
Abstract

Keywords
Risk stratification in acute pulmonary embolism (PE) is critical in identifying patients most likely to suffer clinical decompensation and therefore more likely to benefit from advanced therapies. Multiple computed tomography (CT) parameters have prognostic value in identifying those at highest risk for adverse clinical outcomes. 1 Dual energy CT (DECT) allows for the visualization of parenchymal iodine distribution as a surrogate of lung perfusion (Figure 1). 2 Perfusion defects corresponding to decreased blood flow in the setting of vascular occlusion are automatically quantifiable as iodine concentration per lung volume with artificial intelligence-based software.3–5
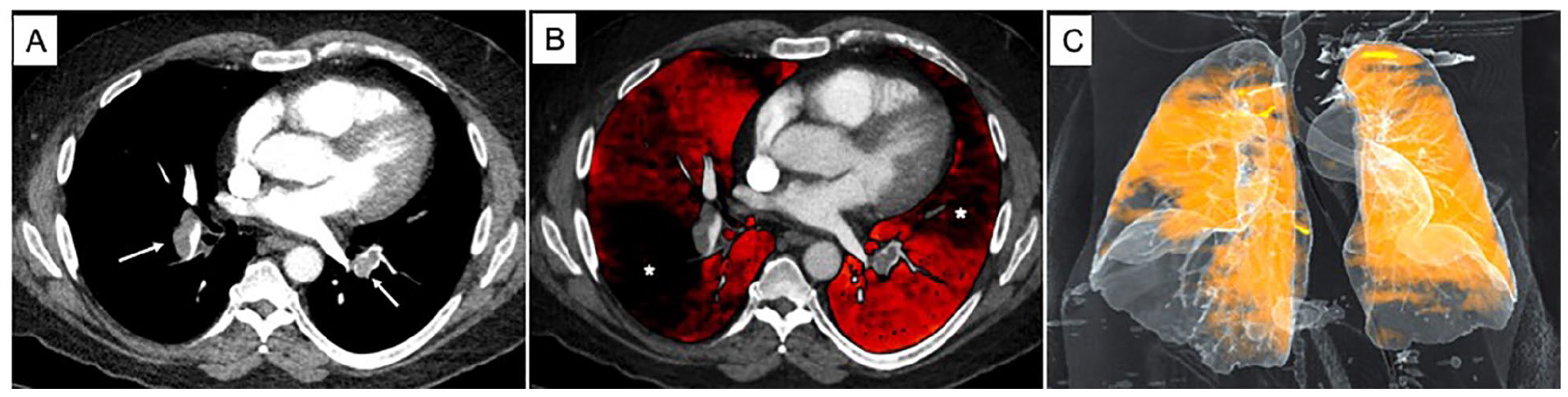
Dual energy CT images.
Although several studies have demonstrated perfusion defect maps can aid in the detection and diagnosis of PE, there are limited data pertaining to patient outcomes.1,2,6–8 As quantitative measures of perfusion defects can be immediately available following PE diagnosis without added radiation dose, we sought to determine whether there was an association between the magnitude of perfusion defects with patient outcomes.
We performed a retrospective analysis of consecutive pulmonary embolism response team (PERT) activations at our institution between September 2017 and August 2020 and identified patients who underwent DECT with calculated iodine concentration scores as subsequently described. The study was approved by the NYU Langone Health Institutional Review Board (s19-00001). The primary endpoint was clinical decompensation or in-hospital cardiac arrest (IHCA). Clinical decompensation was defined according to previously published adult inpatient decompensation event (AIDE) criteria which include the need for invasive mechanical ventilation, severe hypoxemia, and use of vasopressor or inotrope medication. 9 Patients with end-stage malignancy were excluded from the analysis.
All patients were scanned on Force scanners (Siemens Healthineers, Forchheim, Germany) using CareDose in dual energy mode. The dual energy image volume pairs were loaded into a prototype, Dual Energy Lung Isolation, on the eXamine platform (Siemens Healthineers) for analysis. This prototype automatically determines the lobular boundaries using a generative machine learning technique and computes the concentration of iodine in the lungs using a material decomposition technique.4,5,8 On a per lobe and per lung basis, the prototype reports the overall volume (mL), amount of iodine (mg), and the iodine concentration (mg/mL). For the purpose of this analysis, the whole-lung mean concentration (mg/mL) was reported. Patient characteristics were summarized using descriptive statistics. Data were presented as median with SD, mediate with IQR, or number (n) with percentage (%). Data were analyzed using Wilcoxon rank-sum, Pearson’s chi-squared, and Fisher’s exact tests, as appropriate. We performed a multivariable logistic regression analysis to determine the association between the primary outcome with the iodine score. Confounders included in the model were selected based on clinical plausibility and included age, sex, history of cardiopulmonary disease, and history of cancer.
