
Abstract
Background:
Shared medical decision making requires patients’ understanding of their disease and its treatment options. Peripheral artery disease (PAD) is a condition for which preference-sensitive treatments are available, but for which little is known about patients’ knowledge and treatment preferences as it relates to specific treatment goals.
Methods:
In a prospective, multicenter registry that involved patients with PAD experiencing claudication, the PORTRAIT Knowledge and Preferences Survey was administered at 1 year. It asks questions about PAD treatment choices, symptom relief options, disease management, and secondary prevention. PAD treatment preferences were also queried, and patients ranked 10 PAD treatment goals (1–10 Likert scale; 10 being most important).
Results:
Among 281 participants completing the survey (44.8% women, mean age 69.6 ± 9.0 years), 54.1% knew that there was more than one way to treat PAD symptoms and 47.1% were offered more than one treatment option. Most (82.4%) acknowledged that they had to manage their PAD for the rest of their life. ‘Avoid loss of toes or legs,’ ‘decreased risk of heart attack/stroke,’ ‘long-lasting treatment benefit,’ ‘living longer,’ ‘improved quality of life,’ and ‘doing what the doctor thinks I should do’ had mean ratings > 9.0 (SD ranging between 1.21 and 2.00). More variability occurred for ‘avoiding surgery.’ ‘cost of treatment,’ ‘timeline of pain relief,’ and ‘return to work’ (SD ranging between 2.76 and 3.58). The single most important treatment goal was ‘improving quality of life’ (31.3%).
Conclusions:
Gaps exist in knowledge for patients with PAD who experience claudication, and there is a need for increased efforts to improve support for shared decision-making frameworks for symptomatic PAD.
Background
Shared decision making is a collaborative model that supports patients’ and clinicians’ engagement in medical treatment decision making so that high-quality decision making can occur to align treatment with patients’ preferences and goals. 1 Shared decision making, and decision-aids that can support this process, are becoming increasingly important to deliver more patient-centered, value-based care.2,3 Shared decision-making approaches are particularly helpful in scenarios where conditions can be managed with different treatment options, each with their own benefits and risks.2,4–6
A condition that lends itself particularly well for shared decision making is peripheral artery disease (PAD). 7 Multiple treatment options exist for PAD symptom relief and improved functional status, including medications, exercise therapy, and invasive procedures. 8 For patients to appreciate all of the available treatment options for their PAD symptom management, and the trade-offs that are associated with each, it is critical that patients have good knowledge and understanding about their disease and its management so that they can prioritize their different PAD treatment goals. Treatment goals in PAD largely evolve around managing cardiovascular risk, symptom relief, and improvement of quality of life. Previously, we have demonstrated that 70% of patients with PAD prefer to take an active role in their PAD treatment decision making, and created a decision-aid for patients with PAD alongside patient and clinician stakeholders.7,9 Whereas poor overall PAD awareness among those at risk or confronted with vascular complications has been shown, 10 it is unknown whether those with a recent PAD diagnosis understand the various PAD treatment goals and options in PAD management as it relates to cardiovascular risk management, PAD symptom relief, and quality of life improvement and how they prioritize their various PAD treatment goals.
Embedded as a substudy in the PORTRAIT registry, 11 which enrolled and followed patients with new or worsening PAD symptoms at initial presentation to a vascular specialty clinic, we studied participants’ knowledge about PAD treatment benefits as it relates to cardiovascular risk management, PAD symptom relief treatment options, and associated outcomes. We also evaluated their preferences and their treatment goals related to PAD management. Understanding these factors can guide efforts to improve the shared decision-making process, as it can elicit the gaps in knowledge related to PAD treatment benefits and risks, and such information can be used to develop targeted educational strategies. In addition, understanding the variability in treatment goals and preferences will allow us to appreciate which goals need more exploration and discussion, versus those goals that are more universally endorsed by patients who have a diagnosis of symptomatic PAD.
