an artery or, less commonly, discovered incidentally on imaging studies, 4 hypertension (HTN) remains the most frequently recognized symptom in patients with FMD. It is also the most common reason for percutaneous endovascular intervention. FMD is known to be a cause of secondary and/or resistant HTN. Cerebrovascular involvement in FMD is also common and stroke is a potential consequence, resulting most typically from carotid or vertebral artery dissection. 5
There is limited information in the medical literature regarding anti-hypertensive and anti-platelet medication use in patients with FMD. It is conventional to prescribe aspirin to asymptomatic patients.4,6 However, there is currently no report of actual practice patterns in those with FMD. Additionally, the utilization of anti-hypertensive medications among patients with FMD has not been characterized. 7 Recent publications recommend following the Joint National Committee guidelines for patients with HTN. 8 Additional factors, such as prior endovascular intervention and the presence of polyvascular disease, may influence patterns of medication use in FMD patients. The impact of these and other factors have thus far not been examined in a large multi-institutional cohort. While such an analysis may be impacted by referral and screening bias, the present study was conducted in order to describe medication use in FMD patients and identify factors that may be associated with differing patterns of use.
Methods
The United States Registry for Fibromuscular Dysplasia is a multicenter national registry enrolling patients with FMD. It was created to better define the epidemiology of FMD, assess practice patterns, and provide a framework for clinical outcomes research in FMD. As of October 2014, the registry included 1008 FMD patients recruited from 12 clinical centers. Further details of the registry have been published previously. 1 For the purposes of this analysis, 874 subjects for whom information was available for both anti-platelet and anti-HTN medications were included.
As histopathology is rarely available (owing to the large majority of patients either being treated medically or with an endovascular procedure), the diagnosis of FMD is made almost exclusively on the basis of anatomic (invasive or non-invasive) imaging. Trained abstractors using a clinical research form and standardized definitions obtained data included in the registry. The registry was approved by each of the 12 participating institutions’ Institutional Review Boards. In addition, a Data Use Agreement was signed between participating institutions and the coordinating center (Michigan Cardiovascular Outcomes Research and Reporting Program, MCORRP) to ensure appropriate use of data obtained.
The current analysis included baseline demographic characteristics as collected during the time of enrollment (age, gender, race), co-morbid conditions (HTN, hyperlipidemia, impaired renal function and tobacco abuse), past medical history (coronary artery disease (CAD), intermittent claudication, any neurological event, venous thromboembolism), FMD vascular bed involvement (renal, cerebrovascular, mesenteric, lower extremity, upper extremity, aorta), medication use, and endovascular and open surgical procedures occurring prior to the baseline encounter. Blood pressure measurements were collected during the enrollment visit. If blood pressure measurements were available from both arms, an average measurement was used. Cerebrovascular involvement was defined as FMD of the extracranial carotid arteries, intracranial arteries and/or vertebral arteries. Tobacco history was defined as an aggregate of current or former use. A symptomatic neurological event was defined as any of the following, alone or in conjunction: prior transient ischemic attack (TIA), stroke, amaurosis fugax or Horner’s syndrome. Anti-platelet medication was defined as aspirin and/or clopidogrel. A physical examination was performed at the time of initial enrollment in the registry, including documentation of resting bilateral arm blood pressures.
Statistical analysis
Descriptive statistics were used to report the prevalence of anti-HTN and anti-platelet medication use in the cohort. Between-group differences in patient characteristics were evaluated by using the chi-squared and Fisher’s exact tests for categorical variables, t-tests and Wilcoxon rank sum tests for continuous variables. Logistic regression was used to create statistic models. From a list of covariates of clinical interest, significant covariates from the univariate analysis were tested for independent significance by stepwise selection with multivariate logistic regression. We then constructed models with a mindset that we wanted to include the covariates of most clinical interest and also to achieve satisfactory statistical significance and appropriateness. Binary and unordered multinomial models were fit on the dependent variables related to anti-platelet use. Covariates that remained in the final models to assess associations of anti-platelet medication use were age, CAD, vascular bed involvement (renal and cerebrovascular arteries) and a previous therapeutic vascular procedure. Cumulative logit models were implemented in the analysis of the use of anti-HTN agents. The number of anti-HTN agents was divided into five levels: none, 1, 2, 3, and 4 or more. Covariates that remained in the final model were age, HTN, CAD, vascular bed involvement (renal and cerebrovascular arteries) and a previous therapeutic vascular procedure. A two-sided p-value less than 0.05 was considered statistically significant.
