
Abstract
Background:
Medial arterial calcification (MAC) is a vascular disease distinct from atherosclerosis. Recently, several studies have demonstrated that MAC is an important marker of cardiovascular events. We aim to assess the presence of MAC during ultrasound screening of lower-limb vasculature and its association with both cardiovascular (CV) and lower-limb events in patients with type-2 diabetes.
Methods:
A retrospective cohort study was conducted on 1119 patients with type-2 diabetes free from CV disease. A CV work-up, including vascular ultrasound, was performed for each patient. The presence of MAC was assessed on posterior tibial arteries and ankle–brachial index (ABI) was measured. Major acute CV events (MACEs) and lower-limb events (MALEs) were recorded as a composite endpoint for a 5-year period.
Results:
We identified MAC among 212 (18.9%) patients. The independent determinants of MAC were age and diabetic retinopathy. Over a period of 5 years, 125 MACEs and 22 MALEs occurred. MAC was significantly associated with the composite outcome MACE + MALE (HR = 1.94; 95% CI: 1.23, 3.08, p = 0.005) or with MACE (HR = 1.85; 95% CI: 1.16, 2.95, p = 0.010). Adjusted for ABI and diabetic foot wound, MAC remained a determinant of MALE (HR = 5.49; 95% CI: 2.19, 13.76, p < 0.001). Considering each ABI group, MAC was associated with both MACE and MALE in the normal ABI group.
Conclusions:
Ultrasound-detected MAC on tibial arteries seems to be a determinant of both CV and lower-limb events, independent from ABI. MAC helps to refine the CV risk in patients with normal ABI.
Keywords
Background
Medial artery calcification (MAC), a vascular disease distinct from atherosclerosis, results in a progressive and complex process of calcium deposition of the medial layer in the arterial wall. It was commonly considered as a nonsignificant finding. However, several studies now demonstrate that MAC is an important marker of cardiovascular events,1–5 although its pathogenesis differs from atherosclerosis. MAC is more frequent in patients with type-2 diabetes (T2D),1,2,6 chronic kidney disease (CKD), 7 and with aging. 8 In patients with T2D, cardiovascular risk estimation is essential for the management, and the identification of subclinical atherosclerotic disease is recommended for risk stratification. Nevertheless, the prognostic value of MAC screening is understudied. The ankle–brachial index (ABI) is often used as an easily accessible marker able to detect not only peripheral artery disease (PAD), when ABI is low (< 0.90), but also MAC when it is very high (> 1.40) due to stiffened arteries secondary to MAC. 9 ABI is known to be an independent marker of cardiovascular morbidity and mortality.10–14 Nam et al. showed that diabetes was the most important factor affecting the validity of ABI in the diagnosis of PAD because the arterial stiffening related to MAC can falsely increase ABI values. 15 Some past and recent studies proposed MAC screening using computed tomography (CT) scanning as a risk stratifier.16,17 However, this requires irradiating imaging techniques whereas ultrasound can also easily detect MAC. Also, the prognostic interest of MAC to assess both the general cardiovascular risk as well as the lower-limb risk needs further investigations.
We hypothesized that MAC detected by ultrasound is an independent marker of cardiovascular and lower-limb events in patients with T2D free from clinical cardiovascular disease.
Methods
Study design
We performed a retrospective study of asymptomatic T2D patients referred to our center between January 2007 and December 2016 for cardiovascular screening. No ethical committee authorization was required in France during the subject recruitment period. Patients with type-1 diabetes were excluded from the study. We also excluded patients with a prior history of cardiovascular disease and those with cardiovascular symptoms during the first evaluation. Patients with missing data regarding ultrasound assessment of tibial arteries were excluded.
Data collection
Information on sociodemographic characteristics, risk factors, anthropometrics, and medication were collected using standardized questionnaires. Hypertension was defined as blood pressure ⩾ 140/90 or use of antihypertensive treatment. Dyslipidemia was defined by a total cholesterol > 240 mg/dL or triglycerides > 150 mg/dL or the use of lipid-lowering therapies. The closest biological tests, within the 6 months prior to the cardiovascular assessment, were collected from the electronic database of the hospital. A standard 12-lead electrocardiogram was performed for each patient. Four-limb blood pressure measurements using a conventional Doppler method were performed to determine the ABI. The thresholds of the ABI group were defined as: < 0.90 (low), between 0.90 and 1.40 (normal), and > 1.40 (high). For each patient, the lowest ABI of the two legs was selected as the patient’s ABI, unless one leg had normal ABI while the other had high ABI. 18 In the latter case, the higher ABI was selected to capture all abnormal ABIs. Beyond ABI, femoral and posterior tibial arteries have been assessed by ultrasound to detect plaques in the former and MAC in the latter. Our data on femoral plaques have already been published elsewhere. 19 MAC was diagnosed in the presence of continuous, double, hyper-echogenic lines (‘railways’) for at least 2 cm along the posterior tibial artery walls (Figure 1). MAC was determined at the point-of-care by clinicians who were not directly involved in the research at that time or the future outcomes of the patients. The operators were certified vascular physicians with a long experience in vascular ultrasound. The subject was defined ‘MAC+’ in the presence of such an image on at least one leg. All vascular ultrasounds were performed using a Philips iE33 ultrasound machine (Philips, Eindhoven, The Netherlands), with a 8−12 MHz linear vascular ultrasound probe. Other cardiovascular tests during the assessment included an electrocardiogram (ECG) and carotid ultrasound. After an initial assessment, the cardiovascular specialist decided if any additional cardiovascular work-up or treatment was necessary.