Methods
Study design and participants
This was a prespecified cross-sectional substudy of the US participants in the PORTRAIT study, which was a multicenter, prospective, observational registry that enrolled patients with new or worsening symptoms of PAD (Rutherford 1–3, claudication) from 10 PAD specialty clinics, including interventional cardiology, vascular surgery, and vascular medicine clinics. 11 Patients with new or worsening of PAD symptoms presented to these clinics for a PAD work-up and subsequent PAD management. All patients’ PAD status was documented with supporting ankle–brachial index (ABI) information. 11 All patients were treated at the discretion of the vascular specialist, focusing on cardiovascular risk management and symptom management per the established guidelines, 8 as this was a real-world registry. Insights into their understanding of PAD and their treatment goals were collected as part of their 1-year follow-up interview, after having undergone a year of PAD management, with all consecutive patients at the 10 US sites who were eligible for their 1-year follow-up interview from September 14, 2015 through August 15, 2016 receiving the PORTRAIT Knowledge and Preferences Survey. This selection of a limited time frame was chosen to not overburden sites and their patients in adding on questions to their follow-up interviews. Institutional review board approval was received from each participating site, and all patients provided informed consent.
Measures
To assess PAD treatment knowledge, a survey of seven knowledge (‘the PORTRAIT Knowledge and Preferences Survey’ scored as ‘true,’ ‘false,’ and ‘don’t know/unsure’) and four preference questions (‘true,’ ‘false,’ and ‘don’t know/unsure’) was designed based on the current PAD evidence-base, 8 qualitative input from patients, and direct patient and physician expert input as part of the PORTRAIT registry protocol. 11 Knowledge items focused on the availability of PAD treatment choices, PAD symptom relief, chronic disease management, and secondary prevention. Statements on PAD treatment referred to the rapidity of symptom relief, avoidance of invasive strategies, smoking cessation, and exercise therapy. As part of the survey, patients also valued their PAD-related treatment goals by rating 10 PAD treatment goals on a Likert scale from 1 to 10, with 1 being the least and 10 being the most important. Patients were also asked to name their most important PAD treatment goal (see the online supplemental material).
As part of the PORTRAIT registry baseline interview and medical abstraction, information was collected on patient demographics, socioeconomic background, medical history, quality of PAD care, and health status information, as previously described. 11 Baseline information was collected by trained study coordinators at each enrolling site and follow-up interviews were conducted by a centralized follow-up center organized by the call center at the Saint Luke’s Mid America Heart Institute, Kansas City, MO, USA. 11
Statistical analysis
We described patient characteristics for the total sample. Survey results were summarized at the item-level with counts and percentages. The PAD treatment goal ratings were summarized as means, medians, and SDs. The entries for patients’ most important PAD treatment goal were scored and ranked by percent. If a patient mentioned more than one most important PAD treatment goal, a single weight was shared proportionally between each named goal. A comparison was also conducted for patient characteristics between those included in the study versus the remainder of the US PORTRAIT study, 11 and the magnitude of the potential differences was evaluated by calculating the standardized mean differences, with effect sizes 0.20 or smaller denoting negligible differences.12,13 Furthermore, comparisons of patient characteristics, knowledge, and preferences items (Student’s t-tests for continuous variables, and chi-squared tests or nonparametric equivalents where indicated) were performed by whether or not patients received invasive treatment (endovascular or surgical revascularization ⩽ 3 months of PAD work-up) 14 as their primary treatment was performed and standardized mean differences were calculated. Analyses were performed as complete case analysis with R 4.1.0 in the RStudio environment. 15
Results
A total of 281 participants with PAD (claudication symptoms) were surveyed; of whom 44.8% were women and the mean age was 69.6 ± 9.0 years (Table 1). Patients were 72.0% White, 24.7% Black, and 3.2% Native American or Alaska Native. Most (98.2%) were not Hispanic or Latino. The patient cohort had a mean ABI of 0.66 ± 0.18 at baseline. Most patients had documented dyslipidemia and hypertension, over a third experienced a myocardial infarction or had undergone coronary revascularization. Early invasive therapy was administered to a total of 27.8% of the patients, with the majority of them (92.3%) receiving endovascular treatment. A total of 25% were referred to smoking cessation (advice/counseling) and 0.4% received supervised exercise therapy. Missing covariate data ranged from 0.0 to 1.4%.
Baseline patient characteristics of the PORTRAIT Knowledge and Preferences substudy.
