
Abstract
Supervised exercise therapy (SET) is a Class IA recommendation for the management of claudication from peripheral artery disease (PAD), 1 but is underutilized 2 despite gaining coverage approval from the Centers for Medicare & Medicaid Services (CMS) in June 2017. This study evaluated the utilization rate of SET from 2017 to 2021.
The study was approved by the institutional review board of the Beth Israel Deaconess Medical Center. Patients with a Current Procedural Terminology (CPT) code for SET (93668) or International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code for claudication between June 1, 2017 and December 31, 2021 in the 100% CMS Institutional Outpatient File were included. Baseline characteristics and co-morbidities were obtained via a 1-year retrospective review in the MEDPAR, Carrier, and Chronic Condition Warehouse files. Outcomes included 1-year all-cause death and lower-extremity revascularization.
Patients with claudication were divided by the presence or absence of a SET CPT code. Categorical variables were reported as frequencies and proportions and compared with chi-squared or Fisher’s exact tests, as appropriate. To account for baseline differences between patients, the propensity score for receiving SET was calculated for each patient using all baseline characteristics. Each patient enrolled in SET was then matched using the propensity score to the three nearest unexposed patients. Cox regression was then used to evaluate the association between SET and outcomes in the matched population. Fine-Gray methods were used to account for the competing risk of death for nondeath outcomes and subdistribution hazard ratios (SHRs) were estimated. Statistical significance was defined as p < 0.05.
Among 348,213 patients with a diagnosis of claudication, 6254 (1.8%) were enrolled in SET during the study period. Of those enrolled, 1114 (17.8%) underwent lower-extremity revascularization during the 1-year retrospective review period. The median number of SET sessions attended was 20 (IQR 9–31), and 629 patients (10.1%) completed the program (36 sessions). Compared with those not enrolled (n = 341,959 [98.2%]), patients enrolled in SET were slightly older (73.4 ± 8.0 vs 72.8 ± 9.1 years), more likely to be White (87.4% vs 84.0%), and less likely to be Black (8.8% vs 10.6%), dually enrolled in Medicaid (11.2% vs 20.6%), and female (37.6% vs 42.0%). The percentage of patients with claudication enrolled in SET by region during the study period was: Northeast 1.6%, South Atlantic 1.5%, Midwest 2.6%, South 1.1%, Mountain 2.2%, Pacific 2.0%, and Other 0.3% (Figure 1). Over 73% of total patients enrolled in SET were from the Midwest (44.0%), South Atlantic (15.1%), or Northeast (14.6%) regions of the United States. Only 13.4% of patients enrolled in SET were from the South region of the United States, whereas patients from the South region comprised 21.1% of the patients not enrolled in a SET group.
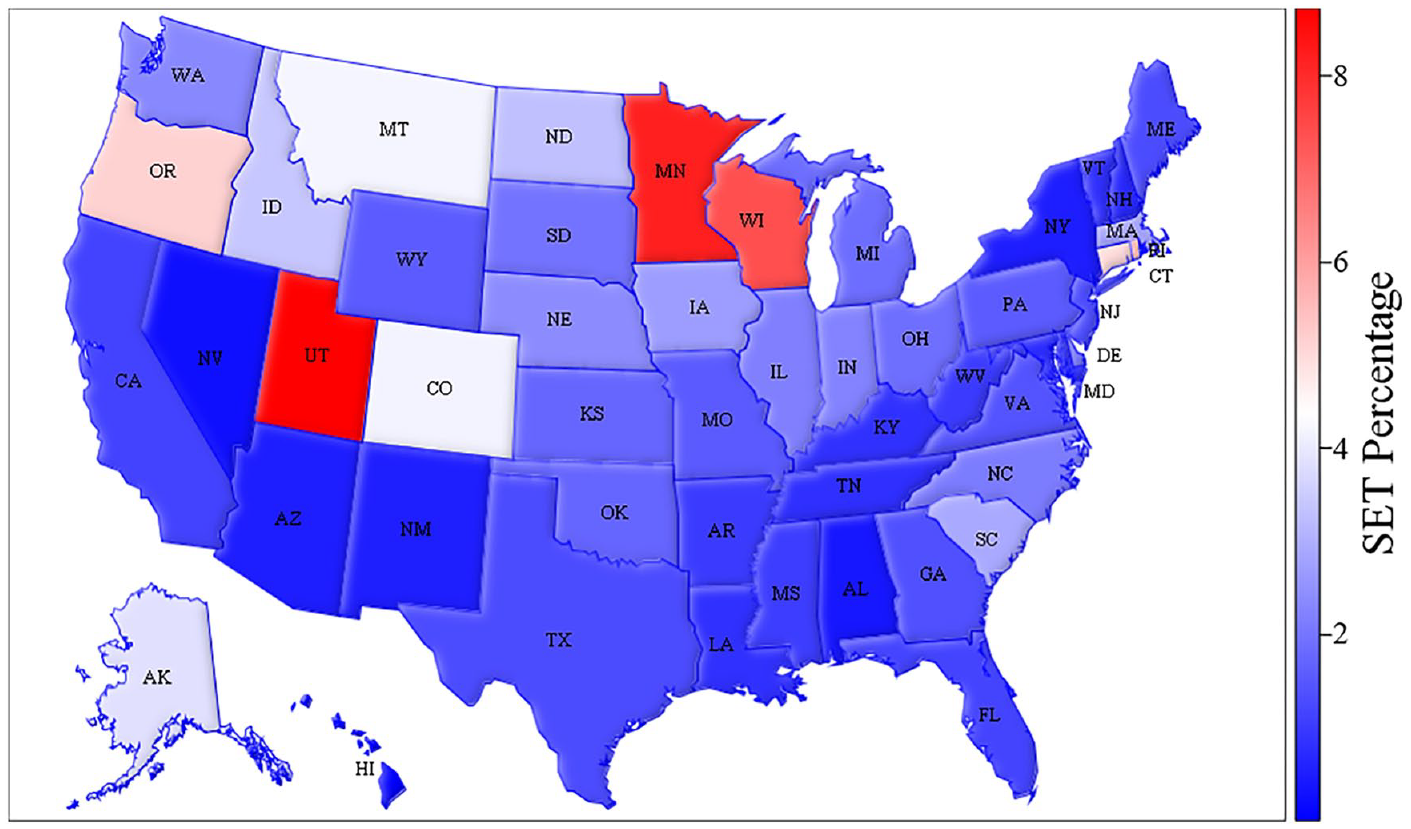
Heat map of supervised exercise therapy (SET) utilization between 2017 and 2021 among Medicare beneficiaries with claudication by state.
