
Abstract
Data on simultaneous hemodynamic changes and pain rating estimation in arterial claudication while walking are lacking. This study was conducted to determine if a difference in transcutaneous oxygen pressure (tcpO2) exists between proximal and distal localization at pain appearance (PAINapp), maximal pain (PAINmax) and pain relief (PAINrel) in proximal or distal claudication and if a relationship exists between tcpO2 changes and pain intensity. We analyzed the pain rating (Visual Analog Scale (VAS)) to lower limb ischemia, measured with the decrease from rest of oxygen pressure (DROP) tcpO2 index during constant-load treadmill tests in patients with calf (n = 41) or buttock (n = 19) claudication. Calves versus buttocks results were analyzed with ANOVA tests. The R2 correlation coefficient between individual VAS versus DROP was calculated. Ischemia intensity versus pain rating changes were correlated. Significant ischemia was required for pain appearance, but pain disappeared despite the persistence of ischemia. We observed no statistical difference for DROP at PAINapp, PAINmax or PAINrel between proximal or distal claudication. A significant correlation between pain rating versus DROP was found: from PAINapp to PAINmax, R2 = 0.750 (calves) and 0.829 (buttocks), and from PAINmax to PAINrel, R2 = 0.608 (calves) and 0.560 (buttocks); p<0.05. Pain appeared after a significant decrease of hemodynamic parameters but disappeared while parameters were not normalized. No difference in pain rating was found in proximal versus distal claudication.
Introduction
Peripheral artery disease (PAD) is a frequent cause of walking-induced lower limb pain (intermittent claudication) resulting in walking limitation.1,2 Pain while walking in PAD defines stage 2 of the Fontaine 3 and stages 1 to 3 of the Rutherford classifications.4,5 Lower limb pain generally affects calves (distal claudication) and/or buttocks (proximal claudication). Distal claudication mainly results from femoro-popliteal lesions whereas proximal claudication is observed in aorto-iliac lesions. There are some clinical differences between proximal and distal claudication. First, in the so-called ‘Leriche syndrome’ (occlusion of the terminal aorta and proximal ischemia), pain is usually described as a lower limb fatigability, whereas calf (Rose-type) claudication is described as a cramp or pain. 6 Second, exercise-induced proximal claudication seems to be under-reported by patients and under-diagnosed by clinicians7,8 compared to distal claudication. It has never been studied whether these differences rely on a difference in the relationship between exercise-induced proximal/distal ischemia or a different perception of proximal/distal pain intensity.
A previous study 9 showed a correlation between pain appearance and walking intensity but not with pain departure. Moreover, a weak concordance exists between resting (before exercise) or post-exercise hemodynamic measurements and walking impairment. 10 A study of intra-muscular oxygen pressure similarly showed a correlation of ischemia and pain at the calf level in claudicants. 11 Nevertheless, as far as we know, there are no data about the relationship between non-invasive hemodynamic parameters during both walking and recovery (exercise-induced ischemia) and pain intensity rating in patients with either proximal-without-distal pain/ischemia or distal-without-proximal pain/ischemia.
Transcutaneous oxygen pressure (tcpO2) can be used to monitor exercise-induced regional blood flow impairment (RBFI) throughout rest, exercise and recovery, although it is a skin (surface) recording. Because of the lack of other techniques that could record RBFI throughout exercise and recovery, tcpO2 is a useful marker. Furthermore, tcpO2 can assess proximal (buttocks) or distal (calves) ischemia simultaneously and on both sides. Thereby, tcpO2 is a unique tool to evaluate the relationship between exercise-induced hemodynamic parameters and pain intensity rating throughout rest, exercise and recovery in PAD patients suffering from either isolated proximal-without-distal or isolated distal-without-proximal claudication. 12
We hypothesized that:
A difference in ischemia intensity could be observed between proximal and distal claudication at pain appearance (PAINapp), maximal pain (PAINmax) and pain relief (PAINrel) in patients suffering from isolated proximal-without-distal or isolated distal-without-proximal claudication.
A significant ischemia is required before pain appears (DROP tcpO2 ≤ −15 mmHg). Similarly, pain disappears while hemodynamic parameters are not normalized.
When pain is present, a relationship exists between changes in hemodynamic parameters and changes in rating of pain intensity from PAINapp to PAINmax and from PAINmax to PAINrel.
