
Abstract

Peripheral artery disease (PAD) is a vascular condition involving atherosclerosis and artery narrowing affecting ~236 million people globally. 1 PAD increases the risk of severe cardiovascular events, significantly affecting patients’ health, quality of life, and daily functioning. 2 Noninvasive treatment, including pharmacotherapy and lifestyle changes (e.g., exercise and smoking cessation) or invasive treatment, surgical or endovascular revascularization, 3 aim to reduce the risk of heart attack and stroke and improve quality of life.
Prior work demonstrated that a third of patients with PAD selected from a medical center in The Netherlands had anxiety. 4 Psychosocial factors, like anxiety, are independent risk factors for incident coronary heart disease and cardiac mortality. 5 However, it is unknown how anxiety moderates the association between treatment strategy and PAD-specific health status outcomes. To address this, we examined the association between anxiety, primary treatment strategy, and 1-year PAD-specific health status.
We investigated patients from PORTRAIT, 6 a multicenter study designed to examine associations between patient and care characteristics and health status outcomes among those presenting with new-onset or worsened claudication. The study protocol was approved by the institutional review board at each participating site, and informed consent was obtained from all patients. The Generalized Anxiety Disorder (GAD)-2 scale was administered at baseline, 6, and 12 months. Scores range from 0 to 6, with a score ⩾ 3 indicating anxiety. Patients who underwent either early-invasive treatment (revascularization within 3 months) or noninvasive treatment were identified through medical record review or interviews. The Peripheral Artery Questionnaire (PAQ) was used to assess PAD-specific health status, with scores ranging from 0 to 100 (full health).
Propensity score analysis based on optimal variable ratio matching was used to handle confounding between treatment strategies. Linear mixed-effect models were used to assess the association between anxiety, primary treatment strategy, and PAD-specific health status outcome at 3, 6, and 12 months. Analysis was performed using Stata 17 software (StataCorp LLC, College Station, TX, USA).
In the propensity matched cohort of 1078 participants, the patient characteristics between those undergoing invasive (n = 308) versus noninvasive (n = 770) treatment were well balanced, with no significant differences in treatment distribution between anxiety groups (Supplemental Table 1). Positive anxiety screens were more likely accompanied by a positive Patient Health Questionnaire (PHQ)-8 depression screen (62%) and high levels of perceived stress (64.5%). The proportion of positive screens for anxiety decreased 1 year postprocedure (15.7% baseline vs 9.3% at 1 year, p < 0.001).
Based on linear mixed-effect models, patients with anxiety showed significantly lower PAQ Summary scores at 3, 6, and 12 months versus those without anxiety. Among patients with anxiety, those who received invasive treatment had higher PAQ Summary scores compared to those managed noninvasively (mean difference = 11.4, 95% CI: 5.8, 17.1). The interaction between anxiety and invasive treatment across the study period was significant (p = 0.033), indicating greater benefit from early-invasive treatment for patients with anxiety (Figure 1).
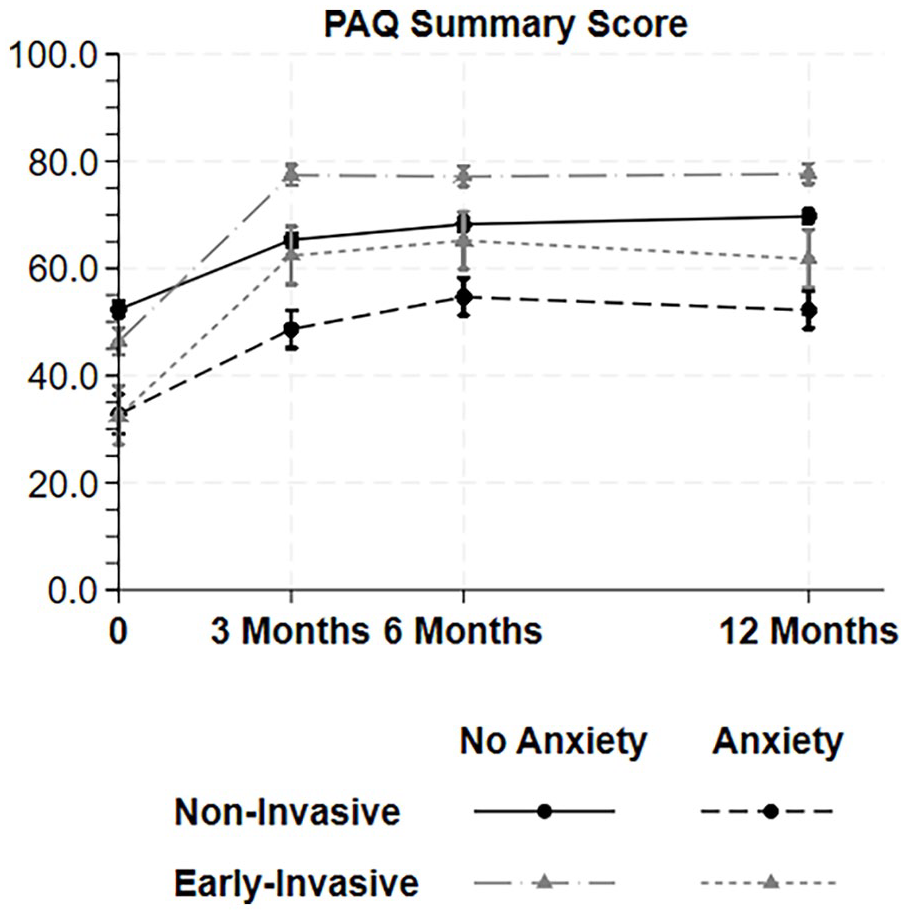