Patients enrolled in SET were followed for a median of 666 days (IQR 244–982 days) and patients not enrolled in SET were followed for a median of 720 days (IQR 304–1164 days). The 1-year cumulative incidences of endovascular and surgical lower-extremity revascularization were 14.6% and 4.4%, respectively. Predictors of SET enrollment were a history of ischemic heart disease (odds ratio [OR] 1.16, 95% CI 1.08–1.24, p< 0.0001), hyperlipidemia (OR 1.40, 95% CI 1.26–1.56, p < 0.0001), and prior surgical lower-extremity revascularization (OR 1.62, 95% CI 1.43–1.84, p < 0.0001). Baseline characteristics were all balanced after matching (p ⩾ 0.05 for all comparisons). In the matched cohort analysis, risk of endovascular or surgical lower-extremity revascularization was significantly lower among those who were enrolled in SET (endovascular: SHR 0.50, 95% CI 0.46–0.53, p < 0.0001; surgical: SHR 0.47, 95% CI 0.41–0.53, p < 0.0001).
This study of Medicare beneficiaries with claudication found persistently low utilization of SET more than 4 years after reimbursement was approved by CMS (1.3% of patients with claudication in the first 19 months after approval 2 and 1.8% during the current study period). Patients enrolled in SET differed in race, sex, socioeconomic status, and geographic region compared with those not enrolled, suggesting ongoing disparities in referral patterns. Only 10.1% of patients completed the full 36-session program. In our experience, the barriers limiting in-person attendance three times per week for SET are similar to those described in cardiac rehabilitation. 3 Additionally, among the patients enrolled in SET, less than 18% were enrolled following a lower-extremity revascularization procedure.
These data have important implications. First, it appears that despite reimbursement by CMS, barriers to accessing SET remain. Geography appears to be a particular discriminator, and alternative approaches including home-based programs may be required for patients without local access. Second, race- and income-based disparities in the utilization of SET have persisted since the initial rollout. Additional initiatives and incentives are needed to increase access to and utilization of this guideline-recommended intervention. Third, potential areas of investment and growth to improve function and quality of life for patients with claudication include increasing overall session adherence and enrollment following lower-extremity revascularization. 4 Limitations of this study include the small number of patients enrolled in SET, the low event rates, and treatment selection bias among those treated with lower-extremity revascularization.
In summary, SET remains underutilized in patients with symptomatic PAD despite a Class IA consensus guideline recommendation and coverage by CMS. Efforts to improve awareness, access, and adherence are needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was funded by the Smith Center for Outcomes Research in Cardiology. Dr Secemsky is supported by NIH/NHLBI K23 HL150290 and Harvard Medical School’s Shore Faculty Development Award.