Methods
Participants
We performed a single-center retrospective observational study among consecutive patients eligible for this study over a 4-year period, referred for exercise tcpO2 tests in the department of vascular investigations at the University Hospital of Angers, France. All patients were evaluated using a standard treadmill procedure. At admission, patients were asked to complete the Edinburgh Claudication Questionnaire and to report all potential painful locations on the body. 13 The treadmill procedure and questionnaire were conducted as part of standard care. At the time of completion of the tests, as the clinical records were analyzed retrospectively and anonymously, in accordance with the French law, no written consents from the patients were needed. The study design received specific approval from the ethic committee at the University Hospital of Angers. Only patients reporting typical vascular-type claudication were considered for the analysis. ‘Vascular-type’ claudication is a lower limb pain, absent at rest but occurring while walking after a pain-free walking period and increasing when walking is continued, forcing the patient to slow down or stop and finally disappearing within 10 minutes of walking cessation. 6
As a routine, we recorded: stature, weight, sex, diabetes, treatments and resting ankle to brachial systolic pressure index (ABI). Exercise tcpO2 is a routine technique in our laboratory and in our study all the clinical records were analyzed retrospectively and anonymously. Moreover, the study design received specific approval from the ethics committee, and the principles of the Declaration of Helsinki were followed. For this retrospective study, we aimed at selecting two clearly different and characteristic populations. We selected only patients with:
No diabetes, to avoid neuropathic pain;
Isolated proximal-without-distal or isolated distal-without-proximal vascular-type claudication;
Limiting claudication (maximal walking time on treadmill < 10 minutes);
No cardiac or respiratory or osteo-articular disease that might interfere with walking limitation;
No use of any kind of painkillers or analgesic drugs that might interfere with the rating of pain;
Claudication at one single site both by history and on the treadmill (e.g. patients with proximal-and-distal symptoms or bilateral symptoms were not included);
Presence of a significant ischemia (DROP ≤ –15 mmHg ) in the area of reported symptoms;
Presence of at least three different levels of pain intensity between PAINapp and PAINmax and two different levels of pain intensity between PAINmax and PAINrel. These values were arbitrarily defined to confirm the correct participation of the patient and allow for the analysis of the relationship of pain to ischemia;
Absence of error in the use of the Visual Analog Scale (VAS), an error being defined as a value above 0 at rest or end recovery, or a maximal VAS at PAINmax <10);
Absence of a tcpO2 chest curve of C or D type to eliminate unknown exercise-induced hypoxemia as a potential cause of exercise limitation. Indeed, the chest tcpO2 changes are classified into four types (A, B, C or D) as beforehand reported. 14 A minimal decrease in excess of 3 mmHg from resting value is required to classify the chest curve in the C or D category, as already published. 15 As previously reported, types A and B are expected to represent normal systemic oxygenation during exercise, whereas types C and D are expected to result from walking-induced hypoxemia. 14 Patients were then divided into two groups: isolated-proximal (buttock) vascular-type claudication with underlying isolated-proximal ischemia or isolated-distal (calf) vascular-type claudication with underlying isolated-distal ischemia.
Imaging analysis
Anatomic localization of the disease in the buttock claudication group versus the calf claudication one were analyzed from reports for radiological and ultrasound imaging, analyzing separately proximal trunks towards the hypogastric circulation (aorta, common and internal iliac arteries) and distal ones (external iliac and femoro-popliteal lesions). Since no patient reported thigh pain, the external iliac artery was considered responsible for distal ischemia
Transcutaneous oxygen pressure measurements
Because the presence of an image is not proof of the presence of exercise-induced ischemia, we used exercise tcpO2 to argue for or against the presence of ischemia underlying the area of pain. For tcpO2 measurements, we used five tcpO2 devices (TCM3; Radiometer, Copenhagen, Denmark) with probes heated to 44.5°C. Stabilization of the tcpO2 values took approximately 20 minutes before each test to attain maximal vasodilation. The tcpO2 values were automatically transferred to a computer (AcqKnowledge software, v3.7.2; BIOPAC Systems, Inc., Goleta, CA, USA) on a sample rate of 0.5 Hz. Probes were positioned on the chest, on the upper external quarter of each buttock and on both calves approximately 4 cm above the ankles. The tcpO2 was recorded for 2 minutes at rest, during exercise and throughout recovery. From tcpO2 recorded values, we automatically calculated the decrease from rest of oxygen pressure (DROP) at each limb site. The DROP index has previously been described and validated.16,17 The DROP index consists in the subtraction of limb tcpO2 changes from chest tcpO2 changes. At either proximal (buttocks) or distal (calves) sites, a significant ischemia is a minimal DROP value ≤ −15 mmHg. Lower DROP values are observed in more severe arteriographic lesions. 17 The reliability of the DROP index on repeated tests has been previously demonstrated at the calf level. The test-retest reliability is fair to good with absolute minimal tcpO2 values. Because DROP is independent from starting values (and from the transcutaneous gradient), the test-retest reliability of tcpO2 is excellent and much higher than it is when tcpO2 is expressed in absolute value. 17
Visual Analog Scale
A homemade electronic VAS was used. It consisted in a 10-cm-long straight line with a vertical presentation from no pain (lower end) to maximal pain forcing the patient to stop (upper end), along which the patient might displace a cursor from one end to the other (Figure 1). The system automatically converted the position of the cursor to a current with a linear response from 0 (no pain) to 10 volts (maximal pain). The patients were asked to move the cursor as often as possible, and if needed were reminded to do so, throughout the test. They were informed that the treadmill test would be stopped as soon as the pain rating reached its maximum (10 arbitrary units) or at their request if they were unable to handle the VAS system while walking. Throughout the exercise and recovery periods the patient was recalled, on a once per minute basis, to modify the position of the cursor if needed. Data from the VAS were automatically transferred to the computer and recorded simultaneously with tcpO2 values with a 0.5 Hz sampling rate.