Results
Data were available for 874 patients (93.6% female). The mean age was 55.6±13.1 years, 74.5% had HTN, 25.4% had a history of stroke/TIA and 7.5% had a history of CAD. Renal and cerebrovascular artery involvement with FMD was present in 70.4% and 74.7% of patients, respectively (Table 1).
Cohort characteristics (n = 874 FMD patients).
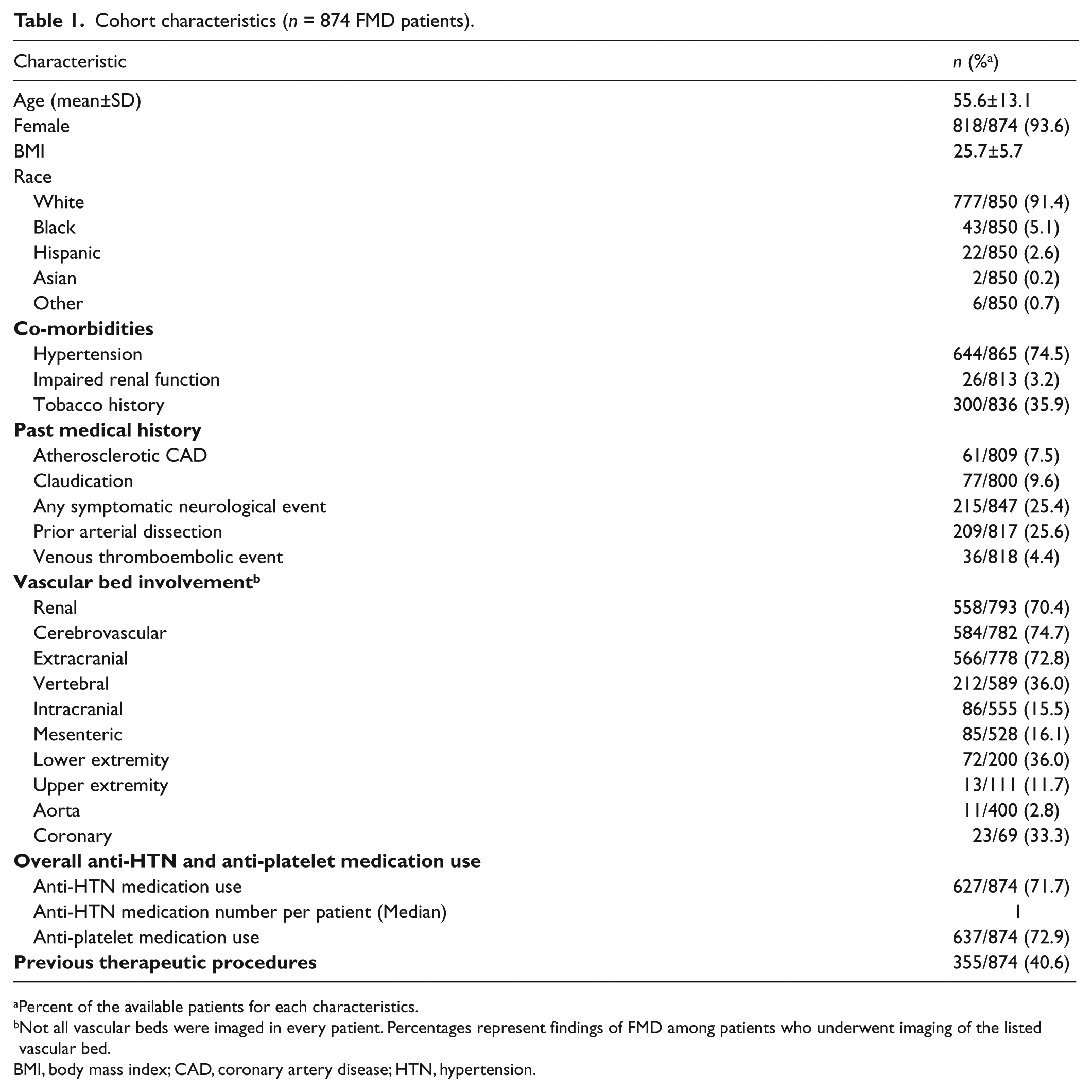
Percent of the available patients for each characteristics.
