
Abstract
This systematic review evaluated the knowledge and awareness of peripheral artery disease (PAD) within the general public (including patients with peripheral vascular disease), nonspecialist healthcare professionals (nsHCP), and trainees (medical students and trainee doctors). Relevant articles were identified from electronic databases using key search terms: ‘peripheral artery disease’; ‘limb ischaemia’; ‘intermittent claudication’; ‘knowledge’; ‘understanding’; ‘public’; ‘medical professional’. The heterogeneous results were described narratively. A lack of knowledge and understanding of PAD (disease awareness) were identified in all groups. Among nsHCPs, factors which affect knowledge include the level of training, early clinical exposure and the presence of family members with cardiovascular/vascular disease. Within the general public, knowledge and awareness was improved if a family member/friend had a diagnosis, or following a patient-centred consultation with any HCP. Public campaigns are proven effective in improving disease knowledge/awareness in conditions such as stroke alongside sustained patient education. These may provide future avenues to improve PAD knowledge and awareness, in order to effectively manage risk factors and minimise delayed or missed diagnosis of PAD. (
Keywords
Introduction
Peripheral artery disease (PAD) describes the impairment of blood flow to the peripheries due to atherosclerotic disease. Although the total number of deaths due to circulatory disease has decreased, they represented 31% of all global deaths in 2016. 1 PAD is estimated to be present in a fifth of those aged over 60 and carries an increased risk of cardiovascular disease and stroke. 2 In the majority of patients, PAD is asymptomatic. However, when symptoms do arise, they can cause functional impairment and decreased quality of life. 3 A community doctor working in general practice with an average patient list of 3500 patients would expect to manage approximately 100 patients with PAD. 4
PAD has long been underdiagnosed and it is estimated that up to half of all people with PAD are undetected.5,6 In order to make a timely diagnosis, a patient must identify they have a medical issue and present themselves to healthcare services. Alternatively, any healthcare professional should appreciate patient risk factors and undertake opportunistic screening. 4 Considering a possible diagnosis, followed by a carefully taken patient history and appropriate examination, including an ankle–brachial pressure index (ABI), are all important in the recognition of PAD.2,7
Several reasons have been postulated for the lack of detection, of which the most common are the high prevalence of asymptomatic disease and the inappropriate use of screening and diagnostic tools.3,8 Individual studies have recognised poor awareness of PAD within individual populations. However, these findings have not been correlated and compared across multiple study populations. In order to develop interventions to improve knowledge, greater understanding of the determinants of PAD knowledge by nonspecialist healthcare professionals (nsHCPs) is required. These comprise multiple disciplinary professionals including general practitioners, nurses, and podiatrists, who are often the first contact patients have with healthcare services. Equally, it is also important to determine the current level of patient/public knowledge to evaluate whether the current provision provides adequate education and opportunity to assess the risk of disease. Ultimately, improved knowledge aims to improve health quality outcomes.
The aims of this review are: (1) to identify the current level of knowledge regarding PAD in patients/public; (2) to identify the current level of knowledge regarding PAD in nsHCPs and trainees; and (3) to evaluate factors determining knowledge levels.
Methods
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed to identify articles where the main focus of the study was knowledge of PAD. 9 A search of electronic databases (MEDLINE, Embase, The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Methodology Register, CINAHL, Scopus, and grey literature) of all available articles was conducted by CP and BB (December 2018), using combinations of the following keywords and thesaurus headings: ‘peripheral artery disease’; ‘limb ischaemia’; ‘intermittent claudication’; ‘knowledge’; ‘understanding’; ‘public’; ‘medical professional’. Bibliographic lists were scanned for additional relevant articles. The search was repeated on April 30, 2019.
A study protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42018117304).
Eligibility criteria
All quantitative and qualitative studies relating to this topic were included if they presented cognitive PAD knowledge. Articles which related solely to relevant performing of practical skills (e.g. ABI) were excluded. For breadth, conference abstracts were also included. Only English language articles were considered.
Types of participants
This study investigated knowledge of PAD in three adult groups (aged 18 years or older):
The general public, including individuals with a presumed or confirmed diagnosis of PAD.
Practising healthcare professionals not specialised in managing PAD or its complications: nsHCPs. The nsHCPs included general practitioners, nurses, and podiatrists.
Training healthcare professionals, including medical or nursing students.
Definition of PAD
For the purposes of this review, where appropriate, an ABI ratio of less than 0.9, a confirmed diagnosis of PAD within patient records, or history of a previous revascularisation procedure were used to indicate the presence of PAD.2,10
Data extraction
Search results were imported into EndNote™ X9 (Clarivate Analytics®) and duplicates removed. Titles and abstracts were reviewed independently for potential suitability against the inclusion criteria by investigators BB and AN. The full texts of suitable studies were retrieved and independently assessed for final inclusion by BB, AN, and JH. A standardised data extraction form was created and tabulated into Excel™ 2016 (Microsoft®). Data extraction was performed independently by BB, AN, and JH Cases of disagreement were resolved by discussion within the team.