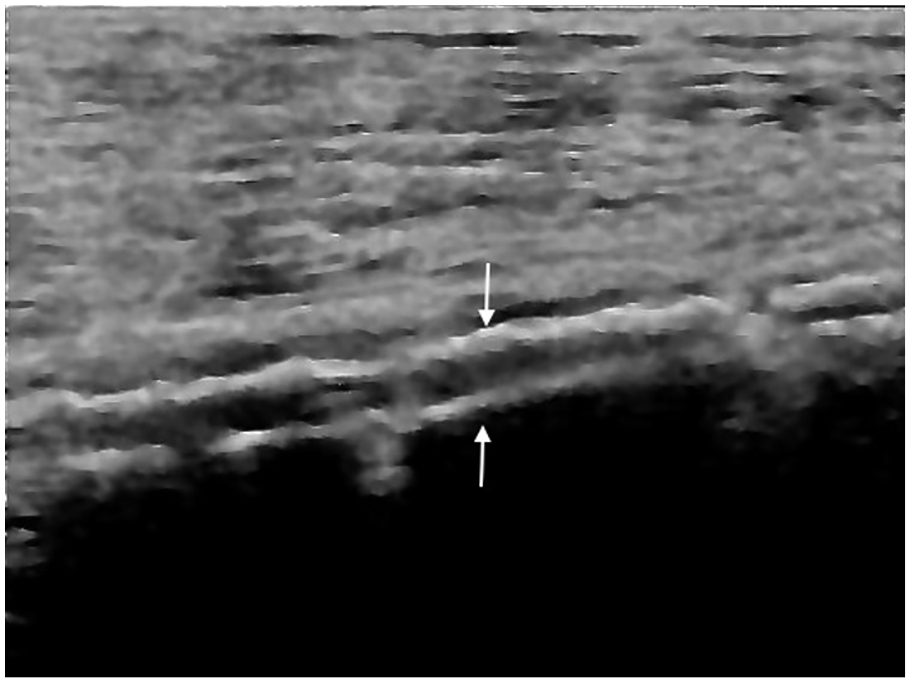
Continuous, double, hyper-echogenic lines (‘railways’; arrows) on posterior tibial artery walls corresponding to medial artery calcification.
Follow-up and outcomes
Follow-up data were collected through patients’ medical records and general practitioners were contacted when necessary. To avoid confounding factors occurring during long-term follow-up and with potential impact from mortality and cardiovascular events, the present analysis purposely focused on only a 5-year follow-up period. Deaths from noncardiovascular causes, loss to follow-up, and a follow-up duration > 5 years were analyzed as censored data. The occurrence of major adverse cardiovascular events (MACE) included cardiovascular death, stroke, acute coronary syndrome, and cardiac revascularization. Acute coronary syndrome was defined as ST-elevation myocardial infarction (STEMI), non-STEMI, and unstable angina. The major adverse lower-limb events (MALE) were first hospitalization for PAD, amputation, or peripheral revascularization.
The primary outcome was a composite endpoint of both cardiovascular events (MACE) and lower-limb events (MALE), as mentioned earlier. Secondary outcomes consisted of the study of MALE and MACE separately.
Diabetic retinopathy was considered to be present from the mild nonproliferative stage and CKD was defined according to KDIGO guidelines. 20 A diabetic foot wound was defined by the presence of a chronic pressure point unstageable wound with callus lasting more than 1 month.
Statistical analysis
Quantitative continuous variables and categorical variables are reported using means ± SD or number and percentage, respectively. Comparison between groups were performed using χ2 test, Fisher’s exact test, or Student’s t-test appropriately.
Log binomial regression analysis was used to determine independent factors associated with MAC. The selection of variables was carefully performed to avoid collinearity (e.g., obesity instead of body mass index (BMI), dyslipidemia instead of low-density lipoprotein (LDL)-cholesterol). MAC and ABI are indicators of peripheral arterial conditions and were not included together in the same model because of plausible collinearity. After univariate analysis, a subsequent multivariable model was used. Variables with a univariate p-value less than 0.20 were incorporated in the multivariable model. The 5-year event-free survival for MALE and MACE were generated using Kaplan–Meier analysis and compared using the Log-rank test. Independent markers of cardiovascular and peripheral events were assessed using the Cox proportional hazard model. Univariate analysis was performed for each variable. To investigate independent factors associated with the composite factor MACEs + MALEs and MACEs alone, multivariable analysis was used incorporating variables with a univariate p-value less than 0.05. Thereafter, we explored the interrelation between ABI and MAC to predict outcomes. Because of a lower number of MALE events, a full multivariable analysis could not be performed, so a staged multivariable analysis was performed: (1) adjustment for age and sex; (2) adjustment for ABI; and (3) adjustment for CKD and diabetic foot wound. Hazard ratios (HR), CIs, and p-values are reported. These models should be interpreted with caution because of the small number of events (n = 22).
All statistical analysis was performed with IBM SPSS Statistics, Version 26.0 (IBM Corp., Armonk, NY, USA). Statistical significance was considered as p < 0.05.
Results
From January 2007 to December 2016, 1873 patients with T2D had a cardiovascular screening and prevention consultation for the first time. Among them, 1119 (59.7%), in whom the presence or absence of MAC was assessed, were included in our study (Figure 2).
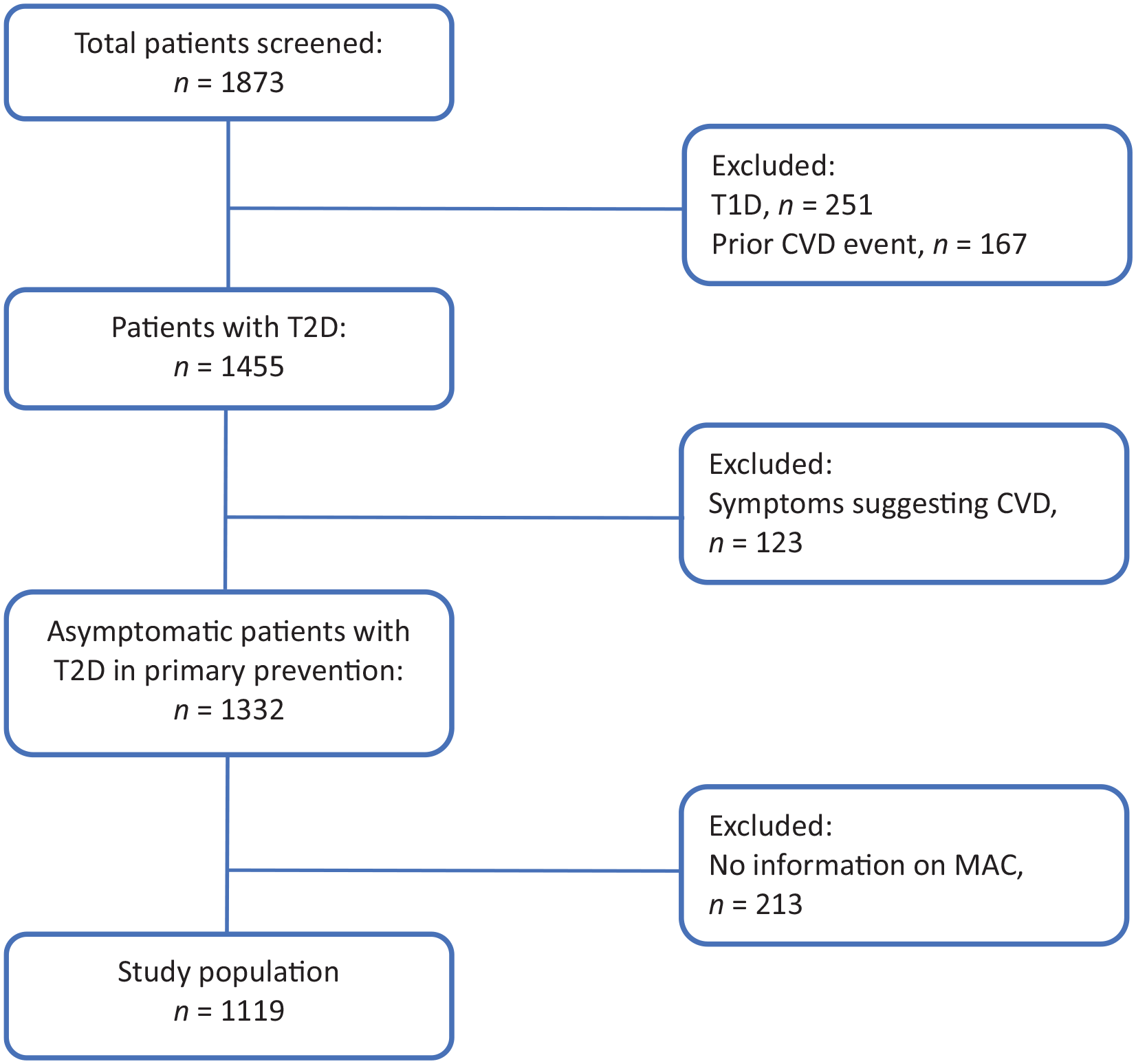
Patient selection flowchart.
