
Abstract

Keywords
Ankle–brachial index (ABI) is the standardized test for diagnosis of lower extremity peripheral artery disease (PAD), with high specificity and sensitivity for a resting-ABI threshold of 0.90 or less. 1 Post-exercise ABI (PEABI) is useful in establishing the diagnosis of lower extremity PAD in the symptomatic patient when resting ABIs are greater than 0.90. 2 In some clinical conditions (i.e. diabetes, renal insufficiency, and advanced age), the resting ABI measurement can be falsely within the normal range and, in these cases, the use of the toe–brachial index (TBI) is recommended to diagnose PAD. 2 For PEABI, commonly used diagnostic criteria are a pressure decrease of more than 30 mmHg or an ABI decrease of more than 20% from the resting value. For TBI, according to guidelines, the threshold value to diagnose the presence of PAD is less than 0.70. 2 We have previously shown that vascular medicine residents from four medical schools in France lack training to perform limb pressure measurements for the diagnosis of PAD. 3 That study was performed with only 19 residents, so it was not possible to know whether or not these results would have been similar in the whole country.
Therefore, we conducted a nationwide study to assess the knowledge of new first year vascular medicine residents in France (n = 44). During a single day of training in Paris, all 44 vascular medicine residents from 22 French medical schools completed a survey regarding their knowledge and training on PAD diagnostic tests. The paper survey was a French language, multiple-choice questionnaire with 30 items specifically developed to evaluate each resident’s prior experience and knowledge about the three main noninvasive tests for PAD screening: resting ABI, PEABI, and TBI (see online supplement). The questionnaire covered four topics: residents’ medical school, resting ABI, PEABI, and TBI. This study was approved by the ethics committee of Centre Hospitalier Université de Rennes and conducted according to French Health Research Authority guidance. A proportion comparison test, Fisher’s exact probability test (R software, version 3.6.0; R Foundation for Statistical Computing, Vienna, Austria), was used to compare the number of vascular medicine residents capable of performing ABI, PEABI, and TBI, according to the procedure, based on their experience and knowledge, as reported in the survey. A two-tailed p-value less than 0.05 was considered as statistically significant.
All 44 residents completed the questionnaire. They had all completed 8 months of vascular medicine training (over a period of 4 years) after 6 years of medical school. Vascular medicine residents who had previously performed at least one measurement for each test (ABI, PEABI or TBI) were considered ‘experienced’ in the respective test. Only four residents were experienced in all three tests. ‘Competent’ residents in respective tests were defined as having more than 50% correct answers for each test component of the questionnaire. Figure 1 displays the results.