Study quality
The quality of these studies was assessed using the complement of critical appraisal tools provided by the Joanna Briggs Institute.11–13 This considered the evidence in each study with relation to our research questions throughout a series of domains. We graded the study quality as high (all domains satisfied), moderate (one domain unsatisfied or unknown) or low (more than one domain unsatisfied). Currently, no tool exists for assessment of conference abstracts.
Evaluation of quality was performed independently by BB and AN, or JH after data extraction and disagreement was resolved through discussion. All studies were included, irrespective of their quality.
Strategy for data synthesis
A narrative synthesis of results structured around the knowledge and awareness of PAD, and determining factors for knowledge within the three groups, was performed and the data were tabulated where appropriate. Given the anticipated heterogeneity of results, a meta-analysis was not undertaken.
Results
A total of 27 articles were identified as meeting the eligibility criteria (Figure 1). Table 1 summarises the characteristics of the studies. Table 2 gives an overview of the included participants. The quality of the studies focused on nsHCP were deemed as high = 1, moderate = 6, and low = 2. For those focused on public/patients, study quality was deemed as high = 7, moderate = 4, and low = 7 (online supplementary information).
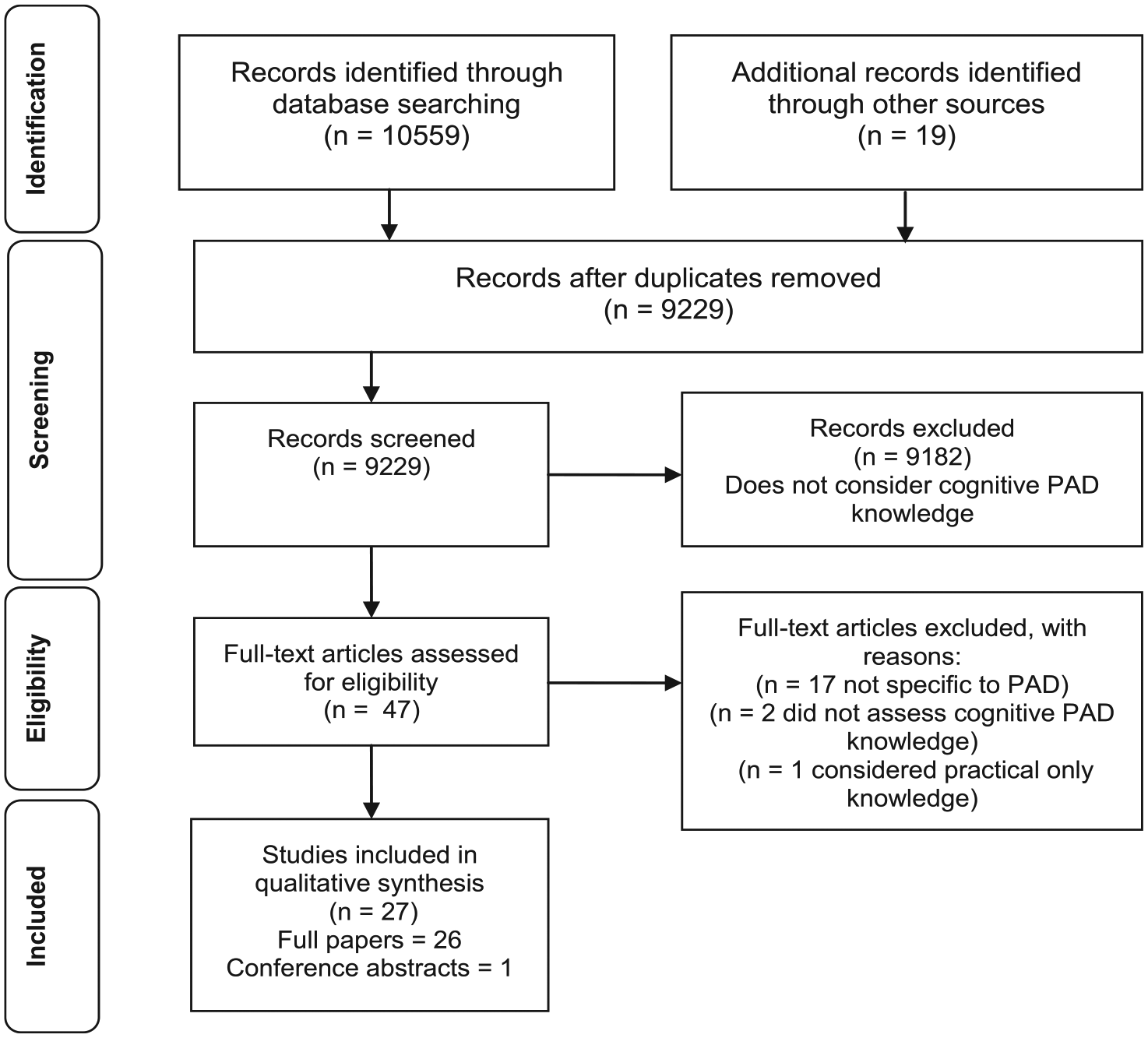
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of information through the different phases of the systematic review.
Overview of the characteristics of the studies.