Electronic Visual Analog Scale, which consisted of a 10-cm-long straight line with a vertical presentation from no pain (lower end) to maximal pain (upper end), along which the patient could displace a cursor from one end to the other.
Treadmill exercise test
Our standard procedure included: a 2-minute reference period at rest while the patient was standing still on the treadmill; thereafter, the walking period was performed at 10% grade and 3.2 km/h. Patients were blinded to the distance and time throughout the test. When exercise was stopped, the speed and slope rapidly returned to zero. During the recovery phase after walking, the patient was asked to remain stable in the standing position. Recovery usually lasted 10 minutes but could be prolonged if pain or ischemia was still present at minute 10.
Two different examples of VAS pain rating and tcpO2 recording are reported in Figure 2: patient A had a calf claudication and patient B a buttock claudication. Specifically, pain was reported to have completely disappeared in patient B far before hemodynamic values were normalized, whereas it was not the case for patient A, with pain departure closer to the hemodynamic normalization. As shown in online supplementary data, the difference does not seem to depend on the localization of pain but seems to result from individual sensitivity to pain (Supplemental Figure 1). Indeed, we found simultaneous or non-simultaneous departure of pain rating and ischemia in patients of both groups (proximal or distal ischemia).
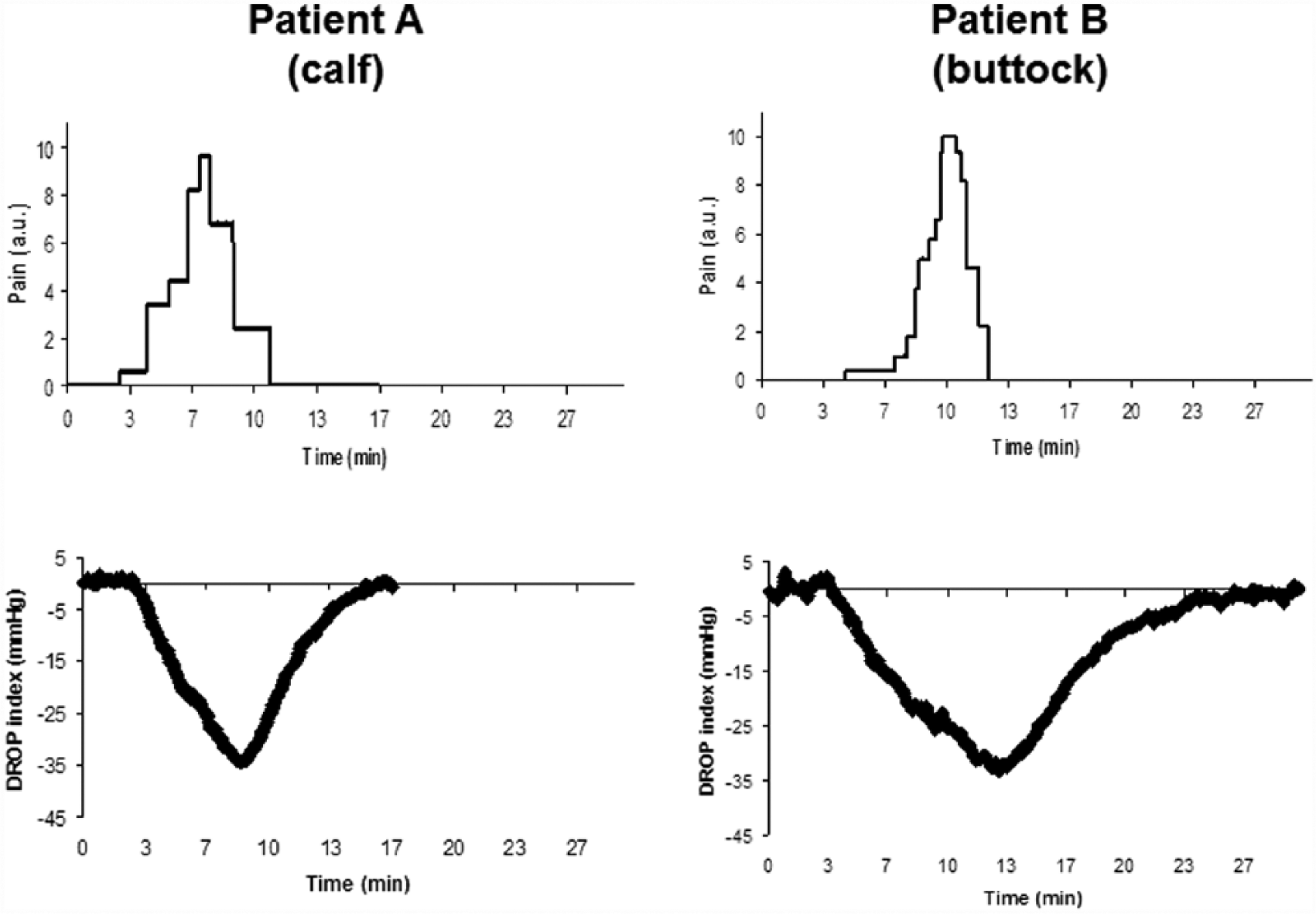
Two different examples of pain rating (Visual Analog Scale) and tcpO2 recording. Patient A has a calf claudication and patient B has a buttock claudication. (a.u., arbitrary unit; DROP, decrease from rest of oxygen pressure)
Analysis of data
We used analysis of variance (ANOVA) to compare calf versus buttock DROP tcpO2 values at PAINapp, PAINmax and PAINrel, and to define whether DROP values were significantly different from their respective resting values. We calculated the average of the pain rating, DROP tcpO2, for 10 different intervals of pain rating: [0–1], [1–2], … [9–10] in the PAINapp to PAINmax individual period; and for 10 different intervals of pain rating: [10–9], [9–8], … [1–0] in the PAINmax to PAINrel individual period. Then, we analyzed the correlation between the individual average values for pain versus DROP from PAINapp to PAINmax and from PAINmax to PAINrel with non-linear (logarithmic) models with Microsoft Excel. The R2 coefficient of correlation for Spearman (for non-linear analysis) was calculated for this model with SPSS software (version 23.0; IBM Corp., Armonk, NY, USA). For all the tests, we used two-tailed p < 0.05 to define statistical significance.