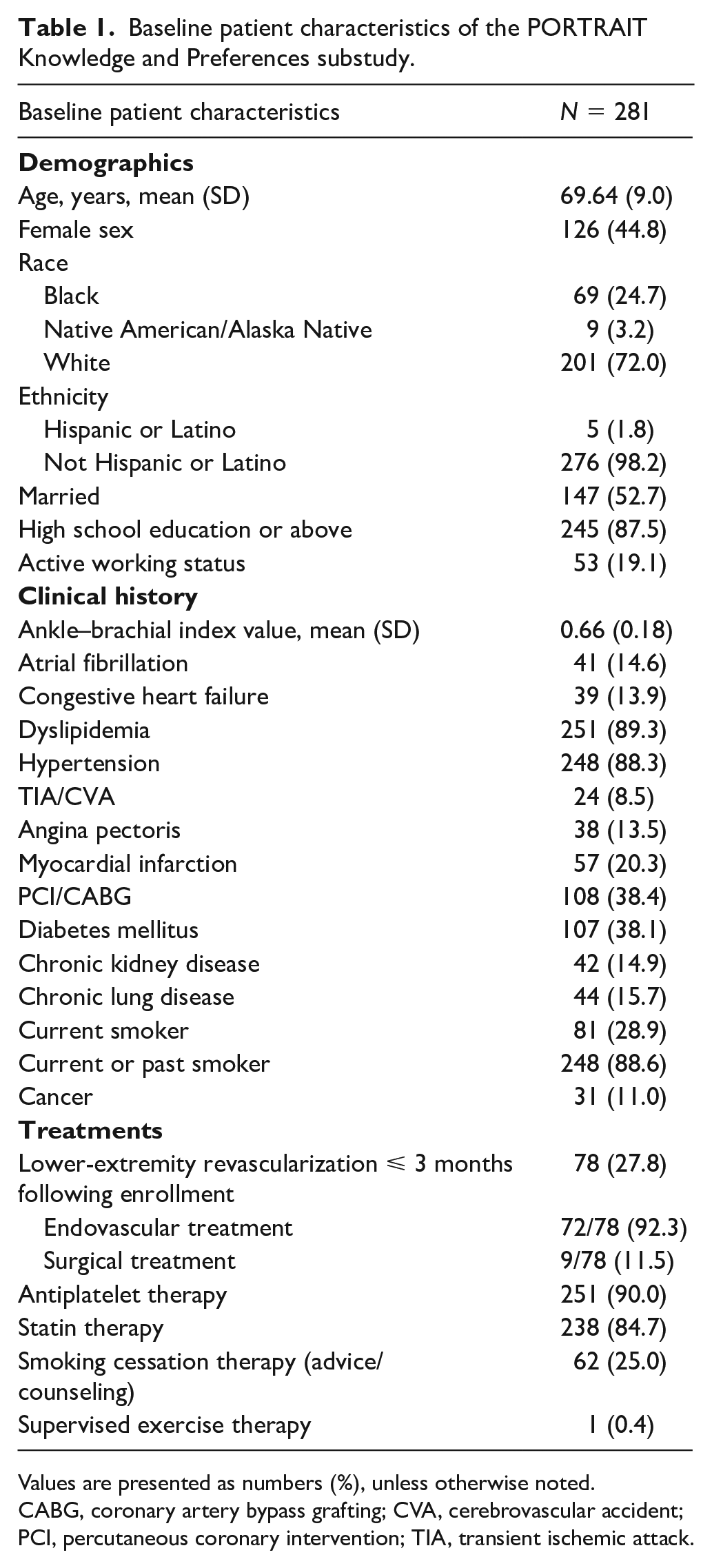
Values are presented as numbers (%), unless otherwise noted.
CABG, coronary artery bypass grafting; CVA, cerebrovascular accident; PCI, percutaneous coronary intervention; TIA, transient ischemic attack.
Regarding treatments for symptom relief, only 54.1% knew that there was more than one way to treat their PAD symptoms, and less than half (47.1%) were offered more than one treatment option (Figure 1 and online supplemental Table 1). Among those who smoked, 24.3% knew that quitting smoking may improve their symptoms. Finally, a little over a third of patients (37.3%) thought that medications alone could be used to manage their PAD symptoms (Figure 1 and online supplemental Table 1).
