
Abstract
Peripheral artery disease (PAD), a prevalent manifestation of atherosclerosis, is associated with increased cardiovascular morbidity and mortality as well as decreased functional ability. Exercise training for PAD is acknowledged to be a highly effective treatment, which improves walking ability and cardiovascular risk. The historical development of this treatment has not been the focus of a report. Therefore, we present a historical review of research on exercise training for PAD. Overall, this body of knowledge has provided strong evidence of the efficacy of supervised exercise training (SET) to improve walking ability for patients with claudication due to PAD. SET, using intermittent bouts of walking exercise to moderate claudication pain on a treadmill, is considered the most efficacious mode of exercise to improve walking ability in patients with claudication. This compelling evidence published over the past 60 years was evaluated by the Centers for Medicare & Medicaid Services in 2017, which culminated in a national coverage determination for SET to improve symptomatic PAD. Future directions include determining optimal delivery strategies for SET and further elucidation of the mechanisms of improvement in walking ability resulting from SET. In addition, alternative forms of exercise should be evaluated and effective home- and community-based exercise interventions should be assessed. There is an enormous need to increase the inclusion of women and racial and ethnic minority groups in studies. It is to be hoped that researchers will continue with new innovative research and persistence in the treatment of claudication due to PAD.
Introduction
Peripheral artery disease (PAD) is a progressive atherosclerotic disease that affects over 200 million people across the world, greatly increasing cardiovascular morbidity and mortality as well as decreasing health-related quality of life.1,2 The prevalence of PAD is estimated to be approximately 13% of all adults over age 50, 3 and increases significantly in older adults over 70 years of age. 1 By age 80, the prevalence of PAD reaches as high as 30%. 1 About a third of PAD patients have claudication, which may be defined as ischemic muscle pain, aching, fatiguing, and cramping in the calves, thighs, or buttocks that is precipitated by skeletal muscle exertion and relieved by rest. 2 Claudication results from an inability to meet the oxygen demand of the working skeletal muscle due to the progressive atherosclerotic plaque buildup in the arteries of the lower limb, thereby limiting walking ability and impairing quality of life in about a third of people with PAD.4,5 The majority of people with PAD are asymptomatic or have mild symptoms. However, these patients still have significant impairment in their health-related quality of life.6,7 A small percent of people with PAD have severe symptoms, which can lead to severe functional impairment or even amputation.8–11 Exercise training has proven to be a powerful tool to treat claudication and thereby improve health-related quality of life. 12 In fact, exercise training has been seen to improve functional status and health-related quality of life, even in those PAD patients who have no symptoms or very mild symptoms of PAD.13–16 Importantly, exercise training has been shown to reduce cardiovascular risk in all people with cardiovascular disease. Dr William R Hiatt, of the University of Colorado, was a pioneer in bringing this treatment to the fore, developing it, and refining it for use in those with PAD.17–22 In honor of this lifetime work on his part, the purpose of this paper is to provide a brief historical view of exercise training for claudication. It is not meant to be an exhaustive systematic or integrative review; rather, we aim to weave a seam through the history of research on exercise training for claudication due to PAD.
The beginning of supervised exercise therapy (SET)
Claudication was initially described in horses by the French veterinarian Bouley in 183123 and Brodie described classical claudication in humans in 1846. 24 In 1858, Jean-Martin Charcot described thrombotic iliac artery aneurism and introduced the term intermittent claudication, 25 and in 1898, Erb described claudication in a series of 13 case reports, which indicated that claudication was more prevalent and occurred earlier in life than previously believed. 26 Moreover, this was one of the initial reports of smoking being a primary risk factor for developing claudication. Following the Framingham studies, additional risk factors were identified, confirming the two most prevalent and prominent risk factors for PAD – smoking and diabetes. 