Results
Participants
We finally included 60 patients in our study. Characteristics of the studied patients are reported in Table 1. No major difference was found between the two groups (proximal vs distal claudication) except for the average ankle to brachial index (ABI) values (p = 0.04). It is noteworthy that patients with distal claudication had significant lower ABI than those with proximal claudication.
Characteristics of the studied patients.
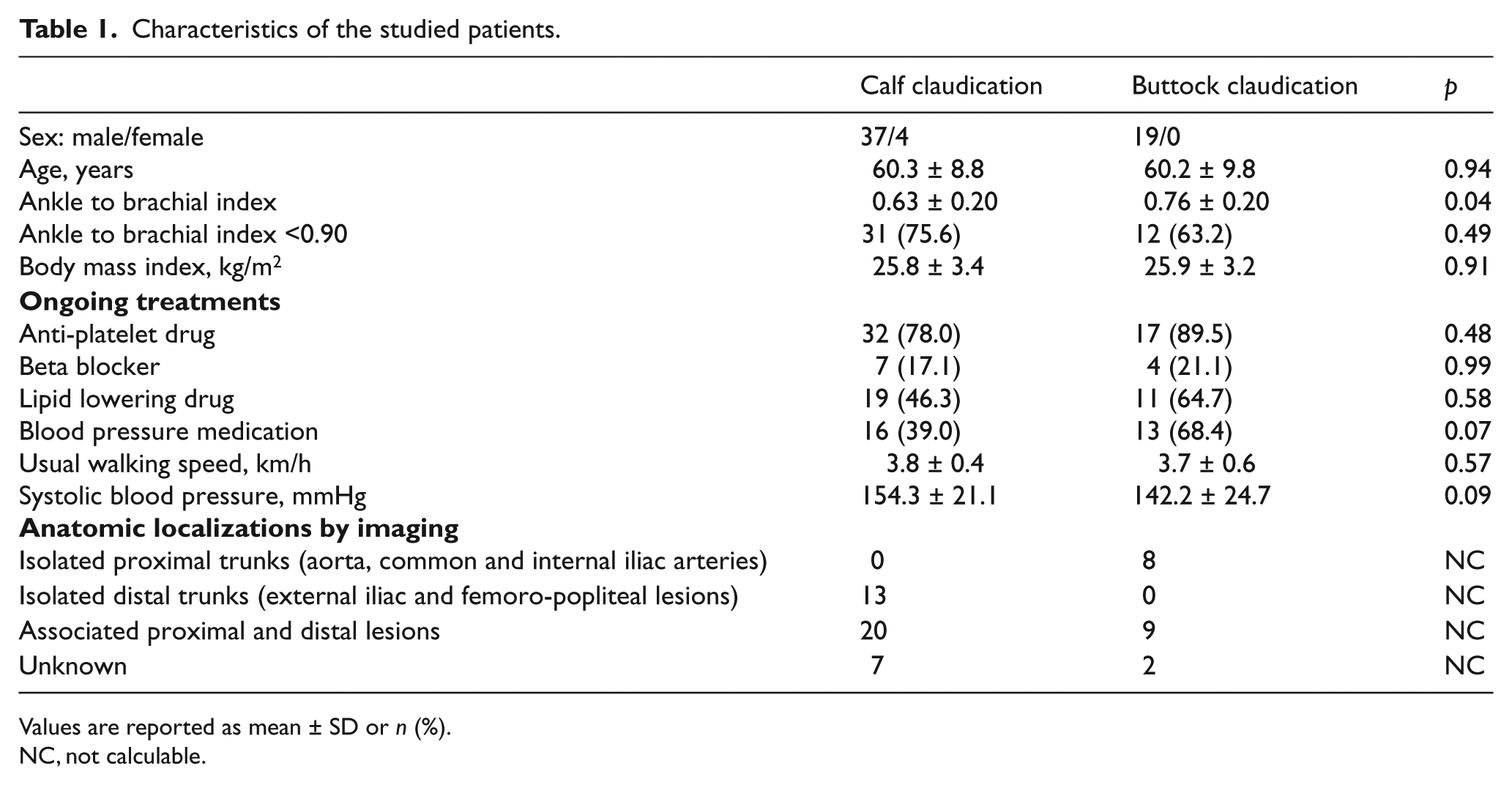
Values are reported as mean ± SD or n (%).