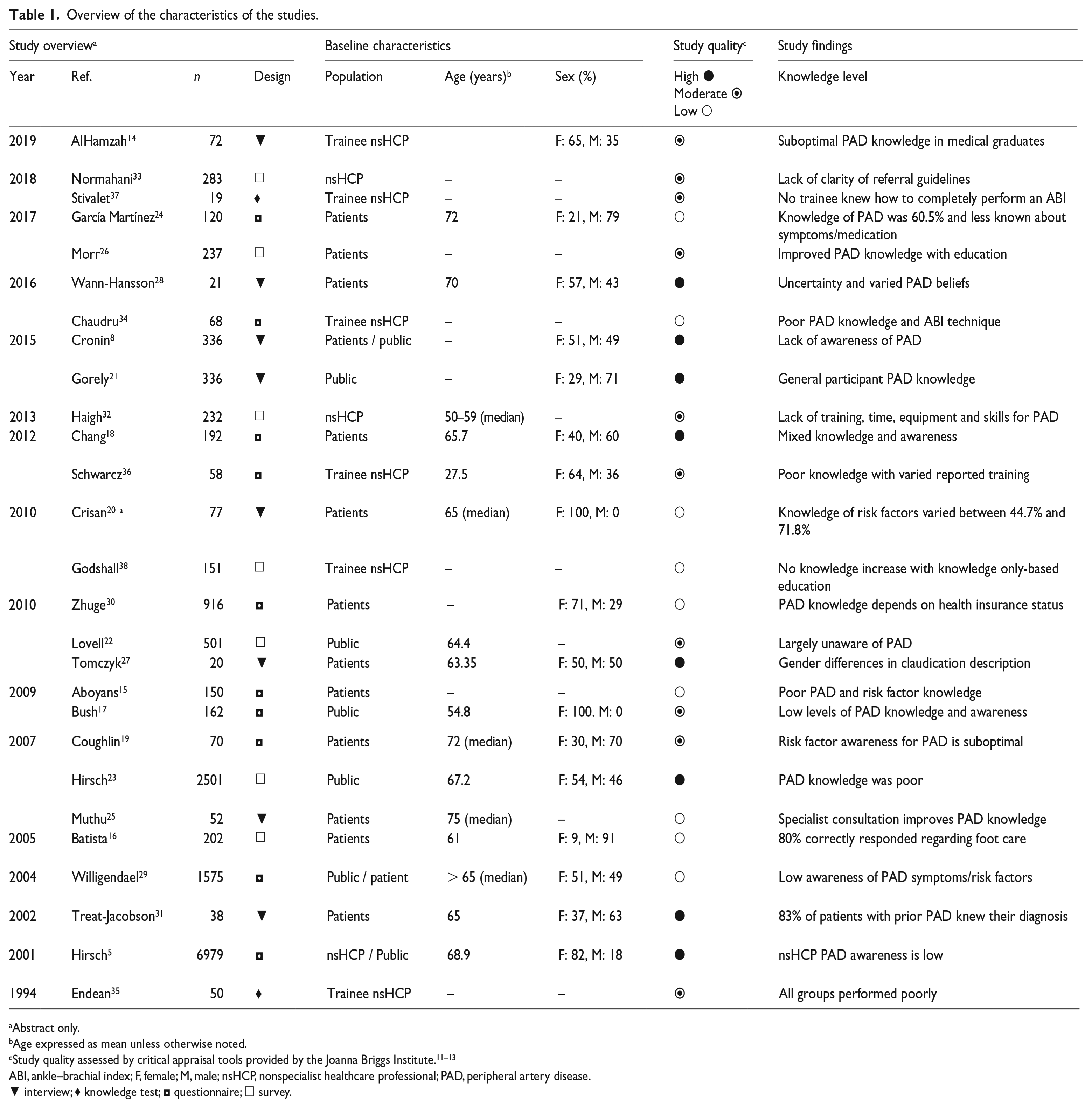
Abstract only.
Age expressed as mean unless otherwise noted.
ABI, ankle–brachial index; F, female; M, male; nsHCP, nonspecialist healthcare professional; PAD, peripheral artery disease.
▼ interview; ♦ knowledge test; ◘ questionnaire; □ survey.
Characteristics of the study participants.