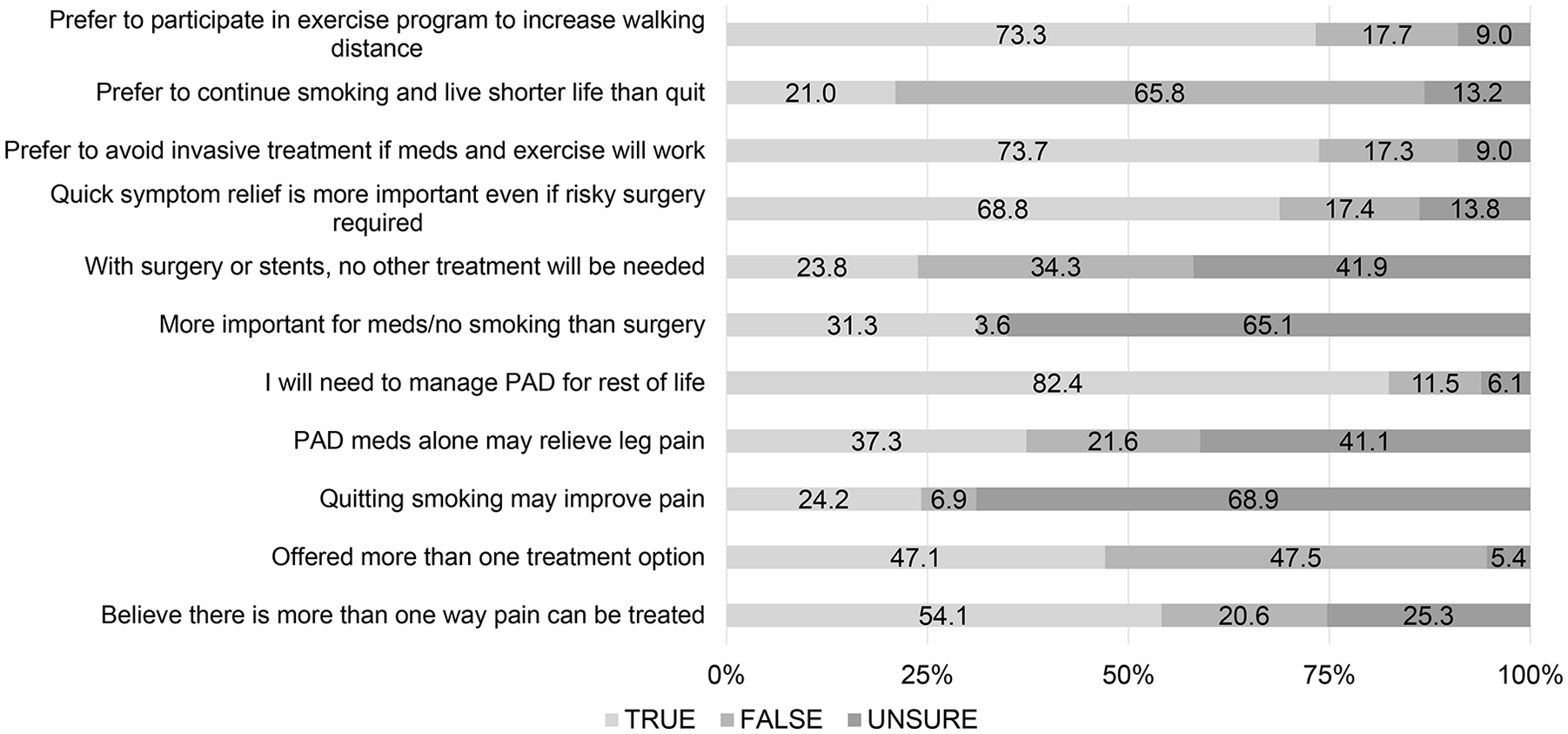
Overview of responses to PORTRAIT Knowledge and Preferences Survey items (%).
With regards to the chronic nature of PAD, most (82.4%) acknowledged that they had to manage their PAD for the rest of their life, but only a third (31.3%) agreed it is more important to take medications and stop smoking than to undergo invasive treatment for their legs to prevent heart attacks, amputations, stroke, and death. Almost a quarter (23.8%) thought that with leg surgery or stents, no other treatments were needed to manage their PAD (Figure 1 and online supplemental Table 1). When comparing patient characteristics between those included in the knowledge and preferences substudy, against the remainder of the US PORTRAIT population, no meaningful differences were noted (all standardized mean differences of 0.20 or smaller) (online supplemental Table 2).