27 As interest and recognition of the prevalence of claudication grew in the mid-20th century, additional tools were added for the assessment of functional capacity in patients with claudication. Specifically, measures to assess walking distance in patients with claudication were developed and utilized. In 1949, Boyd et al. introduced the cladicometer to measure walking distance in patients with claudication due to PAD. 28 The cladicometer was an early design of a walking treadmill test, and a precursor to later methods used to measure walking distance. These methods include the constant-load treadmill test used in the classic Rutherford classification, 29 the graded treadmill test that Hiatt et al. subsequently developed and validated in 1988, 30 and the Gardner–Skinner graded treadmill test, developed in 1991, 31 both of which are commonly used today to investigate walking distance on a treadmill in patients with claudication. Recently, there has been a move to include the 6-minute walk test as an outcome measure of walking distance in patients with claudication since this test provides information regarding functional capacity and response to therapy in PAD, as well as across a range of other limiting cardiovascular conditions. 32
1960–1989: Exercise for claudication in the early years
Treatment for PAD and claudication did not always include rehabilitative exercise training as a cornerstone therapy as recommended by current guidelines, rather the early recommendations included bedrest and avoidance of physical activity. However, a change was initiated in the mid-1960s when Larsen and Lassen conducted the first study to describe the positive effect of daily exercise on walking ability in patients with claudication (Table 1). 33 This study was followed by a number of other intervention studies and mechanistic studies in the late 1960s/1970s, primarily from Scandinavian and German research teams.34,35 In addition, notably the Skinner–Strandness mechanistic ankle pressure study in four men that was published in 1967 suggested that increases in walking distance with repeated testing were due to increased collateralization, as reflected by increased resting and recovery ankle systolic blood pressures.36,37 In 1974, Dahllöf et al. 38 investigated SET compared to placebo tablets in 18 participants with claudication over 6 months (Table 1). This study found that improvements in walking ability were correlated to metabolic activity of the skeletal muscle and not blood flow. In 1976, Dahllöf et al. 39 conducted another randomized placebo-controlled trial in 34 patients with claudication before and after a 4–6-month long exercise training program. They found an increase in walking ability that was greater in the intervention group, compared to the placebo group, but this increase was unrelated to improvements in maximal calf blood flow or blood flow resistance. The authors speculated that collateralization and other physiological mechanisms were responsible for the observed improvement in walking distance. As interest in exercise training for claudication increased, additional studies were conducted during the 1970s and 1980s that continued to indicate an improvement in walking ability following exercise training. Ruell et al. 40 in 1984 showed that 8 weeks of exercise training increased walking distance in both low and high-functioning patients with claudication, and in patients with comorbidities including lung disease and angina. This study was uncontrolled, but suggested that patients with comorbidities, and high or low function, could improve walking distance following exercise training. Additionally, they reported a decrease in exercise blood lactate values suggesting an improvement in muscle aerobic metabolism. Mannarino et al. 1989. 41 compared exercise training versus placebo in 16 participants over 6 months, and included several measures of calf blood flow: Doppler velocity, strain-gauge plethysmography, and transcutaneous oxygen pressure. This study concluded that exercise training improved walking distance with no change in observed blood flow indices. Similar to the study by Dahllöf in 1976, 39 they concluded that mechanisms other than blood flow must contribute to improved walking ability. At about the same time, Carter et al. 198942 investigated 56 patients with claudication in a single-arm study and showed significant increases in walking ability at 3 and 6 months independent of smaller improvements in ankle pressure changes. Additionally, larger-scale studies started comparing surgical reconstruction to SET. In 1989, Lundgren et al. 43 randomized 75 participants to surgery, surgery + SET, or SET alone. At the 13-month follow-up, all groups improved walking distance, with the surgical group improving maximal walking distance the most, but with pain-free walking improving the most in the surgery + SET group (Table 1). In a separate report of 23 participants undergoing surgery, surgery + SET, or SET alone, Lundgren et al. 44 showed that calf blood flow increased in the surgical groups, but that metabolic enzymatic improvements improved with SET, which was positively correlated with pain-free walking distance, suggesting that SET improves skeletal muscle metabolism.
Key papers on exercise therapy for peripheral artery disease 1960–2020.