NC, not calculable.
In patients with proximal ischemia, imaging showed significant stenosis or occlusion on the aorta, common iliac or internal iliac arteries in all patients, with (n=9) or without (n=8) associated mild to moderate external iliac or femoro-popliteal lesions.
In patients with distal ischemia, imaging showed: external iliac or femoro-popliteal stenosis or occlusions with (n=2) or without (n=13) mild aorto-iliac lesions; external iliac and femoro-popliteal stenosis or occlusions with (n=11) or without (n=5) aortic or common iliac mild to moderate lesions; diffuse aortic, iliac and femoro-popliteal multiple stenoses (n=2).
Nine patients could not be analyzed due to incomplete information, non-accessible data or absence of imaging: two in patients with proximal ischemia, seven in patients with distal ischemia.
Test results
We observed a significant correlation between pain rating versus DROP in the period of worsening pain (from PAINapp to PAINmax) and in the recovery period (from PAINmax to PAINrel) (Figures 3 and 4). R2 coefficients calculated with non-linear analyses are given in Figures 3 and 4.
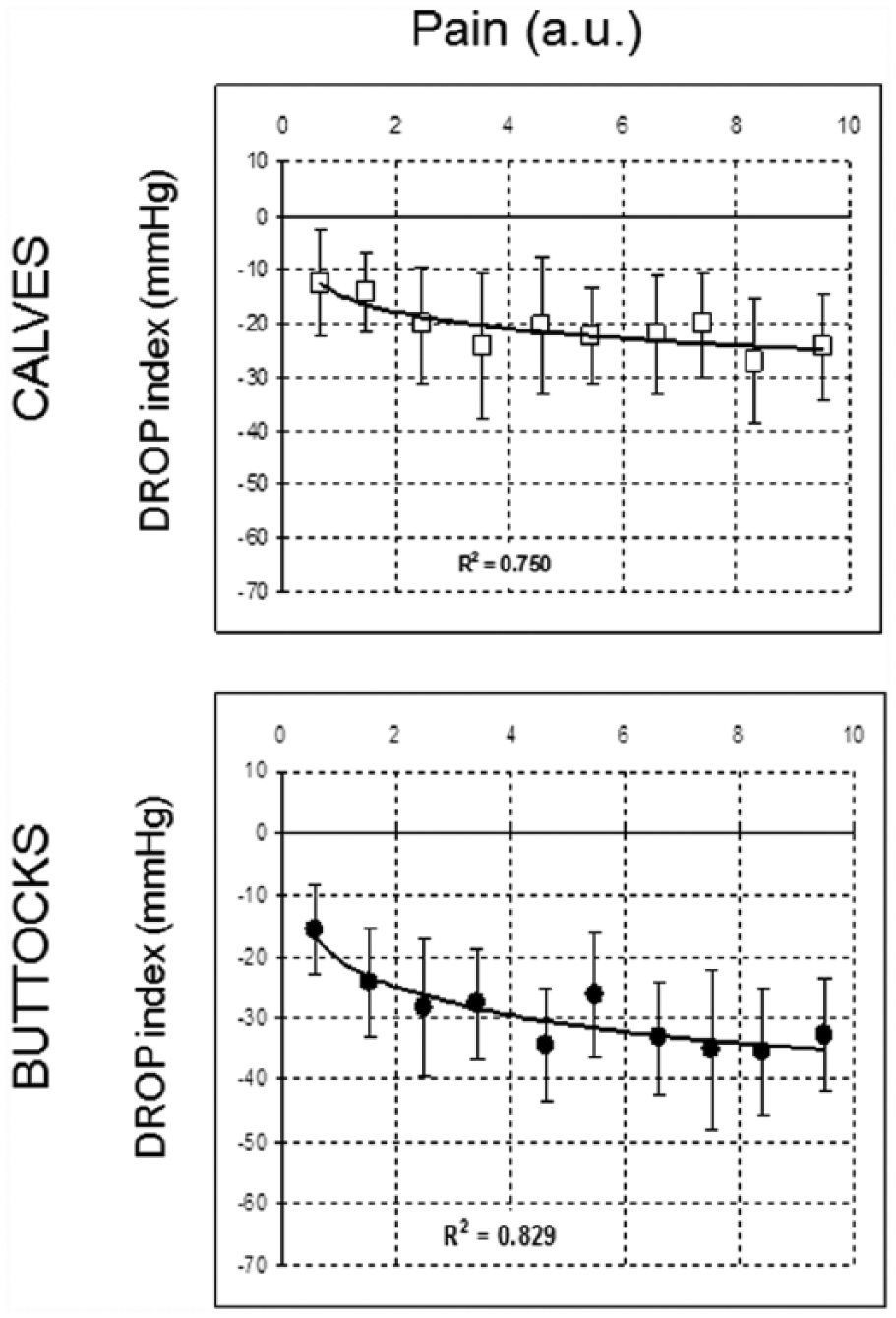
Correlation between pain rating versus DROP in the period of worsening pain (from pain appearance to maximal pain leading to stopping exercise). Vertical bars are given for the standard deviation at each point. (a.u., arbitrary unit; DROP, decrease from rest of oxygen pressure.)