As for PAD treatment preferences, the majority (68.8%) preferred quick symptom relief, even if requiring invasive treatments with possible risks (online supplemental Table 1). However, the majority (73.6%) also indicated that they want to avoid invasive treatments, if medications and exercise could relieve their symptoms. Among smokers, 22.1% preferred to continue smoking, even if this meant a shorter life. A total of 73.3% was also prepared to engage in exercise therapy, in addition to their usual PAD care (Figure 1 and online supplemental Table 1).
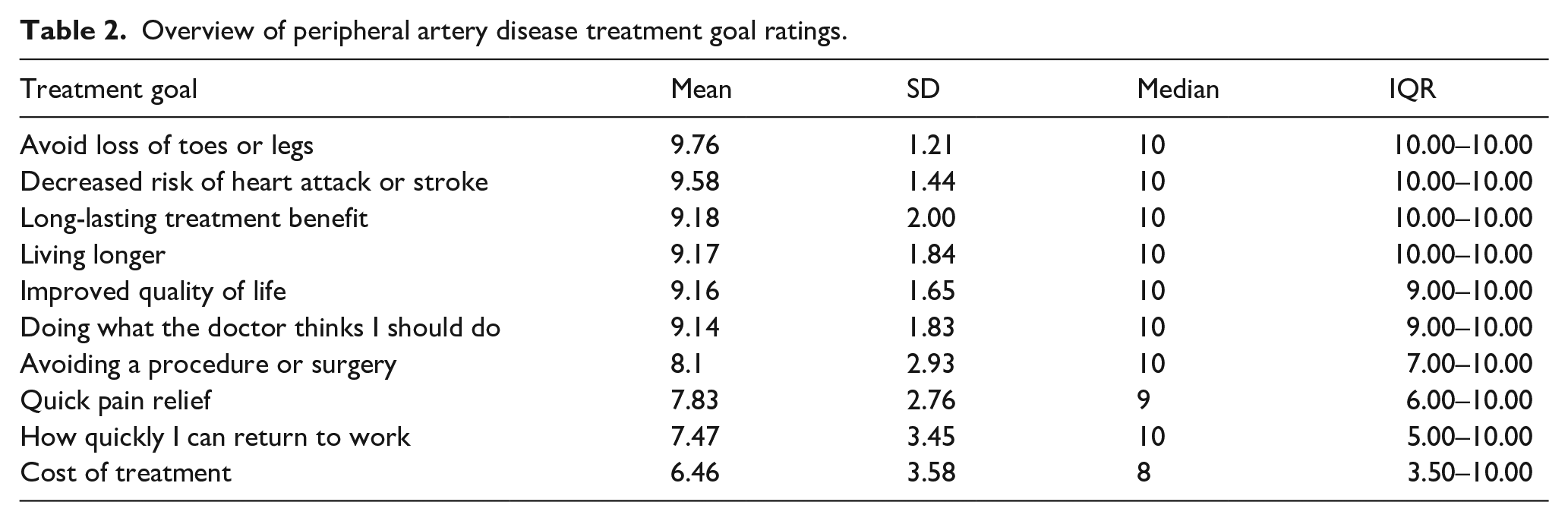
Several treatment goals were identified, including ‘avoid loss of toes or legs,’ ‘decreased risk of heart attack or stroke,’ ‘long-lasting treatment benefit,’ ‘living longer,’ ‘improved quality of life,’ and ‘doing what the doctor thinks I should do,’ which each had mean scores > 9, with little variability across respondents as demonstrated by their IQR and SDs (Table 2 and online supplemental Table 1). Treatment goals with lower perceived value and wider variability included ‘avoiding a procedure or surgery,’ ‘quick pain relief,’ ‘how quickly I can return to work,’ and ‘cost of treatment,’ indicating more disparate ratings across respondents (SDs ranging from 2.76 to 3.58; Table 2 and online supplemental Table 1).
Overview of peripheral artery disease treatment goal ratings.
When asking patients to choose the five most important PAD treatment goals, the top goal was improving quality of life (31.3%), followed by living longer (20.5%), avoiding loss of toes or legs (10.7%), and decreased risk of heart attack or stroke (4.3%) (Figure 2 and online supplemental Table 1). Treatment goals identified beyond those specified included ‘being present for family’ or ‘no concern’ for treatment goals.