General characteristics
Baseline characteristics of the population are described in Table 1. MAC was found in 212 patients (18.9%). Briefly, compared to patients without MAC (MAC–), MAC+ patients were more often men and significantly older with a longer T2D duration. They were more often on an insulin regimen and exhibited more complications of diabetes (diabetic retinopathy, CKD, diabetic foot). Mean glycated hemoglobin (HbA1c) was not statistically different between patients with and without MAC. CKD was significantly more present in patients MAC+.
Baseline characteristics of the population.
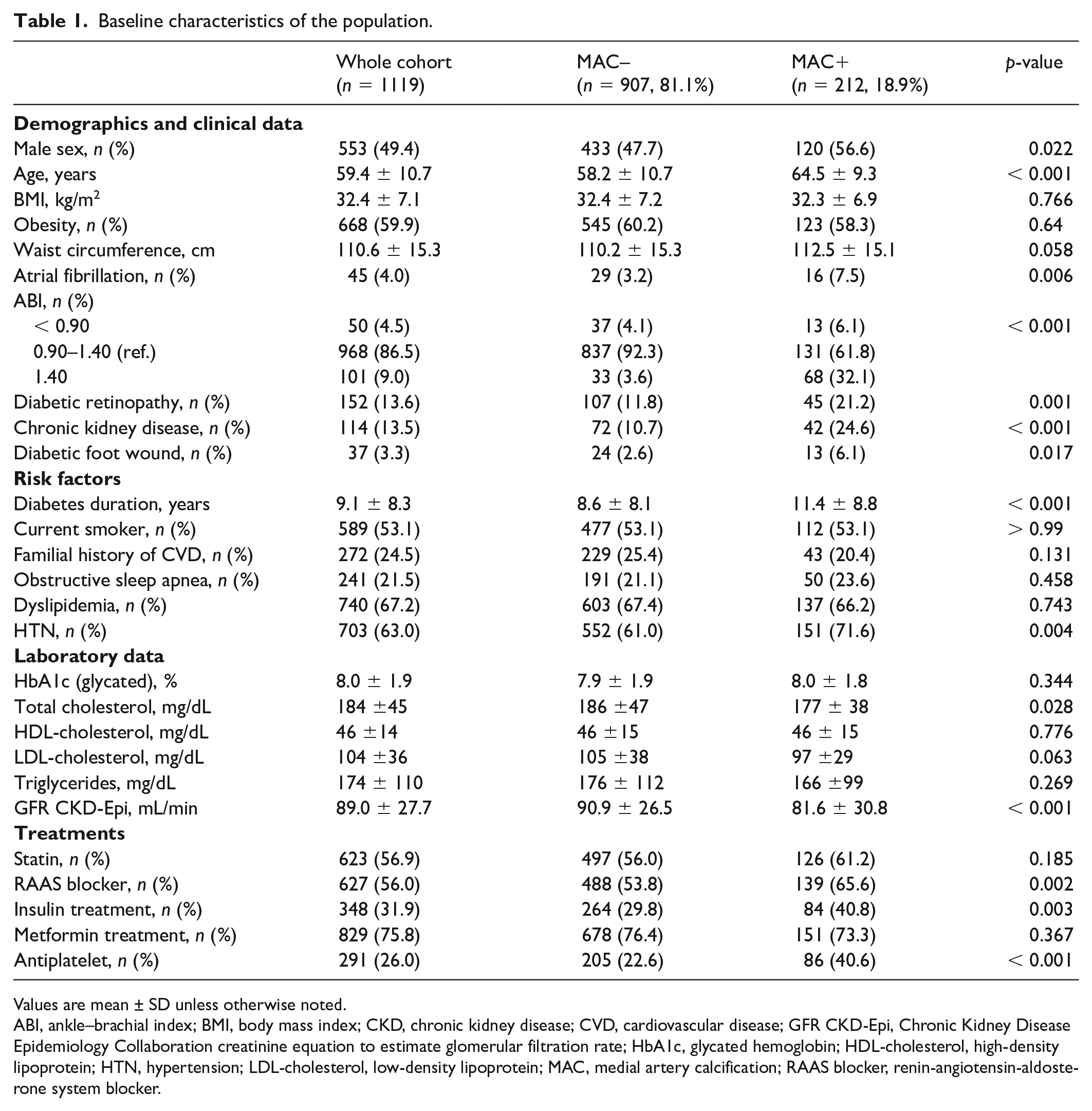
Values are mean ± SD unless otherwise noted.