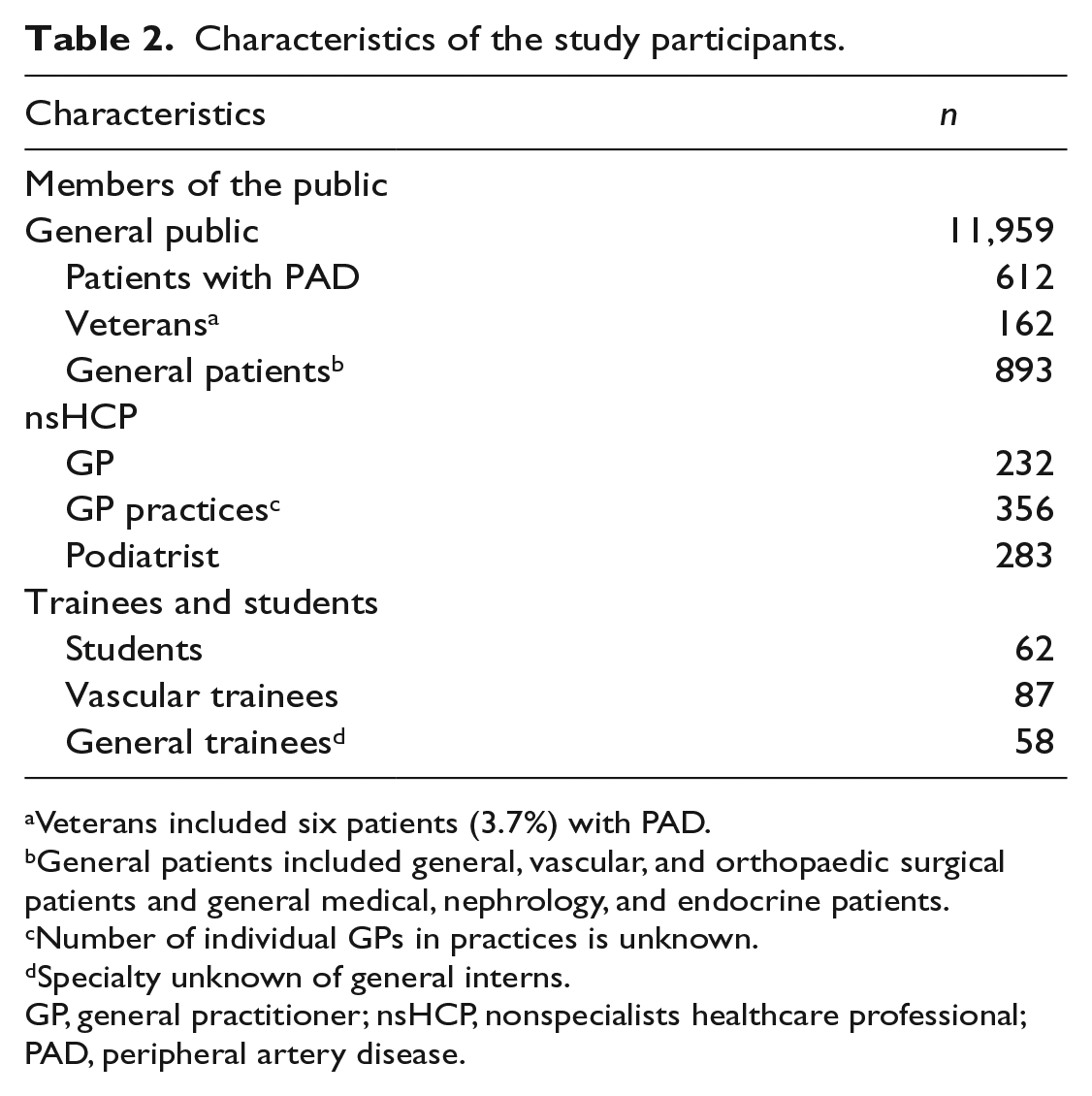
Veterans included six patients (3.7%) with PAD.
General patients included general, vascular, and orthopaedic surgical patients and general medical, nephrology, and endocrine patients.
Number of individual GPs in practices is unknown.
Specialty unknown of general interns.
GP, general practitioner; nsHCP, nonspecialists healthcare professional; PAD, peripheral artery disease.
Knowledge of PAD – patients/public
Nineteen studies explored PAD knowledge within patients/public,5,8,15–31 of which six studies focused on risk factor awareness.8,15,18,20,23,25
Understanding PAD
Awareness of PAD ranged across the studies from 21% 25 to 60.5%. 24 When asked to classify its severity, PAD was considered an innocent condition by 25%, relatively serious by 61%, and very serious by 5%. PAD symptoms were described as a ‘pain in the legs that subsides during rest’ and ‘pain during walking’. Willigendael found that participants had ‘heard of’ PAD (50%) but were less familiar with the term intermittent claudication (5%). 29 Gorely and Tomczyk provided terms used by patients which give insight into their understanding of PAD. Descriptions included ‘a blockage with plaque or fat’; ‘hardening of the arteries, where blood just doesn’t flow properly’, and ‘it’s kind of a blockage of the artery’.21,27 Colloquial terms such as ‘window-shopping legs’, more commonly recognised by the Dutch, are also used, which may add to confusion. 29
Wann-Hansson reported patients/public generally felt they had insufficient knowledge of both cardiovascular and peripheral vascular disease. 28 Even when participants thought that they had good awareness of PAD, they had low overall knowledge of the clinical features of the condition. 26 There was confusion with other diagnoses such as chronic venous diseases and musculoskeletal injuries.14,15,27,29 Wann-Hansson reported that participants assumed that symptoms would dissipate with time or identified them with ‘expected’ pain with older age.28,31
Muthu reported improved knowledge following a consultation with a specialist healthcare professional; although 4% remained unaware of their vascular diagnosis. 25 Chang reported 90% of patients treated at a vascular clinic knew their diagnosis, where 88% of these identified the correct diagnosis and 78% were aware of the importance of secondary prevention. 18 In the same study, 68% of participants reported they had never discussed PAD or risk reduction. When a relative or friend had PAD, 10% more participants were able to describe universally recognised PAD symptoms. 29 Hirsch noted participants gained knowledge regarding PAD mostly from nonmedical sources including from family and friends, the internet, and books. 5
Risk factors
Knowledge regarding PAD risk factors varied among the studies (Table 3). There was a general lack of knowledge regarding causes of PAD, despite the presence of multiple risk factors.14,17,22 Although specialist assessment improved awareness of some risk factors, such as smoking (73% vs 90%, p = 0.028) and diabetes (23% vs 66%, p = 0.028), Muthu did not report an increased awareness of any other PAD-associated risk factor. 25 Hirsch highlighted that reduced risk factor recognition was associated with older age, lower educational level, and income, 5 something which was corroborated by Coughlin. 19 Some ex-smokers continually denied a correlation between smoking and PAD, or needed confirmation and encouragement to continue their nonsmoking status.28,31
Risk factors for PAD identified by members of the public and patients segregated into those correctly reported, unrecognised, and incorrectly reported.