Not all vascular beds were imaged in every patient. Percentages represent findings of FMD among patients who underwent imaging of the listed vascular bed.
BMI, body mass index; CAD, coronary artery disease; HTN, hypertension.
Blood pressure and anti-HTN medication use
Mean systolic blood pressure (SBP) was 133.1±20.7 mmHg and mean diastolic blood pressure (DBP) was 75.8±12.3 mmHg. Of 822 patients who had values for both SBP and DBP, 529 (64.4%) had both SBP <140 mmHg and DBP <90 mmHg. Patients with isolated renal artery FMD had a higher SBP (135.7±23.2 vs 129.3±17.1 mmHg, p=0.002) and DBP (78.2±13.0 vs 74.0±10.4 mmHg, p=0.0004) than patients with isolated cerebrovascular FMD. Patients with isolated renal artery FMD had a higher DBP (78.2±13.0 vs 75.6±11.8 mmHg, p=0.02) but not SBP (135.7±23.2 vs 133.1±19.7 mmHg, p=0.22) than patients with both renal and cerebrovascular involvement.
Overall, anti-HTN medications were administered to 71.7% of patients in this cohort. The median number of medications patients received was one, and 21.5% of patients received three or more anti-HTN medications. The most commonly used agents were beta-blockers (40.0%), diuretics (31.3%) and calcium channel antagonists (25.7%). A total of 21.0% of patients received only an angiotensin converting enzyme (ACE) inhibitor, 21.6% received only an angiotensin receptor blocking agent (ARB), and 0.8% received both. Anti-HTN medication patterns differed between vascular beds involved with FMD (Figure 1). More patients with isolated renal artery FMD received an anti-HTN medication than patients with isolated cerebrovascular artery involvement (87.1% vs 52.8%, p<0.0001). Furthermore, the proportion of patients who were receiving three or more anti-HTN medications was significantly higher in patients with isolated renal artery as compared to isolated cerebrovascular FMD (31.4% vs 9.6%, p<0.0001). Also, in nearly each anti-HTN medication type, a greater proportion of patients with renal artery FMD (both in isolation and with cerebrovascular FMD) were receiving them as compared to patients with isolated cerebrovascular disease (Figure 2).