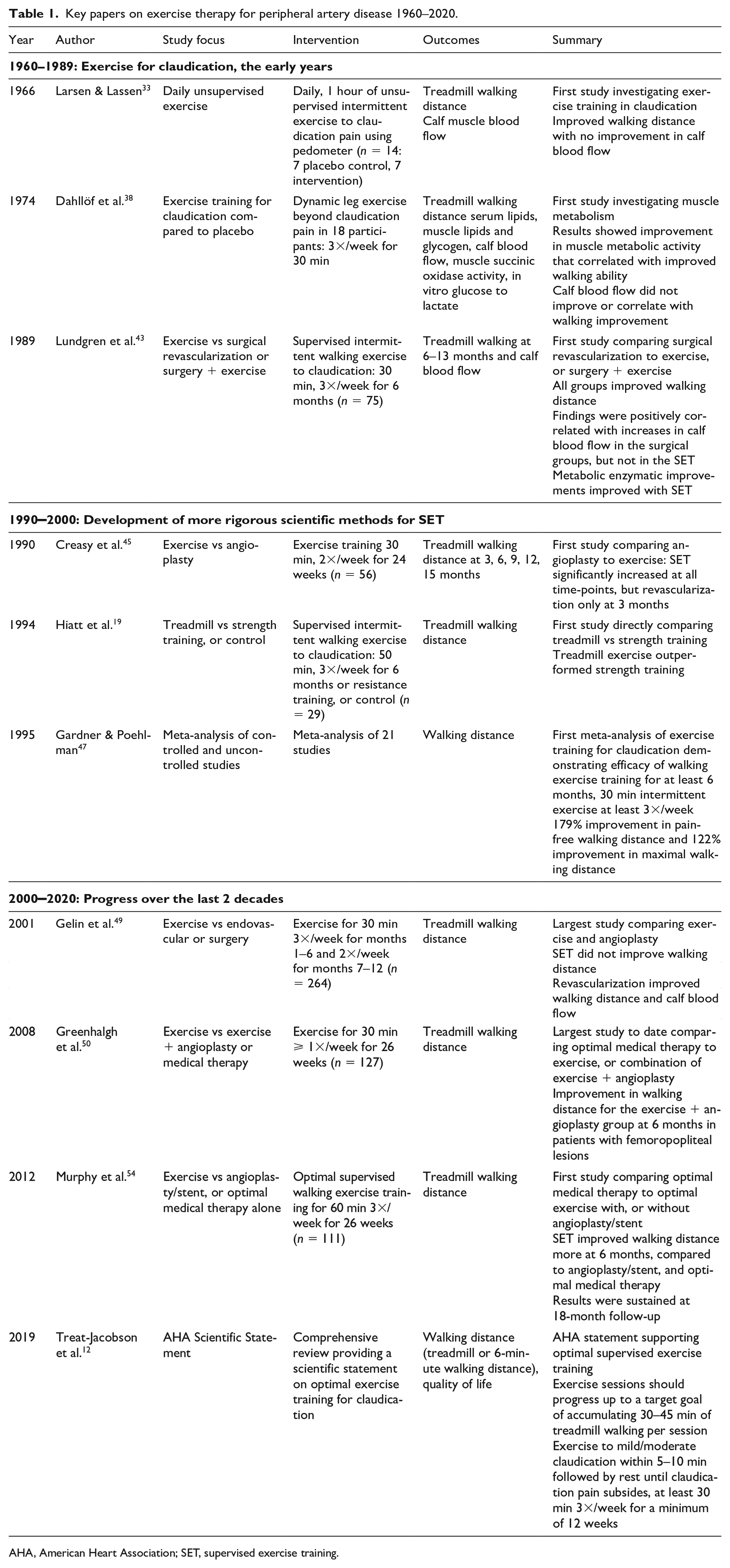
AHA, American Heart Association; SET, supervised exercise training.
1990–2000: Development of more rigorous scientific methods for SET
In 1990, several studies were published further demonstrating the benefit of exercise training on walking distance in patients with claudication. Hiatt et al. 18 randomized 19 men with claudication to walking exercise training (1 h/day, 3 days/week, for 12 weeks) or control. They reported a 123% increase in walking distance and 165% increase in pain-free walking time in the intervention group, accompanied by an increase in calf blood flow and a decrease in short-chain acylcarnitine concentration, suggesting metabolic improvement in the trained skeletal muscle. During that same period, Creasy et al. 199045 reported that walking distance increased at 6, 9, and 12 months following SET without improvement in ankle–brachial pressure, whereas patients randomized to percutaneous transluminal angioplasty (PTA) improved ankle–brachial index (ABI), but not walking distance. In 1994, Hiatt et al.19,22 reported that participants receiving SET showed 38% greater improvement in walking distance compared to a group receiving strength training, with no significant improvement in the nonexercising control group. Following a modified cross-over design, all participants continued walking exercise training for an additional 12 weeks, which indicated similar improvements across groups, suggesting the walking exercise training outperforms resistance training as a training modality. This improvement was related to muscle metabolism as indicated by a reduction in short-chain acylcarnitine. Regensteiner et al. 46 further reported in 1996, from the same study sample, that self-reported health-related quality of life (measured by a walking impairment questionnaire) was significantly improved in both the strength training and the walking exercise training group, but that the walking exercise group improved more with additional benefits at 24 weeks. In 1995, Gardner and Poehlman 47 published a seminal meta-analysis to identify the most effective components of exercise training to improve walking ability in patients with claudication. This meta-analysis provided an essential evidence-base in demonstrating the efficacy of walking exercise training as a critical therapy for patients with claudication. Specifically, this meta-analysis established that a walking exercise program was the preferred mode of exercise, and that the program should last at least 30 minutes per session, at least three sessions per week, for a duration greater than 6 months. Additionally, the walking program should consist of intermittent walking to near maximal claudication pain. This meta-analysis was used for almost a decade as a primary evidence-base of the efficacy of walking exercise to improve functional capacity in patients with claudication. Of note, given the timing, this meta-analysis did not include the studies by Hiatt et al.19,22 or a study that was published in 1996 by Perkins et al. 48 showing that SET increased walking ability more as compared to the angioplasty group in 56 participants with stable claudication over 15 months. Since the Gardner and Poehlman meta-analysis was published, additional early investigations have shown that SET was superior to home-based exercise, possibly due to the consistent therapeutic environment and controlled exercise progression. Additional studies continued to show that SET overall resulted in greater functional improvement compared to angioplasty. However, there were some conflicting reports in the literature depending on procedures and patient inclusion criteria. During the late 1990s and into the early 2000s, numerous meta-analyses, systematic reviews, and Cochrane reviews were published as a testament to the exponential increase in research interest of SET for claudication giving rise to the current era.