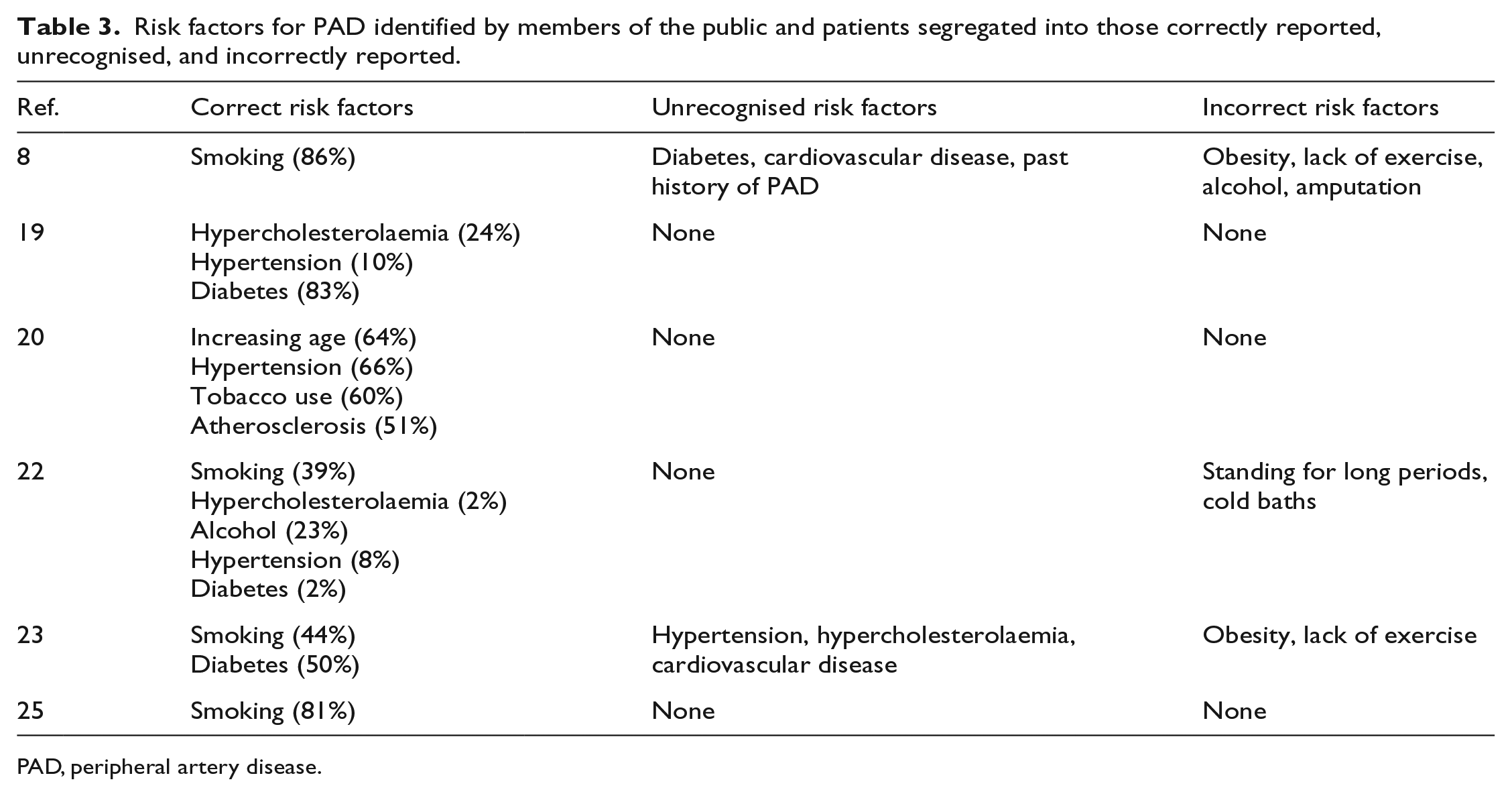
PAD, peripheral artery disease.