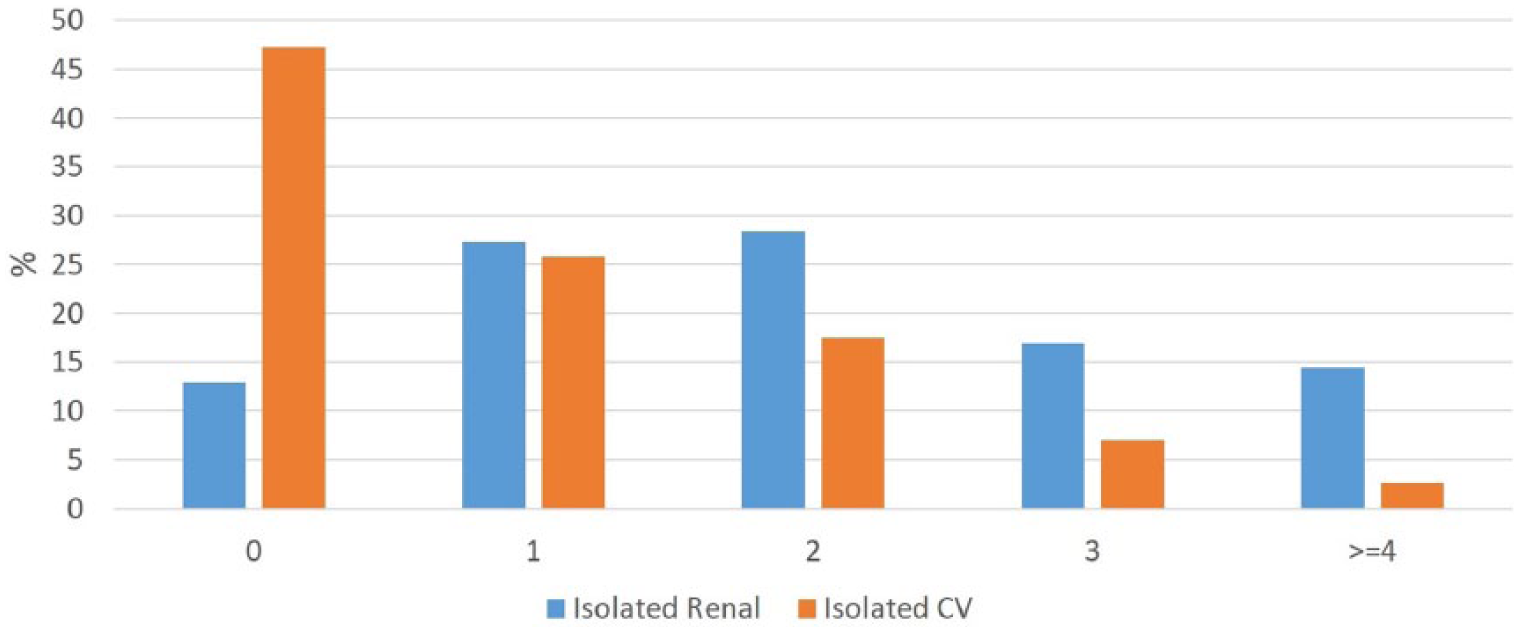
Anti-HTN medication number in FMD patients according to vascular bed involvement. Overall p <0.0001. (CV, cerebrovascular.)
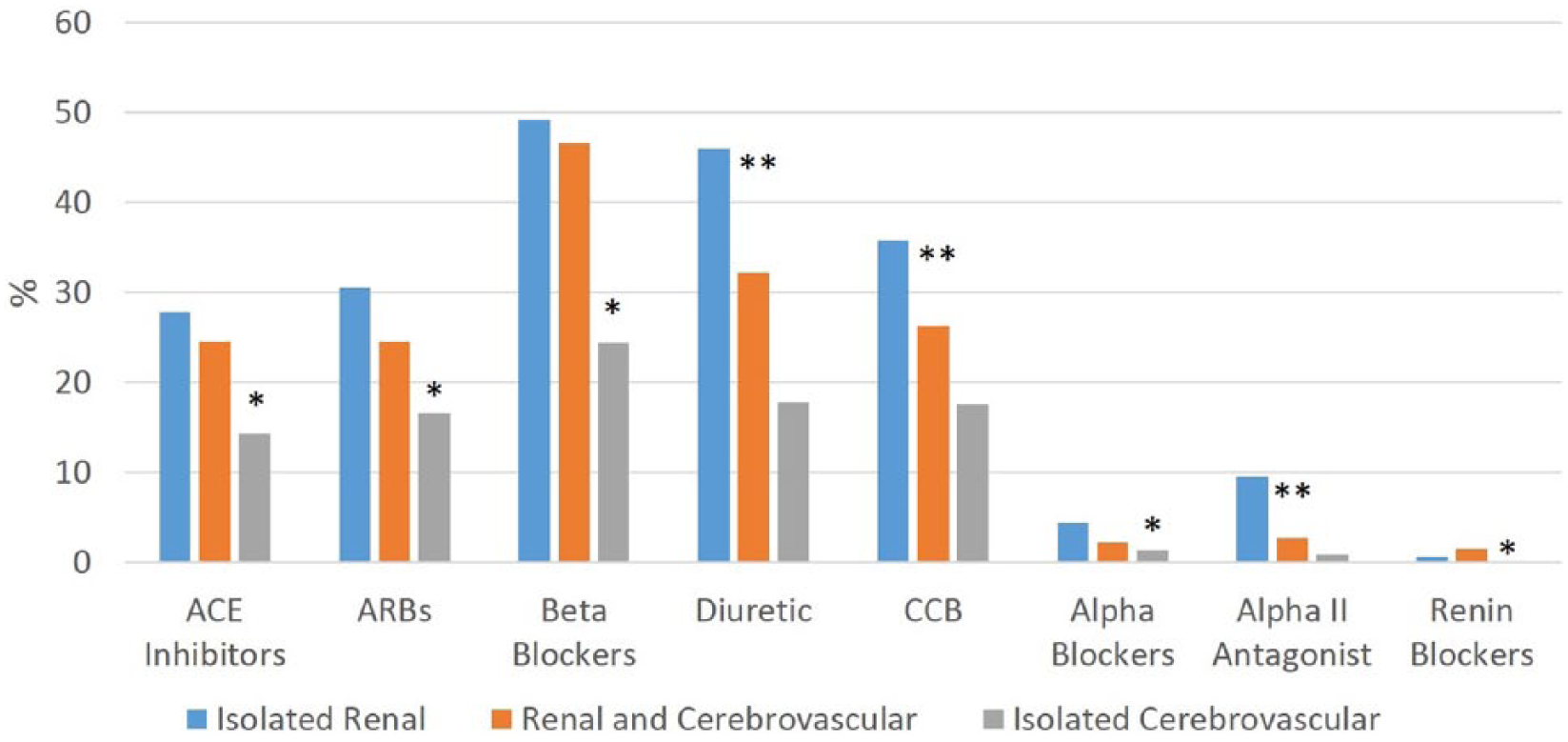
Anti-HTN medication class distribution in FMD patients according to vascular bed. (*Significant difference between isolated cerebrovascular involvement and isolated renal artery involvement only; **significant difference between isolated renal involvement and both isolated cerebrovascular artery and renal artery and cerebrovascular involvement. ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; CCB, calcium channel blockers.)
Compared to patients who did not receive any anti-HTN medication, patients receiving these medications were older (57.0±13.3 vs 52.2±11.7 years, p<0.0001), more likely to have HTN (91.6% vs 30.5%, p<0.0001), more likely to have renal artery involvement (78.3% vs 48.8%, p<0.0001) and had a higher likelihood of a history of an FMD-related interventional procedure (45.9% vs 27.1%, p<0.0001) (Table 1S). Patients with a history of a symptomatic neurological event (23.5% vs 30.1%, p=0.042) or cerebrovascular FMD (68.7% vs 88.8%, p<0.0001) had a lower likelihood of receiving anti-HTN medications.
In the logistic regression model (Table 2), factors associated with a greater number of anti-HTN medications were increasing age (odds ratio (OR)=1.03 for each additional year, p<0.0001), body mass index (OR=1.06, p<0.0001), history of HTN (OR=24.04, p<0.0001), history of CAD (OR=2.71, p=0.0008), impaired renal function (OR=3.04, p=0.018) and history of a vascular procedure (OR=1.72, p=0.001). Patients receiving anti-platelet medications were not more likely to receive anti-HTN medications (71.3% vs 73.0%, p=0.67) (Table 2S).
Cumulative logit model for number of anti-hypertension medications a .