2000–2020: Progress over the last 2 decades
SET versus angioplasty
During the last 2 decades there has been a substantial increase in studies comparing interventional therapy and vascular surgery to SET, or medical therapy. Gelin et al.
49
published a randomized controlled trial (RCT) in 2001 comparing open surgical or endovascular procedures to SET in 264 patients (Table 1). They reported that walking ability increased in the surgical groups compared to SET, and blood flow and pressure improved in the surgical group only. In 2008, Greenhalgh et al.
50
reported on two randomized trials comparing SET to SET + angioplasty, with both groups receiving optimal medical therapy defined as blood pressure control of < 140/85 mmHg, cholesterol < 5 mmol/, blood glucose < 7.3 mmol/L, and antiplatelet treatment with 75 mg aspirin or clopidogrel, compared to optimal medical therapy alone (for conversion to mg/dL multiply by 18). The SET only consisted of a once weekly exercise session for 6 months. Walking ability was significantly higher for the angioplasty + SET group, but only in patients with femoropopliteal revascularization and not in patients with aortoilliac revascularization (Table 1). Spronk et al.
51
in 2009 reported a similar benefit in walking ability at 6 and 12 months from SET or endovascular revascularization in patients with claudication. In 2010, Mazari et al.
52
conducted a RCT comparing angioplasty to SET, or angioplasty + SET in 178 participants. The 1- and 3-month follow-up showed an improvement in walking ability across groups, with a substantially larger improvement in the group receiving the combined therapy. At the 12-month follow-up, Mazari et al.
53
reported that these early effects remained, but the combination therapy appeared to provide a more sustainable clinical improvement. At the same time, Hiatt et al.
17
reported the results from a randomized controlled trial investigating whether propionyl-
In 2012, the landmark CLEVER study was published by Murphy et al. 54 CLEVER investigators randomized 111 patients with aortoiliac disease due to PAD to either SET, SET + stent, or optimal medical care-treated control groups across 29 sites in the US and Canada. All groups received optimal medical care. The SET was designed by a panel of exercise experts in claudication. 55 At 6 months, the SET group showed the largest improvement in walking distance, followed by the stent group, compared to the optimal medical therapy group. Quality of life improved across groups, with larger improvements observed in the stent group (Table 1). An 18-month follow-up was published in 2015 in 79 participants that completed follow-up assessment. 56 The improvement in walking distance was sustained in both SET and the stent group, compared to the optimal medical therapy only group. These results suggest that both SET and angioplasty with stent improved walking ability in patients with claudication and aortoiliac disease.
Meta-analyses and Cochrane reviews supporting the evidence base of SET for claudication
The accumulated wealth of studies in exercise training for PAD reported above has led to a larger number of meta-analyses, systematic reviews, and Cochrane reviews. In 1999, Girolami et al. 57 published a meta-analysis comparing exercise to smoking cessation, pentoxifylline, or nafronyl on improvement in walking ability. This study reported that exercise training improved maximal walking distance 179 meters in five studies, compared to 47 meters in one smoking cessation study, 44 meters in six pentoxifylline studies, and 71 meters in four studies with nafronyl.