Knowledge of PAD consequences
Two studies investigated the awareness of the associations between PAD and other medical conditions, with results varying hugely. Between 28% 23 and 94% 8 of respondents recognised an association with stroke disease; 25% recognised an association with myocardial infarction 5 , and 78% with coronary heart disease. 8 The highest level of recognition was seen with diabetes, at 98%. 8 Awareness of the association between PAD and amputation varied between 14% 5 and 60% 8 and only 14% associated PAD with an increased risk of death. 5 Cronin did not find any increased awareness of PAD in those patients who had previously suffered any of the above conditions. 8
Knowledge of PAD management
Although participants had a general awareness of self-management, which included smoking cessation, weight loss, and regular exercise, these were often without substance or active implementation plans. 23 Uncertainty and lack of motivation was repeatedly noted by participants as a barrier for implementation of self-management, particularly activity-induced pain. One participant in this study stated: ‘exercise causes pain which you’re trying to get rid of’. However, knowledge was increased and retained when individuals received tailored management on a regular basis.5,16 For example, Hirsch reported a 14% improvement in management knowledge between a first and second visit, with further knowledge improvement during subsequent visits. 5
Knowledge of PAD – Nonspecialist Healthcare Professionals
Knowledge of nsHCPs was evaluated within three studies. Knowledge of PAD was classified into disease awareness, adherence to evidence-based guidance, and risk factor recognition.5,32,33
Screening a population of patients with PAD, Hirsch reported that only 49% of patients screening positive for the condition had been diagnosed by their usual primary care doctor. 5 Haigh’s survey reported just 6% of GP respondents were aware of PAD guidance, where 61% of these GPs screened patients for PAD. These GPs were prompted to screen by the presence of risk factors such as smoking and type II diabetes. 32 Screening mainly took the form of history and examination, followed less often by ABI (54%) or duplex ultrasound scanning (42%). 32 Barriers to screening included lack of knowledge, equipment, training, and skills. 32
Normahani surveyed UK podiatrists and found a correlation between level of vascular education, clinical-training, and confidence in recognising vascular foot problems and appropriate referrals. 33 Awareness and recognition was generally improved if nsHCPs had increased clinical exposure to PAD, received training to perform ABI, and if patients displayed classic symptoms such as leg claudication. 5
Knowledge of PAD – trainees and students
PAD knowledge by medical students and trainee doctors was tested using questionnaires and during formal examinations within six studies.14,34–38 Overall knowledge was rated at modest to poor for data gathering and its interpretation during practical exams. It was improved if there was a personal or family history of cardiac disease. Although Chaudru reported 21% of students were familiar with ABI guidance, only 11% were able to perform an ABI. 34
Godshall introduced an educational programme for second year medical students, containing didactic lectures and a problem-based learning session. Here, knowledge scores were comparable with third year medical students unexposed to this module. 38 This suggests an increased level of training and early clinical exposure to vascular disease training may be as valuable as teaching to improve knowledge.
An overview of the recommendations to improve PAD knowledge in all groups is presented in Figure 2.
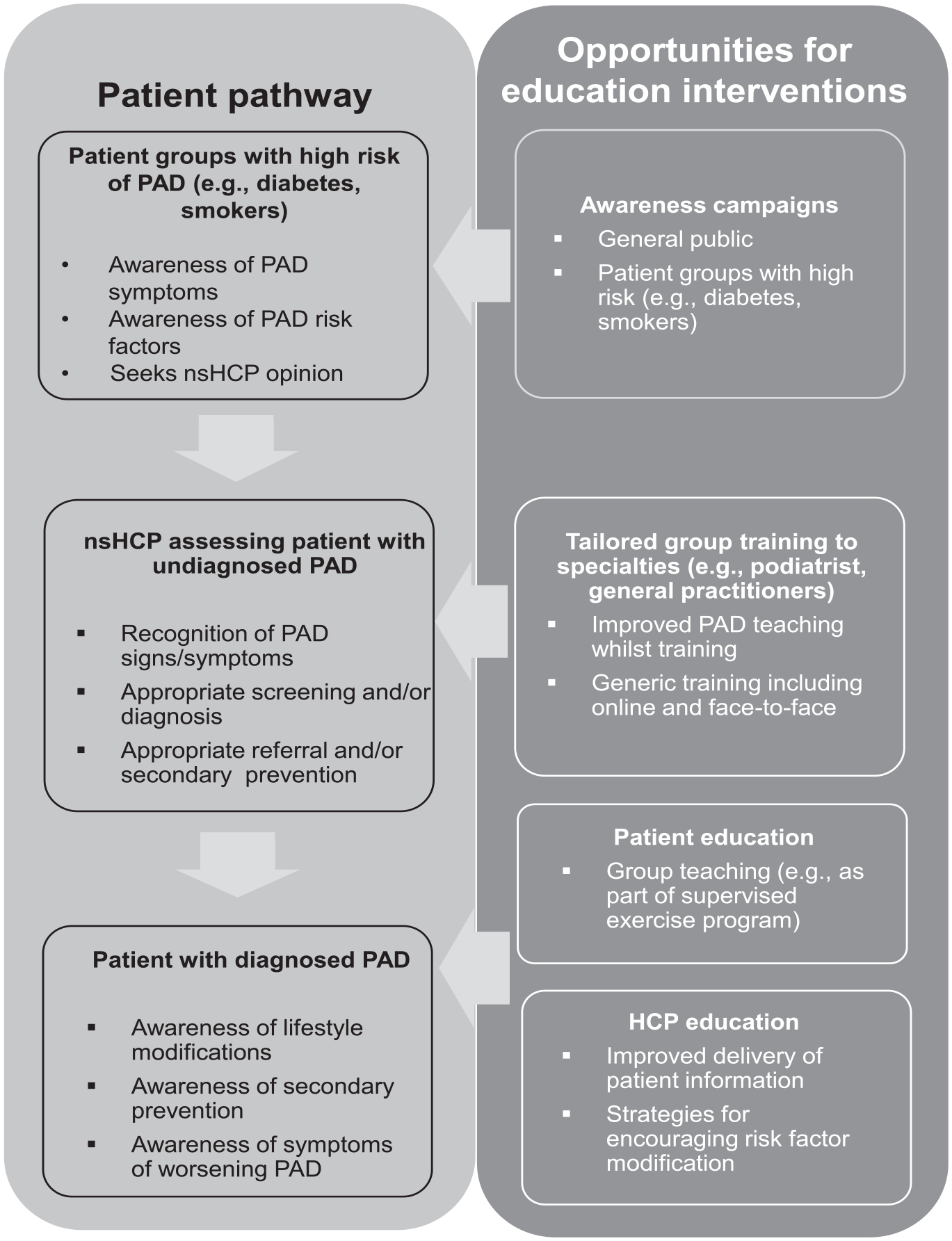
Overview of the recommendations to improve PAD knowledge within healthcare professionals and patients/public.