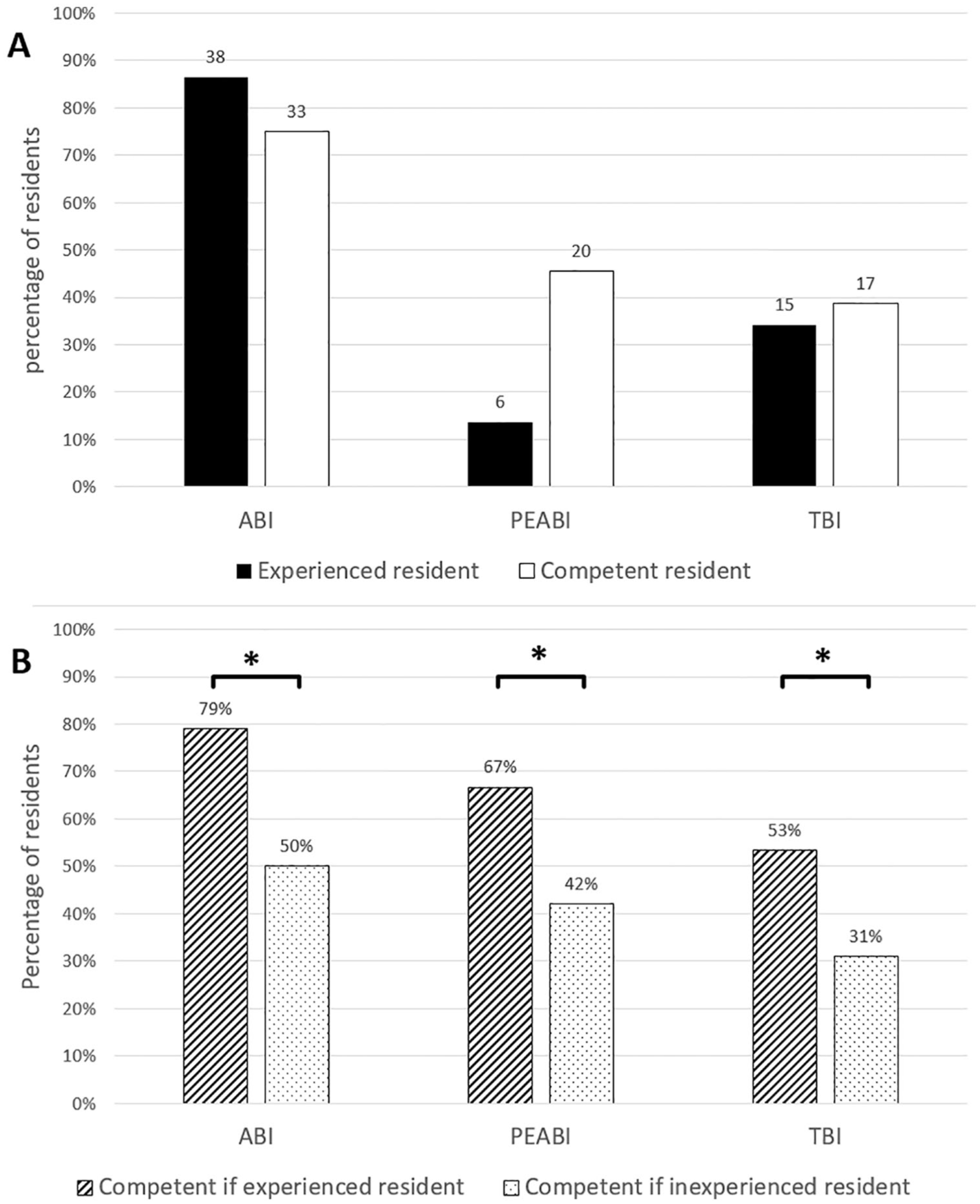
(a) Competence and experience of vascular residents. (b) Competence of vascular residents according to their experience.
Thirty-eight residents (86%) had previously performed a resting ABI measurement, only six residents (14%) had performed a PEABI, and 15 (34%) had performed a TBI. Experienced residents were statistically (p < 0.001) more competent in how to perform the three tests: ABI (79% vs 50%), PEABI (67% vs 42%), and TBI (53% vs 31%).
The number of residents who had performed more than 20 measurements was higher for resting ABI than for PEABI and TBI (84%, 5%, and 37%, respectively; p < 0.001 and p = 0.006, respectively) and significantly higher for TBI that PEABI (37% vs 5%; p = 0.04).
This study, based on a national survey, underscores that a significant lack of knowledge exists among French vascular medicine residents regarding not only the ABI procedure, as previously shown in the USA with internal medicine residents,4,5 but also the TBI and especially PEABI procedures. Furthermore, this nationwide assessment shows that vascular residents lack adequate practical knowledge on limb pressure measurements and it supports our belief that experienced residents were more competent than inexperienced residents. We have previously suggested that practical teaching would improve this competency.5,6
These results from France could be explained by the fact that bedside teaching regarding vascular disease in our medical schools is too limited. 6 Moreover, the lack of a high-quality evidence-base could explain the knowledge gap, especially for PEABI measurement, for which diagnostic thresholds and methods to perform the measure are not standardized.7–9
Based upon the findings of this survey and previously published literature, we suggest bedside teaching in combination with theoretical teaching for PAD assessments. Teaching should focus first on resting ABI measurement, then the technical aspects of TBI and PEABI measurement. This survey also invites vascular medicine mentors to confirm that their residents are truly competent in these important procedures.
Supplemental Material
10.1177_1358863X19867759_Supplementary_questionnaire – Supplemental material for Vascular medicine residents lack adequate training for limb pressure measurement: A nationwide survey in France
Supplemental material, 10.1177_1358863X19867759_Supplementary_questionnaire for Vascular medicine residents lack adequate training for limb pressure measurement: A nationwide survey in France by Damien Lanéelle, Clement Hoffmann, Olivier Stivalet, Loukman Omarjee and Guillaume Mahé in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.