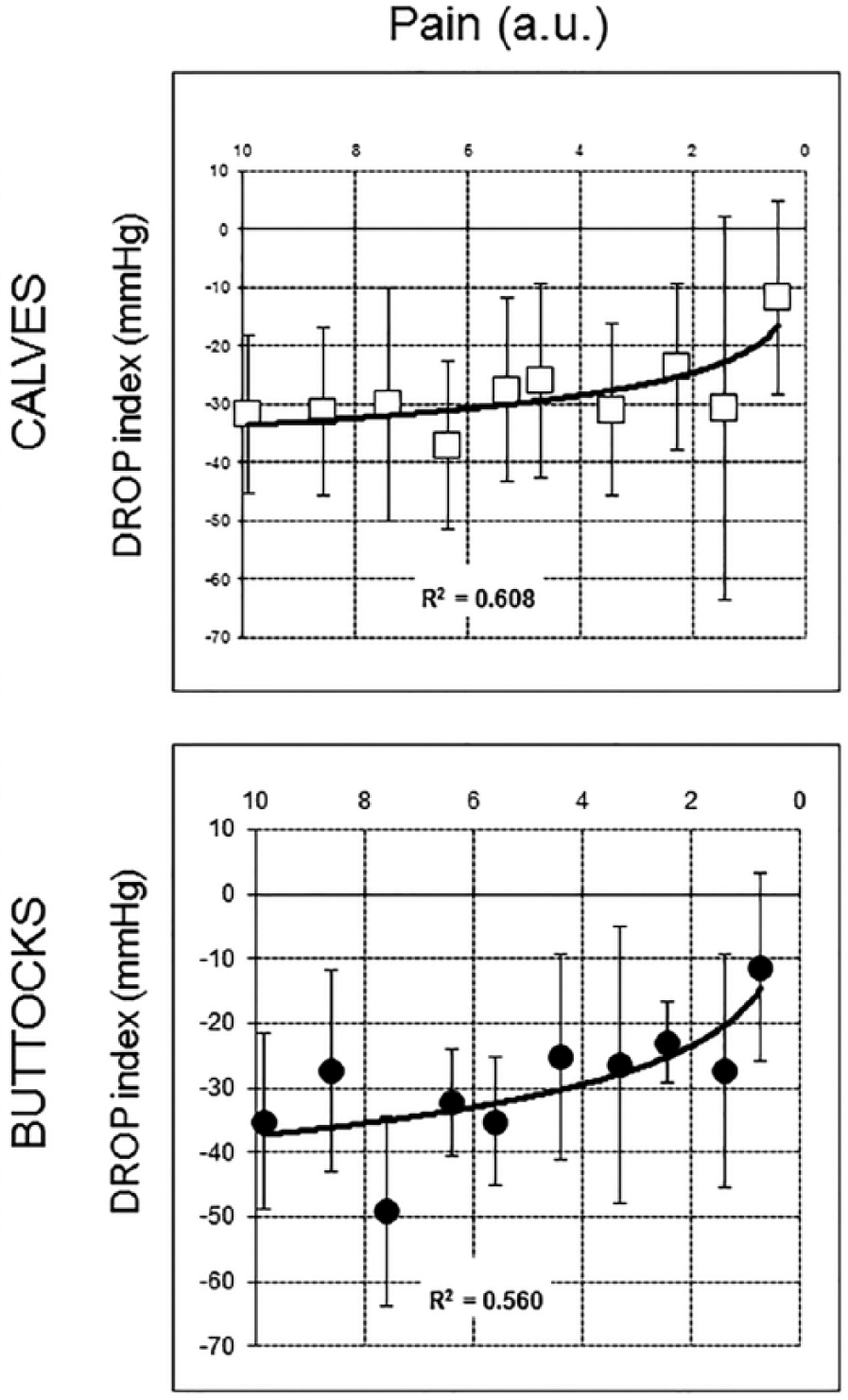
Correlation between pain rating versus DROP in the recovery period (from maximal pain leading to stopping exercise to pain departure). Vertical bars are given for the standard deviation at each point. (a.u., arbitrary unit; DROP, decrease from rest of oxygen pressure.)
The hemodynamic values at which pain appeared or disappeared were heterogeneous in the population, as shown in Table 2. On average, there was no statistical difference for the DROP at PAINapp between patients with proximal claudication and those with distal claudication. No differences were observed at PAINmax or PAINrel for DROP indices (Table 2). As shown in Table 2, DROP indices significantly decreased from their respective resting values at both PAINapp and PAINrel (p < 0.01).
DROP values in the calves and buttocks for patients with distal and proximal claudication, respectively.