Discussion
This systematic review examined 27 articles which focused on PAD knowledge in order to evaluate the level and determinants of PAD knowledge in patients/public, nsHCPs, and respective trainees. Knowledge of PAD, its risk factors, consequences, and management varied across the studies, with clearly recognised knowledge inadequacy alongside uncertainty of its potential seriousness. These findings are consistent across the studies despite the varying levels of the quality of the studies.
Delays in the presentation and appropriate management of PAD may lead to complications such as ischaemia, amputation, and death. 39 To initiate timely treatment, patients must first recognise their symptoms and seek medical attention. Following this, nsHCPs need to suspect the potential for PAD to refer, investigate or initiate secondary prevention. It is therefore important to identify the knowledge of nsHCPs, who are often the first line in consulting patients, in order to offer insight into the problem of PAD underrecognition and delays in presentation from both sides of the consulting room. Several determinants of knowledge have been identified for nsHCPs and patients/public which give opportunities to focus efforts to improve PAD knowledge, recognition, and subsequent management.
Patients/public and PAD
There appear to be misconceptions in the differences between PAD and other common conditions, such as musculoskeletal disorders, and what should be considered normal within the aging process. This is compounded by poor understanding of the basic pathophysiology of PAD by patients/public, which may reduce the ability to correlate risk factors. PAD is often referred to using numerous terms by patients/public and nsHCPs, which may add further uncertainty.
Public understanding of PAD and personal risk was often translated through the knowledge and experience of friends/relatives, social media, and public opinion and campaigns. 34 The Act Fast campaign in the United Kingdom pursued TV adverts with national media coverage in order to improve stroke knowledge and recognition. Dombrowski identified the campaign results in high levels of stroke awareness among the public. 40 Flynn also noted increased information-seeking behaviour with increased presentation to medical services. 41 The National Heart, Lung, and Blood Institute (NHLBI) within the USA has co-implemented a national PAD awareness campaign for the public and for healthcare providers, which offers education events and resources to improve PAD knowledge. Here, there are opportunities to re-invigorate and utilise increasingly popular methods of patient education, particularly online and via social media.42,43 In the UK, the Putting Feet First campaign led by Diabetes UK provides a further opportunity to raise awareness of PAD. 44
For individual patients, knowledge was improved when they received individually tailored management. When practitioners have an understanding of their patient’s knowledge of PAD, this provides an opportunity for a patient-centred consultation using terminology a patient can clearly understand. Despite this, Hirsch identified that only a small number of individuals received PAD information from a nonspecialist or specialist practitioner. 23 A meta-analysis of educational and behavioural interventions to improve stroke risk factors did not show any effect on several risk parameters within stroke management, although some improvements were observed when these were delivered by multidisciplinary team (MDTs). 45
Diabetes literature provides examples of effective patient therapeutic education, particularly when performed by a MDT, facilitating the opportunity for several specialties to be involved in patient care – and multiple opportunities for patient education.45–47 These may reflect the ability to spend time with a patient and provide effective communication. Heiler found that this positively correlated with greater self-management regardless of confounders including sociodemographic and health variables. 48 However, evidence suggests that tailored education should be sustained and intensive from specialist and nonspecialist MDTs members to ensure ongoing patient engagement.49,50
Healthcare professionals
All health professionals – specialist and nonspecialist – should be aware that a large proportion of patients with PAD are asymptomatic and patients may progress to a point of irreversible damage, including higher mortality rates, before diagnosis. 51
For frontline and community-based nsHCPs, which include doctors, nurses, and podiatrists, demands for the recognition of disease within a single consultation are often complicated by multimorbidity, quality outcomes assessment, and patient demands. This may lead to missed opportunities for disease recognition and diagnosis. This has been seen within cancer diagnosis whereby a patient presents with complex symptomology, which can complicate the exploration and recognition of signs and symptoms: the so-called ‘competing demands theory’. 52
Alternatively, health professionals may incorrectly attribute symptoms to existing conditions; for example, osteoarthritis (OA). 53 The cognitive assessment of disease by nsHCPs has been the subject of a recent study involving functional magnetic resonance imaging. 54 Here, decision making was related to a reduction of uncertainty about a diagnosis. 54 How nsHCPs determine whether a symptom may be attributed to PAD and uncertainty surrounding this decision would provide important insights into PAD recognition and stimulate the development of strategies to increase disease recognition.