Reviews of supervised exercise training for claudication
In 2000, Leng et al. 58 published a Cochrane review that included 10 RCTs involving 250 participants, all with stable classical claudication pain. These early trials were small and ranged between 20 and 49 patients. However, the quality of the trials was considered good. This Cochrane review found that SET improved maximal walking time by 6.51 minutes or 150%, although a significant variability was noted (range, 74–230%). Additionally, it was noted that SET improved walking ability compared to angioplasty and medical therapy, and was equivalent to surgery. This was followed by Bendermacher et al. in 2006, 59 whose review compared supervised versus non-SET on walking ability in patients with claudication. This study included eight RCTs involving 319 participants and showed a significant and clinically relevant improvement in SET compared to nonsupervised exercise training. These reviews have been updated periodically over the past two decades and the number of included studies and enrolled participants have increased exponentially, and in some instances the results were changed. For example, in 2008, Watson et al. 60 included 22 RCTs, totaling 1200 participants with claudication with a follow-up period ranging between 2 weeks and 2 years. This study reported an improvement in peak walking distance by 150% within 12 weeks, with walking sessions performed for a minimum of 30–45 minutes at least three times per week, and this improvement lasted for up to 2 years. In 2014, Lane et al. 61 updated this review to 30 RCTs involving a total of 1816 participants. Unfortunately, the quality of the trials included were of moderate quality as a result of inadequate information published. The authors concluded that exercise improves maximal and pain-free walking distance, compared to placebo and usual care, by 50–200%. The most recent update of this Cochrane review was performed in in 2017 by Lane et al. 62 This time, only two additional studies were included for a total of 1835 participants. This review concluded that there is high-quality evidence for SET leading to improvement in walking ability compared to usual care or no exercise, with moderate evidence for improvement in quality of life. The reason for only including two additional trials in this review was explained by the authors to be due to the design of most present studies, which included only different walking exercise prescriptions, or exercise versus other modalities and not exclusively SET versus control.
Determining the benefits of home-based walking exercise
Additionally, studies comparing alternative exercise prescriptions and modalities have increased substantially during 2000 to 2020. Although SET has been shown to be highly efficacious to improve walking ability in patients with claudication, a large group (69%) of patients find the barriers to SET to be too high. 63 Traveling to an exercise facility such as a hospital rehabilitation unit, program costs and failure of insurance to pay for this treatment have all been among the barriers that inhibit participation in SET programs. Home-based exercise has the potential to provide these patients with an opportunity to gain the benefit of exercise training while not raising the same barriers. The earlier studies conducted by Regensteiner et al. 64 in 1997, by Savage et al. 65 in 2001, and Menard et al. in 200466 showed no benefit from unsupervised exercise and general walking advice compared to SET. In 2011, Collins et al. 67 randomized 145 participants to either control or behavioral intervention with counseling and a once-weekly supervised session in addition to three sessions at home for a total of four sessions/week). Participants also received bi-weekly phone calls tailored to facilitate behavioral change. At 6 months, there was no improvement in either group observed. However, since these early trials, several new technologies, including behavioral techniques, have been included in studies to improve walking adherence at home. In contrast to the early trials, which chiefly included unstructured advice to go home and walk, in 2013, McDermott et al. 15 reported the results of the GOALS trial (Group Oriented Arterial Leg Study) in 192 participants with PAD. This 6-month study included a group that received weekly cognitive behavioral therapy (CBT) promoting home-based walking exercise compared to attention control subjects. At 6 months, the CBT group increased their 6-minute walking distance by 53 meters, compared with the control group. These results were sustained at 12 months. 68 In 2014, Gardner et al. 69 conducted a RCT in 180 participants comparing SET to home-based exercise, or light resistance training. The home-based walking exercise was monitored with a step monitor and participants met with a study investigator four times over 12 weeks. At the 12-week follow-up, the 6-minute walking distance increased more in the home-based walking exercise group compared to the other two groups. However, in contrast, the HONOR trial, published in 2018, showed no improvement in walking ability at the 9-month follow-up in a group (n = 99) that received tailored coaching phone calls and an activity monitor, compared to usual care (n = 101). 70 The investigations into optimal home-based exercise for patients with claudication is continuing with several novel approaches, including the use of music to motivate, distract from pain, and guide the home-based exercise program. The music program allows for varying the tempo of the music to allow for intermittent exercise at proper intensity to mild/moderate claudication pain, followed by short rest periods, and thereby mimicking SET. 71 The American Heart Association currently gives home-based exercise training an evidence level of IIa. 12 Further research will be beneficial to the field of exercise training for PAD.