ABI, ankle–brachial index; BMI, body mass index; CKD, chronic kidney disease; CVD, cardiovascular disease; GFR CKD-Epi, Chronic Kidney Disease Epidemiology Collaboration creatinine equation to estimate glomerular filtration rate; HbA1c, glycated hemoglobin; HDL-cholesterol, high-density lipoprotein; HTN, hypertension; LDL-cholesterol, low-density lipoprotein; MAC, medial artery calcification; RAAS blocker, renin-angiotensin-aldosterone system blocker.
The mean BMI was in the range of obesity for the whole cohort (32.4 ± 7.1 kg/m2), without significant difference between the two groups.
Figure 3 displays the distribution of MAC according to ABI classes. Among patients with high ABI, 67.3% of them had MAC detected by ultrasound. In MAC– patients, there was no significant difference in BMI or weight between those with or without high ABI (respectively, 32.6 ± 5.9 kg/m2 vs 32.4 ± 7.2 kg/m2, p = 0.879; 91.0 ± 17.7 kg vs 89.2 ± 20.1 kg, p = 0.136).
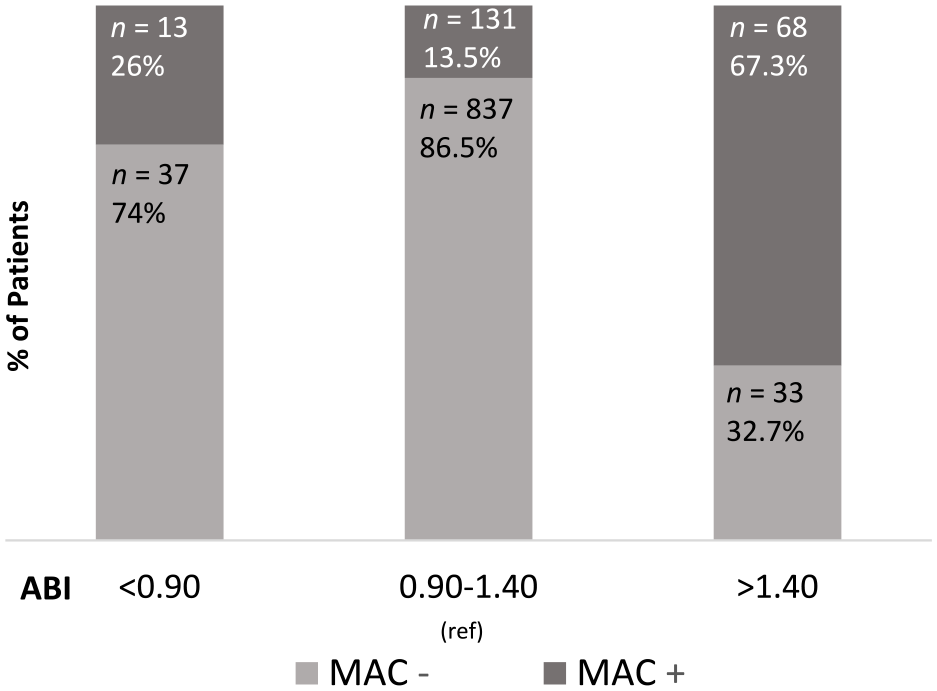
Distribution of MAC according to ABI classes.
Factors associated with MAC
Uni- and multivariable log binomial regression analyses are presented in Table 2. Age (β = 0.05; 95% CI: 0.03, 0.08, per year) and diabetic retinopathy (β = 0.61; 95% CI: 0.12, 1.10) were significantly and independently associated with MAC.
Factors associated with medial artery calcification in log binomial regression.
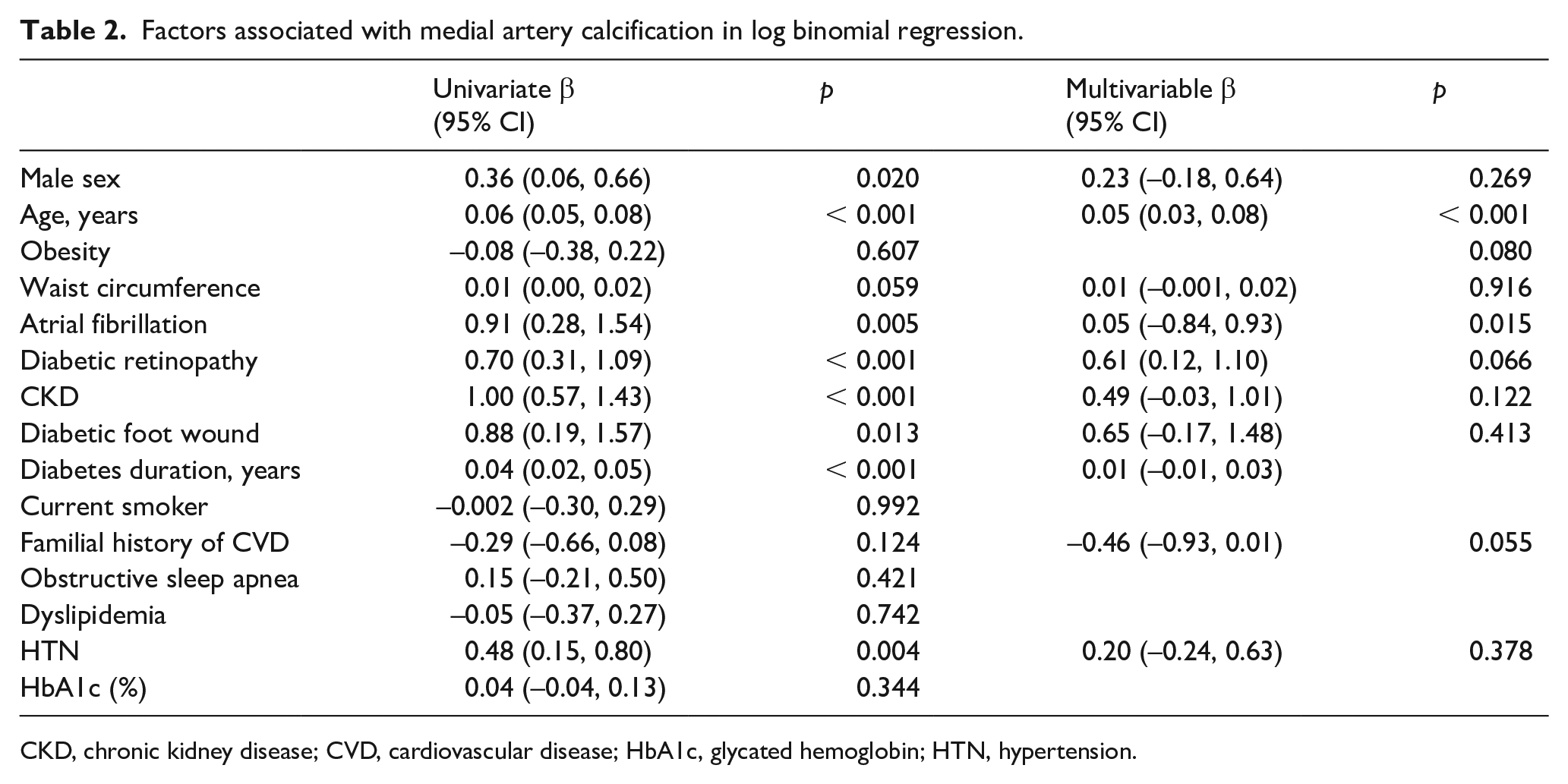
CKD, chronic kidney disease; CVD, cardiovascular disease; HbA1c, glycated hemoglobin; HTN, hypertension.