Of the 357 patients in the PERT database, 217 underwent DECT and had iodine scores available for review. Nine patients were excluded due to poor contrast timing and an additional six were excluded due to the diagnosis of end-stage malignancy. Of 202 remaining patients, 21 (10.4%) suffered the outcome of AIDE or IHCA. Compared to those without clinical decompensation or IHCA, patients were similar in age (68 years vs 61 years), female sex (57% vs 53%), and medical history with respect to cardiopulmonary disease and cancer (online Supplemental Table 1).
Patients meeting the combined outcome of AIDE and IHCA were predominantly categorized as submassive PE (19 of 21 patients) with one uncomplicated and one massive PE patient. Of the 181 patients not meeting the outcome, 51.4% were submassive, 48.1% were uncomplicated, and one patient was a massive PE. Patients meeting the outcome had higher heart rates (118 BPM vs 95 BPM), lower systolic blood pressures (113 mmHg vs 128 mmHg), and higher respiratory rates (26 vs 18). Of the 21 patients meeting the outcome, seven underwent catheter-directed therapy (CDT) whereas two of the 181 patients without the outcome underwent CDT. Whole-lung mean iodine concentration was significantly lower among those with AIDE or IHCA compared to those who did not progress to decompensation or IHCA (0.79 mg/mL [IQR 0.67–0.89] vs 0.96 mg/mL [IQR 0.78–1.12], respectively, p = 0.007) (online Supplemental Figure 1). In the multivariable analysis, we found an association between the odds of the primary outcome and iodine score with an adjusted OR of 0.08 (95% CI 0.009–0.776) (online Supplemental Table 2).
In this retrospective analysis of 202 patients with confirmed PE seen by our PERT, lower mean whole-lung iodine concentration was associated with clinical decompensation or cardiac arrest. Previously, two small studies found that the extent of perfusion defects on DECT correlated with adverse clinical outcomes in PE.2,7 However, prior investigators performed volumetric analysis of defects manually outlining regions of reduced iodine content. The manually segmented regions were used to estimate a perfusion defect volume which was compared to total lung volume. 7 By contrast, we evaluated quantitative parenchymal perfusion using deep learning-based software (Dual Energy Lung Isolation, eXamine; Siemens Healthineers). This method has the advantage of being fully automatic, generating scores reflective of lung perfusion that can be immediately available to the clinician.4,8 To our knowledge, this is the first study evaluating such artificial intelligence-based software in the risk stratification of acute PE. Limitations to our study include lack of data on RV/LV ratios and the limited number of outcomes restricting our multivariable analysis. Selection bias is present as we only included PERT activations rather than all patients with PE. However, this likely concentrated the number of submassive and massive PE patients. We selected AIDE as one of our outcomes based on a large expert consensus and validation; however, other important clinical outcomes (such as a decline in blood pressure) may have captured additional events. From the technical perspective, perfusion imaging provides a single data point in time, which may evolve over the course of a patient’s admission. Parenchymal disease may produce defects unrelated to perfusion abnormalities as a consequence of the PE. A larger study with more outcomes would be necessary to understand whether quantifying parenchymal perfusion can be incorporated into the risk stratification of patients with acute PE.
In conclusion, we have shown that dual energy CT iodine maps demonstrate parenchymal perfusion defects in PE. The degree of perfusion abnormality is quantifiable with artificial intelligence software. Reduced iodine scores correlate with adverse clinical outcomes in acute PE.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221143818 – Supplemental material for Reduced CT iodine perfusion score is associated with adverse clinical outcomes in acute pulmonary embolism
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221143818 for Reduced CT iodine perfusion score is associated with adverse clinical outcomes in acute pulmonary embolism by Eugene Yuriditsky, Oscar J L Mitchell, William H Moore, Akhilesh K Sista, Shari B Brosnahan, Rogelio Cruz, Nancy E Amoroso, Ronald M Goldenberg, Deane E Smith, Catherine Jamin, Thomas S Maldonado and James M Horowitz in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Oscar JL Mitchell is supported by a T32 grant from the National Institutes of Health (T32 5T32HL007891); and James M Horowitz receives funding from Inari and Penumbra. The remaining authors report no conflict of interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.