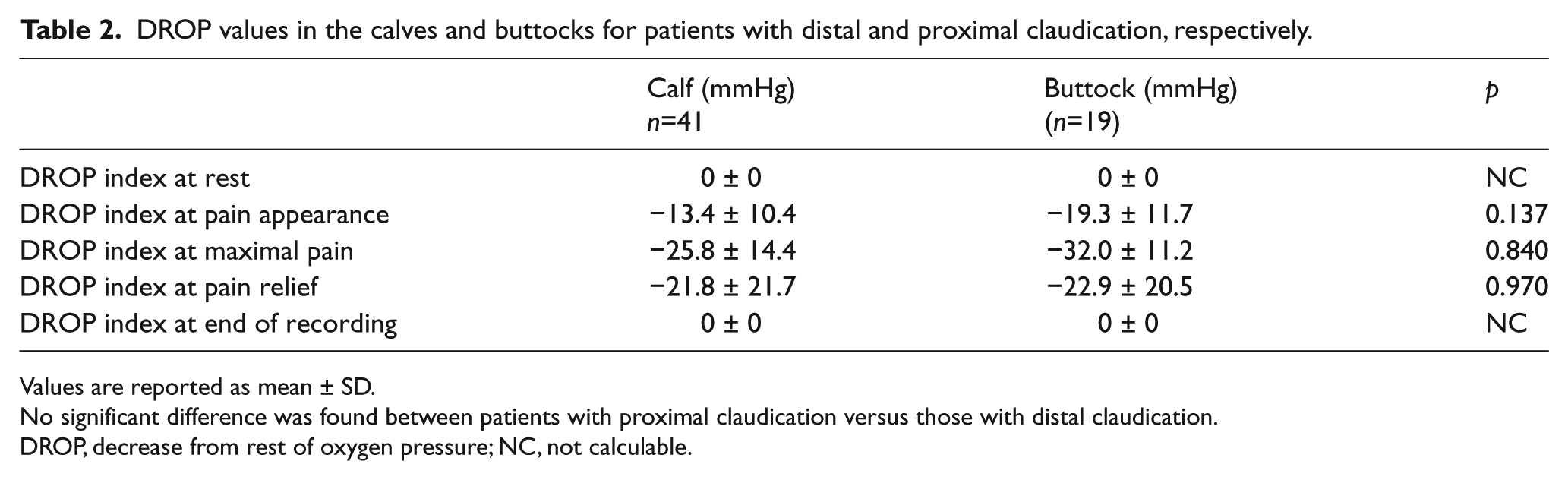
Values are reported as mean ± SD.
No significant difference was found between patients with proximal claudication versus those with distal claudication.
DROP, decrease from rest of oxygen pressure; NC, not calculable.
Discussion
Clinical issues
Although DROP at PAINapp and PAINmax were variable from one subject to another, ischemia and pain did not occur simultaneously. On the one hand, significant ischemia (DROP decrease) was required for pain appearance. It is interesting to note that, on average, the DROP value at PAINapp for calves and for buttocks was close to ≤ −15 mmHg. That value was the one found as the optimal cut-off value to detect significant arteriographic lesions at both buttocks and calves.16,17 On the other hand, despite the persistence of a significant ischemia, pain disappeared, while it could have been expected to disappear only after hemodynamic normalization. Pain occurring in a few patients while DROP was still close to zero could appear surprising. One possible explanation could also be due to a technical problem. Indeed, an abrupt change in the pO2 (e.g. the pO2 in a gas chamber changed from pure N2 to room air) must result from an asymptotic response of tcpO2 electrodes to be measured. The time required for tcpO2 to reach 90% of the change in case of instantaneous change of the pO2 is approximately 20 seconds (i.e. 20 seconds after opening the nitrogen box to room air at 760 mmHg atmospheric pressure, tcpO2 will be 159 × 0.9 = 143 mmHg). Besides, in some patients, deep tissue (muscle) ischemia could be lower than ischemia measured at skin surface. Figure 2 is an illustration that tcpO2 kept decreasing while exercise was stopped, maybe because of this technical delay. Another possibility might have been that pain occurrence in some patients resulted from an associated non-vascular disease, although we did our best to exclude patients with known co-morbidities. If not of technical origin, the persistence of ischemia at the time of pain departure might explain why, after the initial walk was forced to stop, the subsequent walking distance following a period of rest to allow pain to disappear, was inversely related to the duration of the resting period. 18 This should likely be taken into account in rehabilitation programs, depending on whether one aims to induce prolonged ischemia or to allow a complete hemodynamic recovery before a second session of exercise is started. Another possibility explaining why pain and ischemia did not occur simultaneously might have been that pain occurrence in some patients resulted from an accumulation of metabolites, but if metabolite accumulation was the cause of pain, pain should have normalized later than the normalization of ischemia, which was not the case.