Association between MAC and MACEs + MALEs
Over a period of 5 years, a total of 147 events occurred in the cohort (125 MACEs and 22 MALEs), resulting in 128 composite events (only considering the first events for patients experiencing both MACE and MALE).
The composite events MACEs + MALEs occurred significantly (p < 0.001) more frequently in MAC+ than MAC– patients over time (Figure 4A). Using a Cox proportional hazard model, MAC was significantly associated with the composite outcome (HR = 1.94; 95% CI: 1.23, 3.08; Table 3).
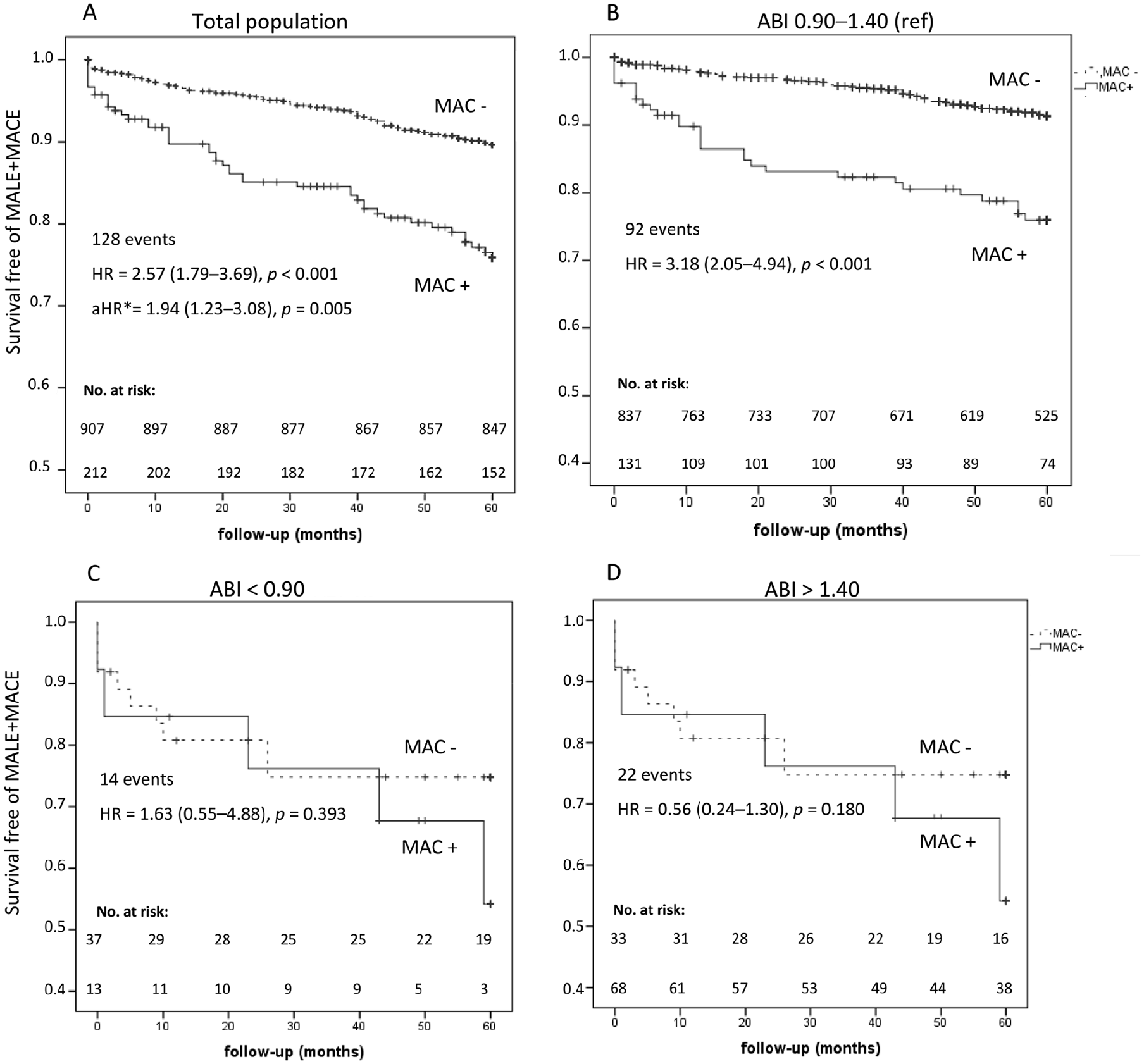
Outcomes of cardiovascular and peripheral artery events (MALE + MACE) according to MAC. (
Cox proportional hazard model to predict cardiovascular events and peripheral events (MACE + MALE).