Updated reviews of supervised versus nonsupervised exercise training for claudication
The updated Cochrane reviews investigating supervised versus non-SET were published in 201372 and 2018. 73 The 2013 update included 14 RCTs and a total of 1002 participants. This study reached the same conclusion that SET improved walking distance compared to nonsupervised exercise with a moderate effect size of 0.69 up to 12 months. 72 The 2018 update included 21 RCTs with a total of 1400 participants, comparing SET to home-based exercise training, or nonstructured walking advice, and reached a similar conclusion that there is moderate/high-quality evidence of the benefit of SET compared to home-based exercise and walking advice alone. 73
Modifications of SET
Alternative forms of exercise for people with PAD
In addition to home-based walking exercise, other alternative forms of exercise to SET have been of increasing interest over the past 20 years (Table 2). In 2000, Walker et al. 74 reported an increase of 57% in maximal walking distance achieved during a shuttle walk test following cycling compared to control. A similar finding was reported by Zwierska in 2005. 75 However, in 2006, Sanderson et al. 76 reported a larger improvement in the SET group compared to a leg cycling group (n = 41) at 6 weeks. An interesting twist in terms of exercise mode was introduced by Walker et al. 74 and Zwierska et al., 75 who introduced not only leg cycling but also arm-ergometry, which showed an average of 30% improvement in walking distance following arm-ergometry, suggesting a possible systemic transfer effect. With the inclusion of Tew et al., 77 there have been 212 participants included in these studies showing an overall improvement of 50% in pain-free walking distance. Few studies have compared walking SET to arm-ergometry. However, current evidence suggests that arm-ergometry exercise training may improve both pain-free and maximal walking distance similarly to SET, although more study is required.78,79 The use of resistance training in the earlier studies cited above suggested a smaller improvement in walking ability compared to walking SET. However, McDermott et al. (2009) 13 and Ritti-Diaz et al. (2010) 80 reported no difference in walking improvement between walking SET and resistance training, although these studies were likely not powered to detect differences between groups. In 2013, Parmenter et al. 81 reported that high-intensity resistance training improved walking distance more than low-intensity resistance training, although this study did not compare outcomes to those of a walking SET group. A recent meta-analysis by Paramenter et al. suggests that resistance training is beneficial in improving walking distance. 82 The utilization of resistance training programs to improve walking distance is still in its infancy.
Summary of supervised walking exercise training and alternative modes of exercise.
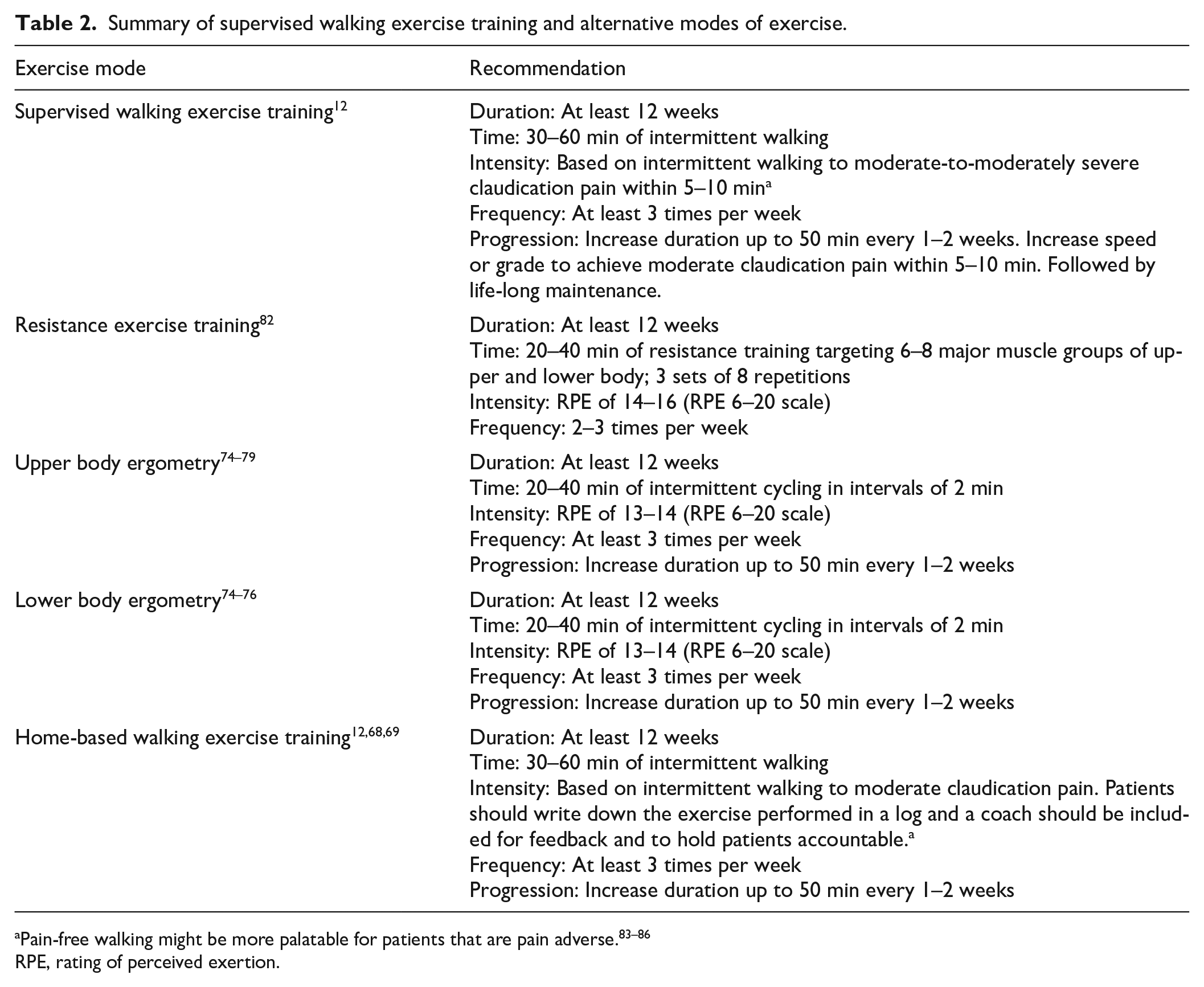
RPE, rating of perceived exertion.