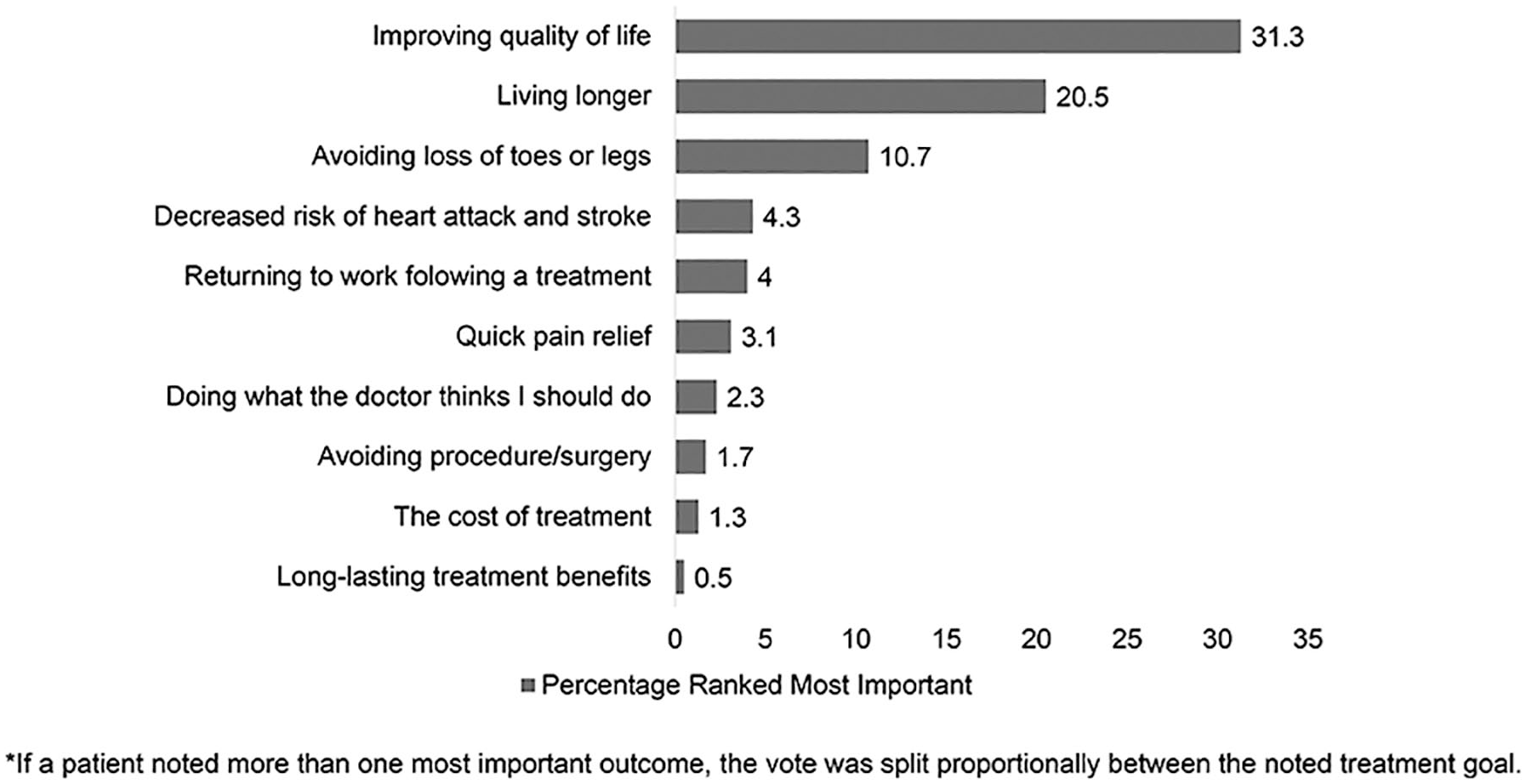
Percentage of most frequently named important peripheral artery disease treatment goals.
A small proportion received invasive treatment (endovascular or surgical revascularization) as their primary treatment strategy (19%, n = 54) (Table 1). Those who received early invasive treatment were more likely to be women and White, and less likely to have a history of stroke or transient ischemic attack. Those who underwent invasive treatment compared with those who did not were more likely to believe that there was more than one way to treat their pain, that medications alone may relieve leg pain, and that with surgery or stents no other treatment will be needed to manage their PAD; they also valued quick symptom relief versus upfront risk more often, were less likely to avoid invasive treatment (vs medications or exercise), and had higher importance scores for the following outcomes: avoiding loss of toes or legs, long-lasting treatment benefit, and quick return to work (online supplemental Tables 3a and 3b).