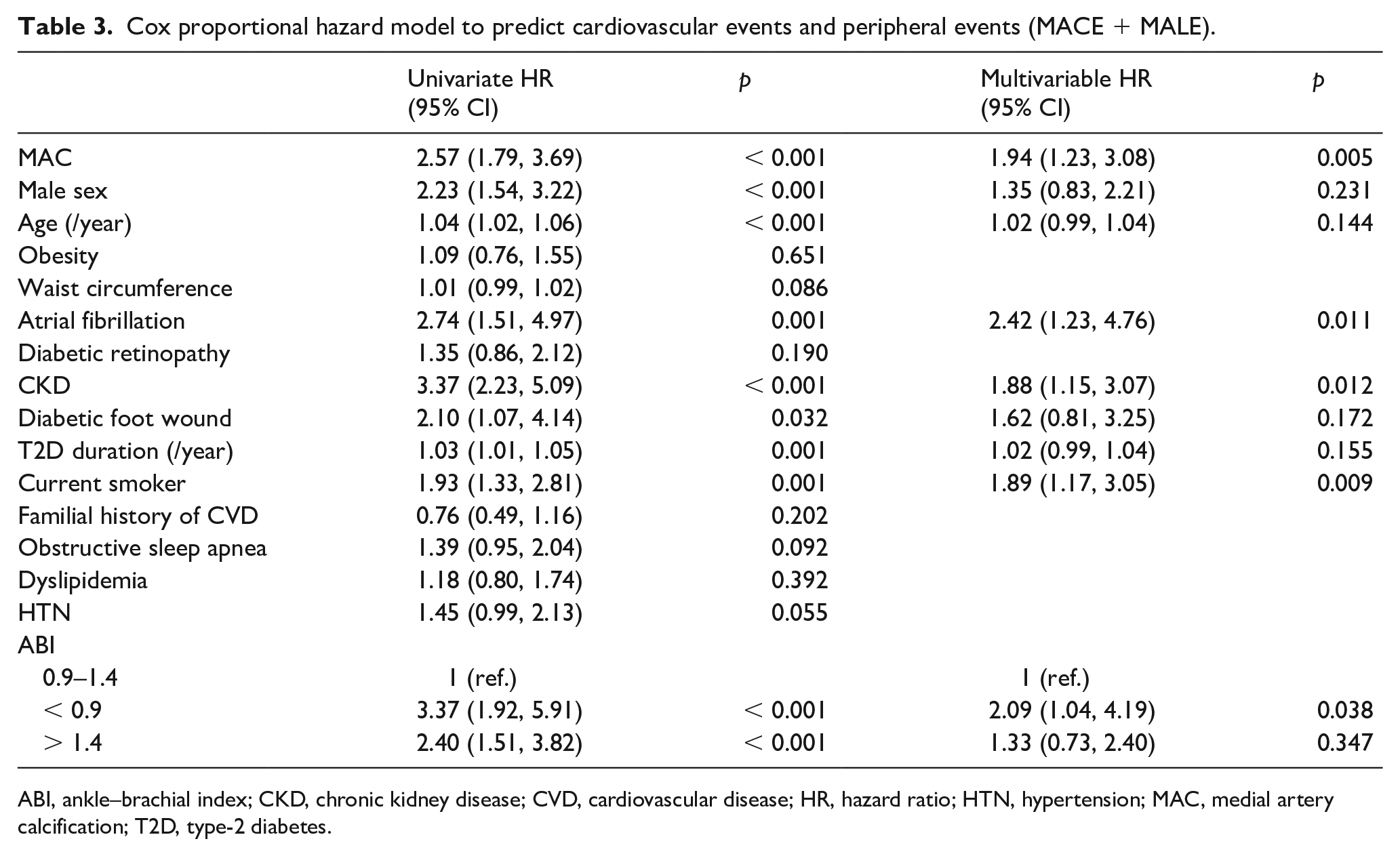
ABI, ankle–brachial index; CKD, chronic kidney disease; CVD, cardiovascular disease; HR, hazard ratio; HTN, hypertension; MAC, medial artery calcification; T2D, type-2 diabetes.
Considering each ABI group separately, the event-free survival in the normal ABI group was significantly decreased in the presence of MAC (p < 0.001; Figure 4B). In low and high ABI groups, the difference between MAC– and MAC+ patients did not reach statistical significance (Figures 4C and 4D).
Regarding MALEs, patients in the MAC+ group depicted significantly lower event-free survival (p < 0.001; Figure 5A). Using the Cox proportional hazard model, MAC was associated with MALEs in a first model adjusted for age and sex (HR = 4.86; 95% CI: 1.99, 11.87, p = 0.001). In further models, MAC remained associated with MALEs even after adjustment for ABI (HR = 5.49; 95% CI: 2.19, 13.76, p < 0.001), and after adjustment for CKD and the presence of diabetic foot wound (HR = 5.85; 2.12, 16.16, p = 0.001) (online supplemental data).
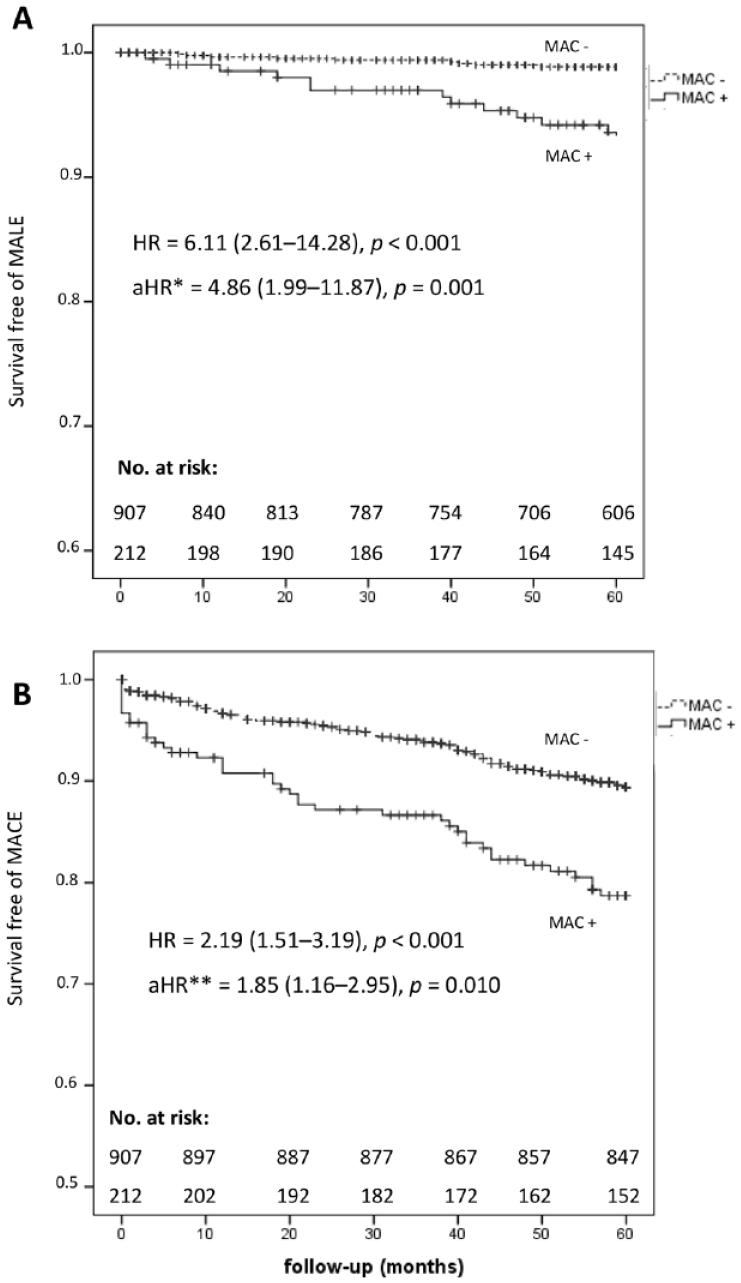
Outcomes of lower-limb and cardiovascular events according to MAC in the total population. (
When considering each ABI group separately, the presence of MAC remained a significant (p < 0.001) determinant of MALE in patients with normal ABI (age- and sex-adjusted HR = 4.46; 95% CI: 1.47, 13.7).