Several trials have investigated the efficacy of pain-free walking SET to improve walking ability in patients with claudication. Three studies were published by Mika et al. between 2005 and 2011.83–85 These studies showed a mean increase in maximal walking distance of 52% and a mean increase of 110% in pain-free walking distance, compared to control. In 2013, Mika et al. 86 compared pain-free SET to moderate pain SET in 52 participants and found comparable improvements in walking distances in both groups. These intriguing findings suggest that it may be possible to achieve the same walking improvement using both moderate pain SET and pain-free SET, although much research is required to confirm these results.
Interest in SET for patients with asymptomatic PAD has increased over the last decade. It has been reported that up to 63% of patients with PAD are asymptomatic. However, even asymptomatic patients still have a significant functional impairment and rapid functional decline. 87 McDermott et al. reported improved walking distance in asymptomatic PAD following both SET and home-based walking exercise in 2004, 16 2009, 13 2013, 15 and 2017. 14 However, is should be noted that these studies were not powered to compare outcomes between those with asymptomatic PAD and those with symptomatic PAD.
Reviews of modes of exercise for claudication
In 2014, Lauret et al. 88 conducted a Cochrane review on the modes of exercise training for claudication. This study included five RCTs totaling 135 participants, comparing walking SET to other modes of exercise training, cycling, strength training, and upper arm-ergometry. They found no clear difference between walking SET and alternative modes of exercise, which suggested that alternate modes of exercise may also be useful to improve walking ability in patients with claudication. An update to this review was provided in 2020 by Jansen et al. 89 This updated review included an additional five RCTs for a total of 10 RCTs and 527 participants. The results remained unchanged and there were no clear differences between modes of exercise. However, the quality of evidence was judged to be low amid sample size concerns and risk of bias. The authors issued a call for further research in the area. The number of studies that have been published during the past 20 years have overwhelmingly shown a benefit of exercise training in improving walking ability in patients with claudication as well as in atypical and asymptomatic PAD. Meta-analyses continue to support the use of 12–24 weeks of SET, with 24 weeks showing larger mean improvements 90 and mean improvements in maximal walking distance of 180 meters. 91
Mechanism of improvement of walking ability
A complete discussion of the physiological mechanisms of improvement of walking ability following SET63,92–95 is beyond the scope of this article. In brief, exercise training stimulates adaptive responses including the potential for formation of collateral blood vessels 96 and thereby increasing blood flow via angiogenesis. 92 However, increased blood flow does not appear to be a primary mechanism of improvement, as shown by a number of studies since the mid-1960s as discussed above. Exercise further improves vascular endothelial function, 97 but few studies have investigated this in response to exercise in patients with claudication. Exercise is known to improve glucose utilization, local and systemic inflammation, 98 lipid-profile to a small extent, and the neurohormonal axis.63,93–95 A few studies have shown improved hemorheology, including improved viscosity and red cell pliability.83,99 Most research has shown that SET leads to improvement in skeletal muscle metabolism and oxygen utilization, 22 as discussed above. Whole-body physiological studies suggest an improvement in walking economy following SET, shown by improvements in respiratory gas exchange measures, blood lactate levels, and heart rate.19,100,101 The mechanism of improvement of walking ability following SET is still an area of active investigation.