Estimation of the health status, based on Peripheral Artery Questionnaire Summary scores at 3, 6, and 12 months using linear mixed effect models including interaction of anxiety (score ⩾ 3 based on the two-item Generalized Anxiety Disorder scale) and receipt of early revascularization versus noninvasive therapy within 3 months in a propensity score matched cohort of patients with peripheral artery disease.
Using a prospective registry, our study shows that anxiety, in patients with new or worsening claudication, is accompanied by a high depression and stress burden especially upon presentation with symptoms, but the number of individuals affected by it decreased over time. High anxiety is associated with a worse 1-year health status, but with greater short-lived health status improvement when undergoing early-invasive treatment. This is the first study, to our knowledge, to elucidate this interaction. Further studies are needed to evaluate the potential factors contributing to worse health outcomes in patients with PAD and anxiety.
This study contributes to understanding how psychological factors, like anxiety, especially around the time of diagnosis, may interact with the PAD treatment course and treatment modalities offered. Recognizing and screening for psychosocial factors in patients with PAD is necessary for optimal management, allowing for identification of patients who could stand to benefit from evidence-based treatment strategies, given competing psychosocial demands on their functioning.
This study has limitations. First, its nonrandomized design precludes establishing causality. Second, there may be potential unaccounted confounders like active treatment for mental health that patients are receiving, the role of other chronic disease, and patients’ larger exposures to stressors due to their socioeconomic status. However, the propensity matched cohort showed a balanced distribution between treatment groups. Third, subcategories of invasive treatment and repeat invasive procedures were not considered in our analysis. Finally, findings may not generalize to sites outside the PORTRAIT study.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241306406 – Supplemental material for Interaction of anxiety symptoms with peripheral artery disease treatment strategies and health status outcomes
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241306406 for Interaction of anxiety symptoms with peripheral artery disease treatment strategies and health status outcomes by Toluwani Odu, Gaëlle Romain, Lindsey Scierka, Jacob Cleman, Santiago Callegari, Francky Jacque, Carlos Mena-Hurtado and Kim G Smolderen in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Mena-Hurtado reports unrestricted research grants from Philips and Shockwave, and he is a consultant for Abbott Vascular, Cook, Medtronic, and Terumo. Dr. Smolderen reports unrestricted research grants from Philips, Merck, Shockwave, and Johnson & Johnson, and she is a consultant for Terumo, Cook, and Twill Inc. The other authors have no conflicts of interest.
Funding
Research reported in this article was partially funded through two Patient-Centered Outcomes Research Institute (PCORI) Awards (IP2 PI000753-01; CE-1304–6677), The Netherlands Organization for Scientific Research (VENI Grant No. 916.11.179), and an unrestricted grant from W. L. Gore & Associates, Inc (Flagstaff, AZ).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.