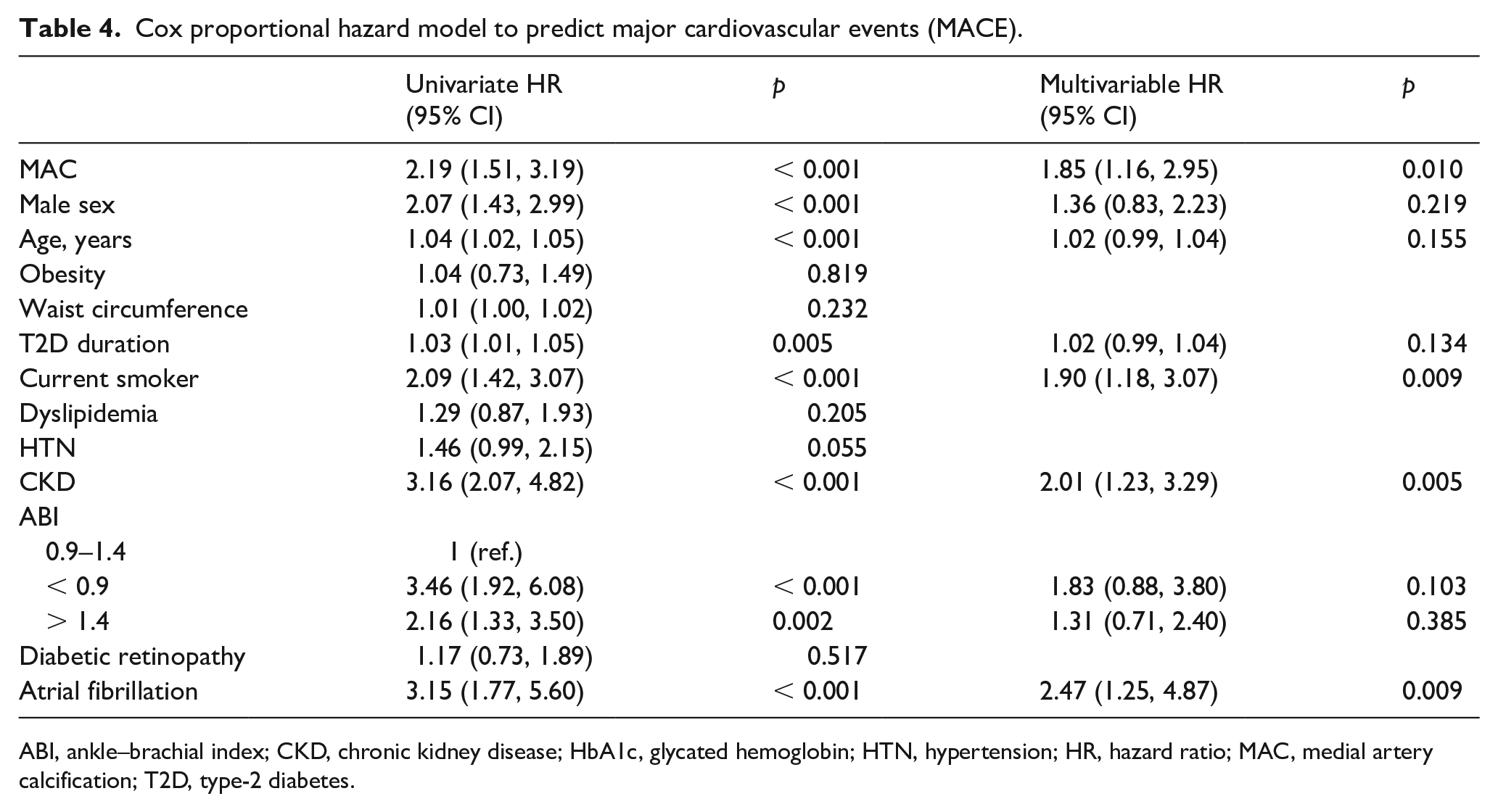
Regarding MACE, MAC was significantly (p < 0.001) associated with a lower event-free survival (Figure 5B). MAC was associated with MACE occurrence along with active smoking, CKD, and atrial fibrillation (HR = 1.85; 95% CI: 1.16, 2.95, p = 0.010; Table 4). Of note, the association of ABI with MACE was no longer significant in multivariable analysis. Among patients with normal ABI, those with MAC had a lower event-free survival, with an age- and sex-adjusted HR of 2.25 (1.40, 3.61), p = 0.001.
Cox proportional hazard model to predict major cardiovascular events (MACE).
ABI, ankle–brachial index; CKD, chronic kidney disease; HbA1c, glycated hemoglobin; HTN, hypertension; HR, hazard ratio; MAC, medial artery calcification; T2D, type-2 diabetes.
Discussion
Our study shows in a population with T2D naïve for any cardiovascular history that (1) almost one out of five patients exhibit ultrasound-identified MAC; (2) the proportion of MAC increases with age, longer duration of T2D, and the presence of CKD; and (3) MAC seems to be an independent determinant of MACEs and MALEs, even after adjustment for ABI or diabetic wound foot.