The journey for Centers for Medicare & Medicaid Services reimbursement
The collected body of knowledge since the mid-1960s has provided strong evidence of the efficacy of SET in claudication due to PAD and even in those who are asymptomatic. SET, using intermittent bouts of walking exercise to moderate claudication pain, has been most extensively studied compared to other forms of exercise for PAD and is currently considered the most efficacious mode of exercise to improve walking ability in patients with claudication. As a result, SET has received a level A evidence base. 12 The large body of work about SET published over the past 60 years was evaluated by the Centers for Medicare & Medicaid Services (CMS) in 2017, which resulted in a determination that national coverage is appropriate since SET improves walking ability in those with symptomatic PAD. CMS conducted an in-depth investigation of the available evidence base, including most of the studies cited in this review. A decision memorandum was issued on March 2, 2017, stating that the evidence base for SET for patients with claudication was sufficient for CMS to cover 30–60 minutes of SET, up to 36 sessions, over a 12-week period for CMS beneficiaries. As of May 25, 2017, CMS covers SET for the treatment of claudication provided in an outpatient hospital setting or physician’s office, delivered by qualified personnel trained in SET for PAD, and under direct supervision of a physician, physician assistant, or nurse practitioner/clinical nurse specialist. Patients must be referred by a physician, are required to have a face-to-face visit with the supervising physician, and receive cardiovascular and PAD risk factor reduction.
Current SET guidelines for claudication
The cited studies have led to the most up-to-date scientific statement by the American Heart Association on optimal exercise programs for patients with PAD. 12 In brief, treadmill walking exercise for patients with claudication due to PAD consists of intermittent walking bouts to moderate/moderately severe discomfort followed by short periods of rest until symptoms resolve. Based on current evidence, the exercise/rest bouts should be repeated over 30–60 minutes at least three times per week for a minimum of 12 weeks. These recommendations are based on meta-analyses that reported that > 30–60 minutes were more beneficial and that > 30 minutes of SET results in similar improvements as 60 minutes and may peak at 45 minutes. The use of walking to moderate pain rather than maximal pain is based on a majority of studies that have included this form of exercise. However, several newer studies suggest that improvement can be obtained even without walking to claudication pain (defined as no pain or mild pain), as reported above (Table 2).
Future directions
It is predicted that the trend of innovation in the use of exercise training for patients with PAD will continue with additional research into several areas identified below:
Elucidation of the physiological and biological mechanisms of improvement
Identification of effective home-based or community-based exercise intervention type/delivery
Implementation trials in the community
Identify behavioral methods increasing adherence
Trials comparing surgical, percutaneous revascularization, and exercise across lesion sites
Greater use of these therapies in women and minorities; determination of potential sex/racial differences in the effects of training
Identification of optimal individual therapies; elucidation of variability in response to exercise training to enable personalized medicine-based prescriptions
Investigations of the short- and long-term effects of exercise training on health-related quality of life and functional outcomes of activities of daily living
One of the most compelling needs is greater inclusion of minorities and women in order to address health inequity. Most of the earlier publications that we reviewed did not include racial or ethnic minorities or women until more recently. It is encouraging that more recent studies have begun to examine racial, ethnic, and sex differences in functional decline in PAD patients, even with a smaller percentage of Black participants (26%). 102 Collins et al. 103 recently reported that a cognitive and patient-centered assessment improved walking distance compared to motivational interviewing in Black Americans with PAD. Additionally, the CLEVER trial reported a greater improvement in quality of life measures in Black Americans in subanalyses. 104 The reader is referred to Hackler et al., 105 who recently published a review of racial and ethnic disparities in the PAD population. Black and Latinx participants continue to be under-represented in exercise trials. This is particularly concerning considering the high prevalence of PAD in these patient populations, especially in women. 106 Additionally, although research has increased recently with inclusion of women, there is still a lack of understanding of potential sex differences in response to exercise training for claudication. Goomans et al. 107 further suggested a possible sex difference in response to exercise training, which needs to be elucidated. There is therefore an enormous need to maximize efforts to increase the inclusion of women, racial minority groups, and other traditionally excluded minority groups in studies. The impact of structural and institutional racism and social determinants of health should be investigated and corrected to eliminate health disparities in the treatment of PAD, including exercise therapy. In summary, the future of PAD treatment is bright and it is predicted that the ingenuity of the trailblazing researchers over the past 60 years will continue with new innovative and persistent research efforts to advance the field of vascular medicine.
Footnotes
Acknowledgements
We acknowledge the groundbreaking work of William R Hiatt, MD (1950–2020) whose leadership, scholarship, and mentorship resulted in extensive growth of the field of supervised exercise training for peripheral artery disease. This therapeutic approach has brought improved health to many people around the world and changed the face of treatment for PAD.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.