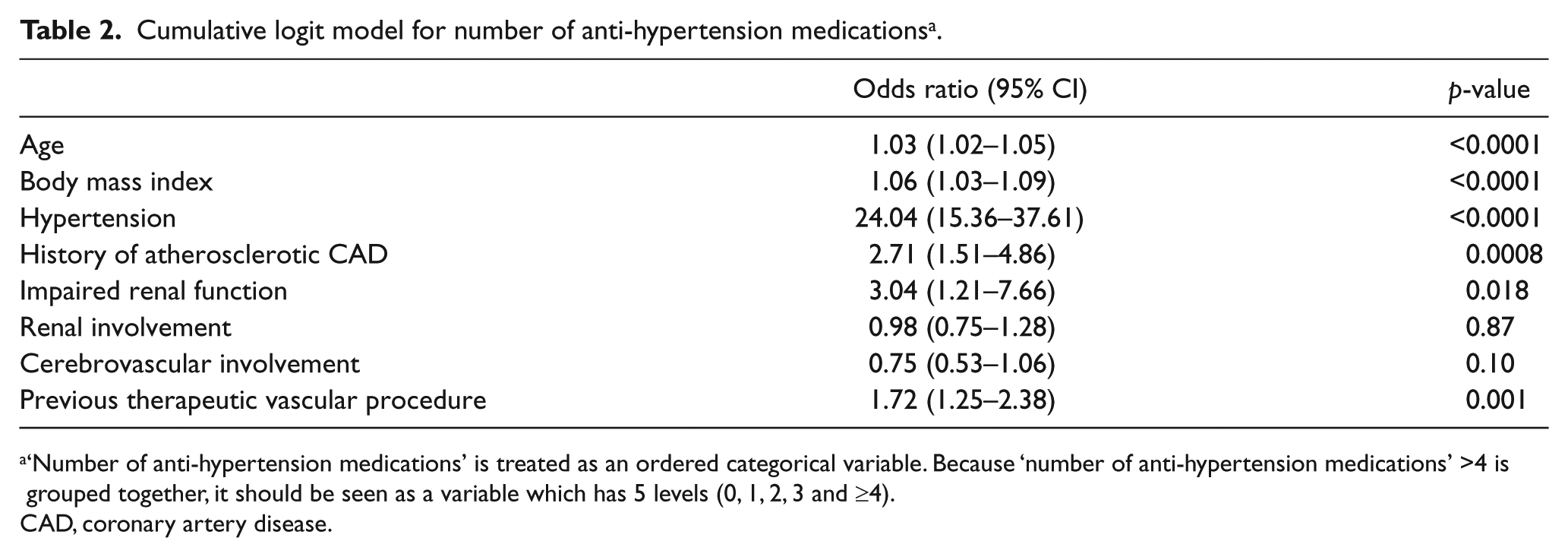
‘Number of anti-hypertension medications’ is treated as an ordered categorical variable. Because ‘number of anti-hypertension medications’ >4 is grouped together, it should be seen as a variable which has 5 levels (0, 1, 2, 3 and ≥4).
CAD, coronary artery disease.
Anti-platelet agent use
Overall, 56.8% of patients received aspirin alone, while 4.6% received clopidogrel only and 72.9% received any anti-platelet medication. An anti-platelet agent was administered in 64.4% and 82.1% of patients with isolated renal artery or isolated cerebrovascular FMD involvement, respectively, p<0.0001.
In unadjusted analyses (Table 3S), compared to patients who were not receiving an anti-platelet agent, patients receiving an anti-platelet agent were: older (56.6±12.6 vs 53.0±13.8 years, p=0.0002), had a lower prevalence of HTN (72.0% vs 81.0%, p=0.007), had a higher prevalence of CAD (9.1% vs 3.5%, p=0.005), a higher prevalence of past neurological events (28.2% vs 18.0%, p=0.003) and a higher prevalence of prior arterial dissection (28.6% vs 17.7%, p=0.001). Also, patients receiving anti-platelet agents had more cerebrovascular involvement (78.4% vs 63.0%, p<0.0001), but less renal artery involvement (66.3% vs 80.9%, p<0.0001).
In the binary logit model (Table 3), the factors associated with a higher odds of taking an anti-platelet agent were: advancing age (OR=1.02 per each additional year, p=0.005), history of CAD (OR=3.76, p=0.015), cerebrovascular involvement of FMD (OR=2.31, p<0.0001) and a previous therapeutic vascular intervention (OR=1.52, p=0.036).