Data on the actual prevalence of MAC are scarce because many studies use ABI as a proxy of MAC. Our finding is in accordance with the existing literature. In patients with T2D, prevalence of radiological MAC varies from 17% to 42%,1,2 with a discrepancy probably explained by differences between the study populations, in terms of diabetes duration, history of cardiovascular disease, and number of cardiovascular risk factors.
Our study population reveals that MAC+ patients share the same characteristics as those classically reported in PAD. 21 Regarding MAC– patients, we hypothesized that high ABI in this population was related to a higher BMI. Tabara et al. showed that body weight and visceral fat area were significantly associated with high ABI, 22 and that appendicular muscle mass was a strong determinant of elevated ABI. 23 However, our study failed to find a statistical difference in BMI between MAC– patients with and without high ABI, and data about body composition are missing in our cohort.
The independent factors associated with MAC in multivariable analysis are those commonly described in the literature. As reported by many groups,1,6,24 age is a strong determinant with a 5% increase in risk per year. Unlike Everhart et al., 6 we have not found any significant association between diabetes duration and MAC in multivariable analysis. This may be explained, at least in part, by the fact that our cohort is composed of asymptomatic patients with a likely lower diabetes exposition. Diabetic retinopathy was independently associated with MAC, in line with previous studies.6,7,25–28 In addition, we found a trend towards an association between CKD and MAC. This highlights the importance of interaction between macrovascular and microvascular complications. Furthermore, in their longitudinal study on Pima Indians, Everhart et al. showed that radiological MAC diagnosed within the first 5 years after diagnosis of diabetes was predictive of microvascular complications. 6
Our study shows that MAC, located at the posterior tibial arteries, is significantly associated with cardiovascular events and limb events in a population of asymptomatic and CVD-free patients with T2D. The presence of MAC almost doubles the risk of occurrence of the composite endpoint in the whole cohort. MAC is associated with cardiovascular events, independent from other major markers, in particular low ABI. The role of ABI as a marker of cardiovascular disease and death was demonstrated in several studies.10–14 Interestingly, in the multivariable model for the occurrence of MACE, ABI was actually no longer significant, whereas MAC remained independently associated with MACE. Considering each ABI group, the predictive value of MAC remains significant in the normal ABI group (0.90–1.40). Yet, in this category of patients with lower cardiovascular risk, MAC enables us to refine the risk stratification and identify a subgroup of higher-risk patients in the presence of MAC, despite normal ABI. In multivariable analysis of the Cox hazard model, high ABI is not associated with the composite cardiovascular endpoint. Overall, in the entire cohort, MAC appears as a better risk predictor than high ABI, often considered as a proxy for MAC, albeit recently challenged. 17 Despite a good specificity, the study of Hoek et al. shows a poor positive predictive value of high ABI for the diagnosis of MAC. 17 In our study, only 67.3% of patients with high ABI had MAC. In turn, high ABI cannot capture all patients with MAC, as most (61.8%) of our patients with MAC actually had normal ABI. These results highlight the crucial role of ultrasound imaging for assessment of MAC and thereby cardiovascular risk stratification of subjects with normal ABI. Regarding limb events, MAC was found to be significantly associated, independently from ABI or diabetic foot wound. Using multislice CT, Guzman et al. showed that a tibial artery calcification score > 400 was the only predictor of major amputation in patients presenting with PAD. 16 Interestingly, in our study, MAC seemed to be a determinant for both MACE and MALE. Some authors previously reported the association of MAC and cardiovascular events1,29 but this is the first study to show interest in MAC to predict both MACE and MALE in patients with T2D without any clinical history of cardiovascular disease.
Study limitations
The main limitation of the study was the screening mode of MAC, which was limited to the posterior tibial arteries. However, the posterior tibial artery was chosen because of the higher prevalence of MAC in distal arteries, as extensive imaging of the whole lower-extremities arteries might be time-consuming and cumbersome. Everhart et al. reported that MAC originates from distal leg arteries and progresses proximally. 6 Somatic and autonomic diabetic neuropathy promotes medial vascular calcification,27,30,31 explaining the distal distribution of MAC. Some histological studies showed that infrapopliteal arteries have a higher burden of MAC than above-the-knee arteries, especially in the elderly, diabetic, and end-stage renal disease patients.32,33 Our study was not designed to evaluate the incremental value of the presence of MAC on posterior tibial arteries compared to femoral and carotid arteries. However, a recent review and meta-analysis showed that infrapopliteal MAC was significantly associated with the occurrence of lower-limb amputations in patients with diabetes. 34
There were no adjudication processes to determine the occurrence of MACE, MALE, or death.
The information about antivitamin K treatment, a significant inductor of MAC, 35 is not available in our study. Chronic atrial fibrillation, mostly treated with antivitamin K treatment, is more frequent in MAC+ patients compared to MAC– patients, but the association was no longer significant in multivariable analysis.
Another limitation is our inability to address the use of cardiovascular-protective antidiabetic drugs, such as the glucagon-like peptide-1 (GLP-1) receptor agonists and sodium-glucose cotransporter-2 (SGLT2) inhibitors. The latter were not available in our market or not widely used for this purpose during the study period.
Finally, it should be emphasized that the management of patients with T2D has evolved throughout the inclusion period (2007–2016) as many changes occurred in guidelines during that period.
Conclusion
The ultrasound screening of MAC is a nonirradiating technique, which can be easily implemented during a cardiovascular check-up of patients with diabetes. Our study shows that posterior tibial artery MAC is a factor associated with cardiovascular and limb events, independently of the ABI. MAC may refine the risk in patients with normal ABI. Our study suggests the use of ultrasound at the ankle arteries to detect MAC. Randomized trials are necessary to compare different treatment strategies to reduce the risk of MACE and MALE in patients with MAC.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231190433 – Supplemental material for Ultrasound-detected tibial artery calcification as a marker of cardiovascular and lower-limb risk in asymptomatic patients with type-2diabetes
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231190433 for Ultrasound-detected tibial artery calcification as a marker of cardiovascular and lower-limb risk in asymptomatic patients with type-2diabetes by Laurence Salle, Julien Magne, Angeladine Kenne Malaha, Lucie Chastaingt, Sophie Galinat, Anne Drutel, Philippe Lacroix, Marie-Pierre Teissier-Clément and Victor Aboyans in Vascular Medicine
Footnotes
Data availability
Datasets analyzed during the current study are available from the corresponding author upon request.
Declaration of conflicting interests
Victor Aboyans receives support from Amarin, AstraZeneca, Boehringer-Ingelheim, NovoNordisk. The other authors declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.