Our study shows a relationship between hemodynamic parameters and pain rating, which is consistent with the results of a previous study evaluating calf pain and intra-muscular oxygen partial pressure. 11 Some studies have also demonstrated the correlation between pain perception and the intensity of other nociceptive stimuli.19–21 Indeed, using pain stimulation by laser has shown a linear relationship between laser intensity and average pain rating.20,21 Besides, a linear relationship between pain and the flexion reflex20,21 and a correlation between pain perception and heat stimulus 22 have also been demonstrated. It is noteworthy that, in our study, we found a correlation with a non-linear model.
Contrary to our hypothesis, we found no difference in the severity of ischemia at PAINapp between patients with walking-induced proximal (buttock) pain and patients with distal (calf) pain. This likely results from the expected high variability of individual values.23–25 The hypothesis was consistent with a difference in muscle fiber types between calves and buttocks. 26 Indeed, fiber types differ from one muscle to another. Although the muscle fiber type composition of the gastrocnemius is reported to be quite similar to the gluteus maximus, a clear difference is reported for the soleus muscle. The gluteus maximus and gastrocnemius contain approximately 50% of type I fibers, whereas the soleus contains nearly 90% of such fibers. Type I fibers are known to have an oxidative metabolism, which entails higher dependency on oxygen supply. The high proportion of type I fibers in the soleus muscle could have been responsible for pain occurring earlier at calf level (smaller tcpO2 decrease or DROP value) than at buttock level. This was not the case but it might have been due to a lack of power in the present study. Nevertheless, isolated proximal claudication is relatively rare and exclusion criteria severely reduced the number of studied patients. However, this study remains the very first attempt to analyze the relationship of hemodynamic parameters and pain rating in proximal versus distal claudication.
Limitations
Exercise-related pain in PAD is assumed to result from a mismatch between the oxygen demand of and supply to exercising muscles. In stage 2 (Fontaine’s classification) / stage 1 to 3 (Rutherford’s classification) PAD, oxygen supply is sufficient to cover resting metabolism, but during exercise the increase in blood flow is insufficient to cover the muscle oxygen demand increase. On the one hand, exercise tcpO2 is an original tool with which to monitor RBFI throughout the period of rest, exercise and recovery. The calculation of the DROP index allows the variability of absolute resting values to be dispensed with and has shown high concordance with underlying arterial lesions at both the proximal and the distal levels.7,16,17,27 On the other hand, VAS has been challenged as a method to evaluate chronic pain. 28 We think that, here, VAS is appropriate because claudication is not a chronic pain but an acute one repeatedly occurring during a chronic disease. Previously, a good reliability of VAS for acute pain measurement 29 has been shown.
TcpO2 evaluates skin oxygen pressure, which is an approximation of regional blood flow impairment and not a direct measure of muscle oxygen content. As calf muscle flow and calf skin flow are both supplied by the femoro-popliteal axis, it is very unlikely that skin could be ischemic without muscle flow impairment. On the contrary, gluteal arteries vascularize skin and muscles at the buttock, but we previously showed that buttock tcpO2 changes are partly dependent on ipsilateral lumbar artery patency. 30 In normal subjects, lumbar arteries are not expected to be involved in gluteus maximus vascularization. As a consequence, in case of lumbar artery occlusion, skin ischemia could be more severe than muscle ischemia and a tcpO2 fall at skin buttock level could cause few symptoms . The small non-significant difference in ischemia to pain relationship in patients with buttock claudication versus those with calf claudication might partly be of technical origin. Anyway, to date, no alternative technique is available, specifically at the buttock where near-infra-red spectroscopy has shown poor diagnostic performances. 31 Another limitation could be the difference of subcutaneous fat thickness between calf and buttock – although we believe that it is clearly a limitation for absolute tcpO2 value analysis but clearly not a limitation for DROP results. Indeed, the specific interest of DROP calculation is to get rid of the transcutaneous gradient difference that exists with different probe positions (assuming that the gradient is relatively stable with time). The absence of difference between the two groups could be also due to the very strict selection of patients, which has been responsible for a lack of power. Indeed, from the results of the present study, the required number of subjects to find a difference between the two groups should have been at least three times as great.
Finally, it is likely that the results observed in the present study are specific to the protocol used and that a different exercise procedure would have given different results. Further experiments are required to compare various slopes or speeds and their effects over proximal versus distal exercise-induced pain. From our experience, we estimate that patients with proximal and distal ischemia, that is to say buttocks associated with calf ischemia, preferentially complain of calf pain on a flat surface and buttock pain when climbing uphill, maybe because of different modifications of their respective oxygen demand in different walking situations.32–34
Conclusion
This work demonstrates that, on average, pain appears only after for a significant decrease of hemodynamic parameters and disappears while hemodynamic parameters are not normalized. Nevertheless, we found no statistical difference for DROP indexes at predefined endpoints between patients with proximal claudication and those with distal claudication. Also, the intensity of ischemia (DROP tcpO2) changes and pain rating changes are highly correlated. The tcpO2 technique might appear an attractive tool to clarify the debate on whether PAD patients with claudication should be encouraged to walk below or over their pain threshold for pain appearance and/or should be recommended to wait for hemodynamic normalization rather than pain departure. Finally, clinical differences observed between patients with proximal versus distal claudication do not seem to rely on differences in the pain rating to ischemia intensity relationship.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.