Discussion
As a foundation for improving shared decision making in patients with PAD experiencing claudication symptoms, it is important to assess patients’ current understanding in routine clinical practice, their exposure to shared decision making, and their treatment priorities. In our study, we identified substantial gaps in PAD knowledge among patients who were diagnosed and treated at vascular specialty clinics for their PAD. Although most people understood that PAD is a chronic disease that needs to be managed for the rest of their lives, only half did not know there are multiple options to manage their PAD symptoms, and less than half were offered multiple options. The role of cardiovascular risk management versus the effects of invasive treatment for managing PAD was not clear to patients, as one in five thought that with invasive treatment no other PAD treatment was needed. As for PAD treatment goals, improving their quality of life was most important, followed by avoiding amputations, death, stroke, and heart attacks. Collectively, these findings underscore the opportunity to further educate patients about PAD and its treatment, and emphasize the need to better clarify their treatment goals so that optimal treatments can be offered and discussed.
This study extends the current understanding of patients’ PAD knowledge and preferences. Previously, a general awareness survey around PAD documented gaps in PAD awareness among the public and providers, and, more recently, an overall lack of PAD disease identification was noted among patients with vascular complications.10,16 Our study expands this prior work by showing that even among those having undergone a year of treatment for their PAD that opportunities exist for additional education and better clarification around the goals and roles of different therapeutic approaches. Our work complements prior work on preferences for interventions and trade-offs for amputation risk, as well as overall work exploring shared decision-making preferences in vascular diseases, and the overall unawareness for the condition of PAD.17–20 Understanding which goals are almost universal to patients navigating PAD versus those that are more susceptible to individual variability can be helpful in creating shared decision-making tools to further improve the patient-centeredness of care. Though shared decision aids for PAD are emerging, they will likely require further adaptation, efficacy testing, and dissemination as new insights emerge as to how to offer educational materials and preference elicitation in a more patient-centered way. 7 In the same fashion, supporting shared decision efforts for more advanced lower-extremity PAD, i.e., critical limb ischemia, will require dedicated comparative effectiveness evidence-base building, such as staged work with patient and provider stakeholders,21,22 to elicit the trade-offs of treatment approaches. These efforts may be spurred by emerging comparative effectiveness research comparing surgical with endovascular approaches for critical limb ischemia.23,24
Specifically regarding the preferences elicitation as it relates to the entire spectrum of PAD treatment goals, the following patterns of valuation emerged. We observed that almost all patients with symptomatic PAD involving claudication symptoms universally valued avoiding clinical events including amputation of toes and legs, death, stroke, or a heart attack, and improving their quality of life, which reinforce the need to value these endpoints in creating decision aids and as outcomes in emerging PAD trials. When asked to choose a top priority for their PAD treatment outcomes, almost one-third chose improving quality of life as their most important goal, over avoiding clinical events, underscoring the utmost importance for this endpoint both in prioritizing clinical trial endpoints, as well as in prioritizing PAD treatment goals. More variability was observed for treatment goals related to work return, avoiding cost, quick pain relief, and avoiding surgery. Especially among those who had received invasive treatment compared with those who did not as their primary PAD symptom management strategy, the goals of quick pain relief and return to work were more valued. This emphasizes the importance of initiating a dialogue with patients who have PAD and are experiencing claudication about their individual preferences and characteristics, such as age, socioeconomic status, and past medical history, as these factors can significantly influence their values and priorities. Only 20% of patients believe additional treatment is necessary after invasive treatment. Lifestyle-limiting claudication should be considered when evaluating treatment options. Patients who smoke and opt for revascularization procedures should be informed of the increased risk of reduced patency and amputation, and offered support for smoking cessation. Less than half of the patients were presented with multiple options to manage their PAD symptoms, likely due to the lack of shared decision-making tools in claudication. Treatment variability may depend on the setting, but medical management should be prioritized, and patient education and shared decision making promoted for informed treatment choices. Finally, patients with symptomatic PAD involving claudication valued the doctor’s treatment recommendation greatly, which does not necessarily have to contradict the fact that patients want to play an active role in the decision-making process, as previously over 70% of patients with PAD indicated they wanted an active, shared role. 9
Study limitations
Our study should be interpreted in the context of the following potential limitations. Owing to the particular sites that participated in the study, generalizability of the findings to other settings needs to be further established. The study participants had symptomatic PAD with claudication, and their perspectives may not be generalizable to patients with more severe forms of PAD like critical limb ischemia. It is also likely that the estimates of patients’ knowledge are greater in this context than in nonspecialty clinics, given the focus of these clinics on patients’ PAD. Furthermore, patients with PAD and claudication were surveyed 1 year following their PAD diagnosis and treatment, which may have made them more informed about the PAD management options, as opposed to patients who are early into the diagnostic process. Future studies will need to evaluate both knowledge and preferences at the time of evaluation and then follow-up to understand how they may evolve over time. As a follow-up to our work, variations by demographic profiles will need to further be explored as preferences may differ as a function of patients’ background. In addition, although patients prioritized improvement in quality of life as an important treatment goal, it is unclear which aspects of their quality of life they valued the most. Lastly, preferences may also change over time, and longitudinal data on PAD treatment preferences are needed as they continue to manage their chronic disease.