Trainees and students
Increased knowledge of PAD was observed when nsHCPs/trainees were exposed to early vascular clinical experience, had a greater level of training, or experience of cardiovascular disease. 55 Adult learning theory holds that people learn new knowledge and skills most effectively when they are presented in the context of the application of new knowledge within real-life situations. 56 Teaching methods for trainees could include early patient contact/clinical experience, multimedia, and utilising smart phones for teaching.57,58 These may be with virtual or real patients – both are documented to promote meaningful theory learned using visual, audio, and verbal experiences and acquiring complex skills and knowledge. 58
Early clinical experience provides context to theoretical learning and improves understanding of how to apply new knowledge.59,60 This includes how patients describe symptoms and how practitioners may recognise disease. For example, with the knowledge that PAD often presents with similar features to other diseases, such as OA, trainees may be taught to screen for PAD alongside OA. Future research aims to provide an insight into the exposure and training of PAD within medical schools correlated with trainee awareness, knowledge, and confidence in its recognition. Using quantitative methods, including direct knowledge testing, and qualitatively exploring student knowledge would provide an understanding of how the education curriculum provides future nsHCPs with the tools to recognise and prevent diseases. Equally, it would identify whether additional educational resources are required to improve PAD knowledge.
While practitioners are expected to engage in continuing professional development to update their knowledge, there is a rapidly expanding landscape of medical information, increased provision of guidelines, and more conditions to diagnose. There is a plethora of platforms to provide educational material for nsHCPs, including web-based learning, interactive group discussion, individual learning, and group learning.60,61 Although there are more resources available online, group learning which allows essential practical skills training would be most suitable for PAD.61,62 Future research should evaluate the knowledge of health professionals at different stages of training, including associated clinical reasoning, to identify effective education interventions to improve PAD knowledge.
Strengths and limitations
This is the first review of publications concerned with knowledge about PAD to identify the levels of knowledge with insight into its determinants for patients/public, health professionals, and their trainees. The studies consistently report low levels of knowledge within the groups, which highlights an opportunity to improve knowledge and hence management of this important disease. There are, however, limitations which impact the quality of the review. The heterogeneous nature of the studies did not enable direct comparisons of the methods, settings, and knowledge measure, nor could a meta-analysis be undertaken. The results gathered were presented for trainee doctors, GPs, nurses, and podiatrists. Despite a broad search strategy, no information is known about the knowledge of other specialties, such as general-internal medicine, emergency medicine, and cardiovascular and endocrine medicine, within the available literature. It is recognised that within different countries, patients may first encounter these specialists. However, the information gained provided both qualitative and quantitative outcomes.
A number of studies included in this review (70%) were of low or moderate quality. Studies were particularly at risk of selection and reporting bias, and many had relatively small sample sizes. While results were relatively consistent across all studies, they should be interpreted with this risk of bias in mind, which limits the strength of the conclusions of this review. Inclusion of a conference abstract raises contention as vital study details may not be provided and there may be little peer review before publication. Although removing this study would have increased the overall study quality, it would have limited the scope of this deliberately broad study.
Conclusion
Knowledge of PAD is lacking in both patients/public and nsHCPs. Knowledge levels could be improved through educational interventions, such as individually tailored patient education or greater clinical exposure, to increase patient and nsHCP knowledge and recognition for earlier PAD treatment. We contend that education is both a critical component of an individual’s health and a contributing cause of other elements of the individual’s concurrent and future health. When PAD awareness gaps are improved by access to knowledge, an informed patient is best positioned to diminish risk in collaboration with an informed clinical provider.
Supplemental Material
Supplementary_information_-_Discrete_domains_of_evidence_final – Supplemental material for Knowledge of peripheral artery disease: What do the public, healthcare practitioners, and trainees know?
Supplemental material, Supplementary_information_-_Discrete_domains_of_evidence_final for Knowledge of peripheral artery disease: What do the public, healthcare practitioners, and trainees know? by Bernadeta M Bridgwood, Andrew TO Nickinson, John SM Houghton, Coral J Pepper and Rob D Sayers in Vascular Medicine
Footnotes
Acknowledgements
The authors would like to thank George Davies and the George Davies Charitable Trust for the generous charitable donation that funded this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Andrew Nickinson and John Houghton are funded and Bernadeta Bridgwood and Rob Sayers are partially funded through the George Davies Charitable Trust (registered charity number: 1024818). The trust had no role in the study design, analysis, manuscript preparation or any publication decisions. All researchers acted independently with no conflicts of interest.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.