Binary logit model for associations of any anti-platelet agent use.
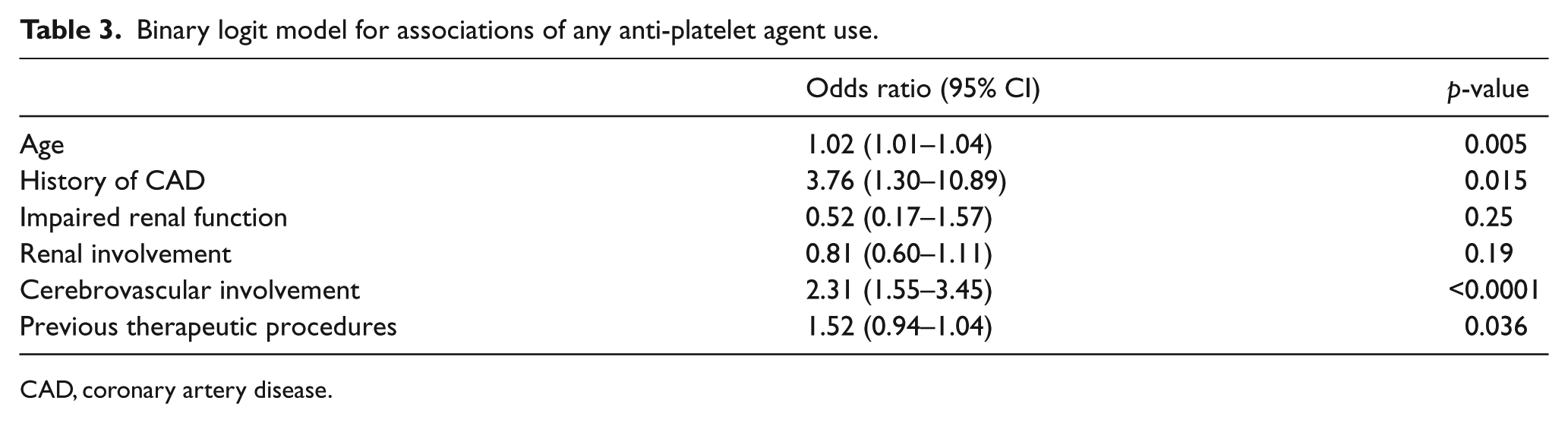
CAD, coronary artery disease.
In the unordered multinomial logit model (Table 4S), a past neurological event (OR=0.28, p=0.001) conferred a lower likelihood of taking aspirin rather than clopidogrel as a single agent. Patients who had a history of CAD (OR=2.32, p=0.027), a previous neurological event (OR=2.96, p<0.0001) or a previous interventional procedure (OR=2.84, p<0.0001) had a higher likelihood of receiving dual anti-platelet therapy than aspirin monotherapy. There were no differences between patients who received dual anti-platelet therapy and clopidogrel monotherapy.
Discussion
This study is the first to report medication-related practice patterns in a large cohort of patients with FMD. Anti-platelet and anti-HTN agent use was widespread. The likelihood of receiving both medications increased with age, a history of CAD and previous vascular intervention. However, there were also differences in administration patterns. Increasing anti-HTN medication use was also associated with body mass index, history of HTN and with impaired renal function, while anti-platelet medication use was also associated with cerebrovascular involvement of FMD.