Conclusion
In conclusion, we identified substantial, addressable knowledge gaps in patients with symptomatic PAD involving claudication who were treated in vascular specialty clinics. Moreover, we identified key PAD treatment preferences that can further inform shared decision-making frameworks for patients with symptomatic PAD. In an era of value-based PAD care, addressing PAD-related health literacy and tailoring patient preferences to evidence-based PAD treatment options will be key to increase the quality of decision making, work as active partners, for both patients and the PAD care team, and to optimize subsequent outcomes.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231181613 – Supplemental material for Patient knowledge and preferences for peripheral artery disease treatment
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231181613 for Patient knowledge and preferences for peripheral artery disease treatment by Kim G Smolderen, Gaëlle Romain, Kensey Gosch, Ahmad Arham, Jeremy B Provance, John A Spertus, Anwesh B Poosala, Mehdi H. Shishehbor, David Safley, Kate Scott, Nancy Stone and Carlos Mena-Hurtado in Vascular Medicine
Footnotes
Acknowledgements
The PORTRAIT (Patient-Centered Outcomes Related to Treatment Practices in Peripheral Arterial Disease: Investigating Trajectories) research consortium honors the memory and contributions of Mark L Friedell, MD. We acknowledge the patient (Shirley Leg; Robert Liedler; Mark Bryant) and physician (Herbert Aronow, MD; Thomas T Tsai, MD; Alan T Hirsch, MD, deceased) expert members, and our observational monitoring board members (William Hiatt, MD, deceased; Mark Creager, MD; Greg Moneta, MD; Mark L Friedell, MD) who have advised us throughout the planning, design, and implementation of the study
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kim Smolderen receives research grants from J&J, Philips, and Abbott and is a consultant for Optum Labs, Cook, Tegus, Happify, and Abbott; John Spertus reports consulting relationship with Merck, Janssen, Novartis, Myokardia, Bayer, and United Healthcare, grant funding from Abbott Vascular, ownership of the copyright to the SAQ, KCCQ, and PAQ, and service on the Board of Directors of Blue Cross Blue Shield of Kansas City; Carlos Mena-Hurtado reports consulting for Abbott, Optum Labs, Penumbra, and Cook; all other authors report no other disclosures. Drs. Smolderen and Mena-Hurtado are supported by NIH grants 1R21AT012430-01 and 1R01HL163640-01A1.
Funding
Research reported in this article was partially funded through two Patient-Centered Outcomes Research Institute (PCORI) Awards (IP2 PI000753-01; CE-1304–6677), The Netherlands Organization for Scientific Research (VENI Grant No. 916.11.179), and an unrestricted grant from W. L. Gore & Associates, Inc. (Flagstaff, AZ, USA). Drs. Smolderen and Mena-Hurtado receive additional support from the National Institutes of Health (grants 1R21AT012430-01 and 1R01HL163640-01A1). The funding organizations and sponsors of the study had no role in the design, conduct, analysis, and interpretation and reporting of the study. The statements in this article are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or Methodology Committee. All manuscripts for the PORTRAIT study are prepared by independent authors who are not governed by the funding sponsors and are reviewed by an academic publications committee before submission.
Data availability
The data for this study are available from the corresponding author upon reasonable request.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.