There are no guidelines to aid clinicians in the treatment of HTN in patients with FMD. Current practice is to follow the Joint National Committee guidelines for the treatment of HTN. 8 For FMD patients with long-standing HTN in whom the diagnosis of FMD has been delayed, anti-HTN medications should be continued as long as blood pressure is well controlled and the patient does not experience undesirable medication-related side effects. 9 Furthermore, renal artery FMD may result in HTN but seldom results in renal dysfunction. 9 It follows that as in other patients with HTN, the primary goal in treating patients with renal artery FMD is the control of blood pressure to prevent the sequelae of long-standing poorly controlled HTN. 6 Although renal and cerebrovascular involvement in FMD is almost equal in prevalence, 1 anti-HTN medication administration patterns in this cohort differed between patients with renal artery and cerebrovascular involvement. Almost all of the patients with renal artery FMD received at least one anti-HTN medication, and the use of three or more anti-HTN medications was relatively common in renal artery FMD patients, yet quite rare in isolated cerebrovascular FMD patients. Furthermore, in the current study, patients with renal artery involvement received a greater proportion of nearly all classes of anti-HTN medications as compared to patients with isolated cerebrovascular involvement. The most commonly utilized classes of anti-HTN agents were beta-blockers, diuretics and calcium channel antagonists. Either an ACE-inhibitor or ARB was given in over 43% of the cohort, as can be expected in a patient population enriched with renal artery stenosis. 10 Associations of anti-HTN medication use in patients with FMD included HTN and CAD, similar to associations of these medications in patients without FMD. 11 Age was also an independent predictor of anti-HTN use, echoing the greater use of these agents in the aging population. 12
Anti-platelet agents are also logical to administer to patients with FMD, as blood flows through areas of stenosis interrupted by fibrous bands and areas of post-stenotic dilatation. 13 Accordingly, these agents have been recommended empirically to asymptomatic patients with FMD.6,14 Nonetheless, no study to date has examined anti-platelet agent use in patients with FMD and yet, in the current study, most patients received an anti-platelet agent. Anti-platelet agents are considered appropriate after vascular surgical or endovascular procedures in the general population. 15 Accordingly, patients who have had an invasive procedure were more likely to receive an anti-platelet agent. While a previous neurological event was associated with a relatively lower likelihood of aspirin compared to clopidogrel or dual-anti-platelet medication use, aspirin use was still much more prevalent, in absolute terms. This observation effectively deviates from best practice recommendations for non-FMD patients. While controversial, guidelines support the use of anti-platelet agents for patients who have suffered a TIA or stroke and clopidogrel is preferred to aspirin (level of recommendation 2B). 16 Interestingly, prior arterial dissection did not remain associated with anti-platelet medication use in the final model. It follows that there is a great need for additional research focused on optimal medical therapy among patients with FMD, especially clinical outcomes studies.
This study has limitations. There may be referral bias in that the most symptomatic of the FMD population or those who have had imaging studies or a vascular event may be more likely to be evaluated at one of the centers included in this registry. Also, medical treatment as presented in this study is representative of specialized FMD referral centers, and may not represent the treatment of these patients in general. It is quite feasible that medication utilization patterns differ outside of these FMD clinical centers. However, it is noteworthy that given the degree of uncertainty concerning FMD evaluation and management, relying on specialty centers may represent the most state-of-the-art management available. Second, inherent to registries which collect clinical data across a diverse number of referral centers, there are some missing data for certain fields. These missing data are likely partially a result of the lack of standardized recommendations regarding imaging protocols, ancillary testing and treatment for patients with FMD. In our multivariate analyses, we cannot exclude the possibility of unmeasured confounders affecting our results. One such confounder may be concomitant atherosclerosis and FMD. Nonetheless, the US Registry for FMD is by far the largest cohort of FMD patients ever assembled, making the available information unique and representing a substantial strength of this study. Finally, as this was a cross-sectional study, it could not offer information about causality. Future analyses of follow-up data regarding this cohort may offer more information about the effect of various medications and interventions on blood pressure management as well as patient outcomes.
Conclusion
Most patients with FMD receive anti-platelet and anti-HTN medications. The use of anti-HTN agents differs by vascular bed involvement, with almost all patients with renal artery FMD requiring at least one anti-HTN agent. In fact, these patients require three or more medications twice as often as patients with cerebrovascular FMD. Anti-platelet agents, on the other hand, were administered broadly in most patients despite the lack of supportive data. In some cases administration patterns deviated from general, non-FMD, consensus guideline recommendations. Further studies of FMD are necessary to correlate medication use with clinically meaningful patient outcomes.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The United States Registry for FMD is funded by the FMD Society of America.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.