
Abstract
Risk stratification of acute pulmonary embolism (PE) is important to identify patients at risk for hemodynamic collapse who would benefit from more aggressive therapies. Angiopoietin-2 (Ang-2) is a signaling molecule involved in angiogenesis and is upregulated in response to tissue hypoxia. We aimed to assess the association of Ang-2 with (1) PE severity, (2) echocardiographic and invasive hemodynamic markers of right ventricular (RV) dysfunction, and (3) need for intensive treatment. Patients presenting to our institution with acute PE were included in a prospective database and blood samples were collected and stored for later analysis. A total of 65 patients were included in the study. Ang-2 correlated with PE risk stratification and echocardiographic and invasive hemodynamic markers of RV dysfunction and pulmonary hypertension. An Ang-2 level of > 4101 pg/mL had an odds ratio of 7.4 (95% CI: 1.53–12.5, p < 0.01) for intensive care unit (ICU) admission. In conclusion, Ang-2 correlates with PE severity, RV dysfunction, and need for ICU admission. Ang-2 holds promise as a novel marker that can aid in risk stratification for this patient population.
Introduction
Pulmonary embolism (PE) is a common cause of morbidity and mortality accounting for up to 300,000 deaths in the United States each year.1,2 The clinical presentation of PE is highly variable, ranging from mild symptoms of dyspnea to sustained hypotension and shock. 3 As a result, a number of clinical prediction models have been created in order to stratify patients according to their risk for hemodynamic collapse and death.1,4–8 A recent analysis showed that commonly used risk prediction models had only modest ability to predict 7- and 30-day mortality. 9 Therefore, identification of additional markers that can predict poor outcomes in patients presenting with acute PE is of significant clinical importance.
Angiogenesis in adults is tightly regulated through a variety of activating and inhibitory signals including Angiopoietin-1 and -2 (Ang-1 and -2) and their receptor, Tie-2. 10 Binding of Ang-1 to the Tie-2 receptor results in activation of intracellular pathways which promote endothelial cell survival and vascular stability. In contrast, Ang-2 is a weaker agonist of the Tie-2 receptor and allows the endothelium to respond to angiogenic signals and promotes vessel sprouting. Transcription of Ang-2 is induced by tissue hypoxia. 10
We performed a study to assess the association of Ang-2 with (1) PE severity, (2) echocardiographic and invasive hemodynamic markers of right ventricular (RV) dysfunction, and (3) need for intensive treatment.
Methods
Patients presenting to Loyola University Medical Center (LUMC) with acute PE were included in a prospective database and consenting patients underwent phlebotomy for research purposes following hospital admission. A random selection of patients with varying PE severity (as defined by the European Society of Cardiology classification system 1 ) were selected for inclusion in this study using a random number generator.
Baseline clinical characteristics, laboratory data, and patient outcomes were collected by reviewing relevant electronic medical records. All medical decisions including patient disposition and treatment strategies were made by the treating physician independent of the study. A subset of patients underwent catheter directed intervention as part of their clinical care. In these patients, right heart catheterization was performed at the time of the procedure. A 6F Swan-Ganz catheter (Edwards Lifesciences, Irvine, CA, USA) and a fluid filled transducer to measure the right atrial (RA), RV, and pulmonary artery (PA) pressures were utilized. Cardiac output (CO) was obtained using the Fick method after determining the mixed venous oxygen saturation and then indexed to body surface area to obtain cardiac index (CI).
All patients underwent transthoracic echocardiography and measurements were made according to published guidelines.11,12 The right ventricle/left ventricle (RV/LV) ratio was obtained using the RV and LV internal diameter in diastole (1 cm apical to the atrio-ventricular valves) from the apical four-chamber view. S prime (S′) was assessed using tissue Doppler velocity of the lateral tricuspid annulus in the apical four-chamber view. Similarly, tricuspid annular plane systolic excursion (TAPSE) was measured using M-mode tracings of the lateral tricuspid annulus in the apical four-chamber view. The RV acceleration time (AT) was obtained using pulsed wave Doppler of the RV outflow tract (RVOT) in the parasternal short axis view at the level of the aortic valve and measuring the time from zero to peak velocity in milliseconds. The modified Bernoulli equation was used to estimate the PA systolic pressure (PASP) utilizing the tricuspid regurgitant velocity and adding the estimated RA pressure. RA pressure was estimated in accordance with previously published guidelines. 11 RVOT velocity time integral (VTI) was measured using pulsed waved Doppler in the RVOT immediately adjacent to the pulmonic valve, while LV outflow tract (LVOT) VTI was measured using pulsed wave Doppler in the LVOT immediately adjacent to the aortic valve.
Blood samples were collected on the day of hospital presentation and stored frozen at –80°C at the Loyola University Cardiovascular Research Institute until time of analysis. All samples were analyzed using a commercially available ELISA kit for Human Ang-2 (R&D Systems, Minneapolis, MN, USA). Results are given as gravimetric quantity according to the calibration of the assay.
To explore the relationship between Ang-2, clinical, and hemodynamic data, patients were divided into tertiles based on the degree of elevation of Ang-2 (highest, middle, and lowest tertile of Ang-2).
The study was approved by the Institutional Review Board at LUMC.
Statistical analysis
Statistical analysis was performed using IBM SPSS 25.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to evaluate the data for normality of distribution. Non-normally distributed data were expressed as median (IQR). Comparisons between groups were evaluated using the nonparametric Mann–Whitney U-test, and Kruskal–Wallis test. Correlation analysis was performed by Spearman rank-order correlation coefficient. A binomial logistic regression model was designed to evaluate explanatory variables as a predictor of intensive care unit (ICU) admission. Receiver operating characteristic (ROC) curves were constructed to illustrate the sensitivity and specificity of the simplified pulmonary embolism severity index (sPESI) 6 and Ang-2 to predict ICU admission. Youden’s J statistic was calculated to determine optimal cut-off values. 13 Significance was considered at p ⩽ 0.05.
Results
A total of 65 patients with acute PE were included in the study (low risk (n = 18), intermediate risk (n = 39), and high risk (n = 8)). Baseline clinical characteristics are shown in Table 1.
Baseline characteristics.
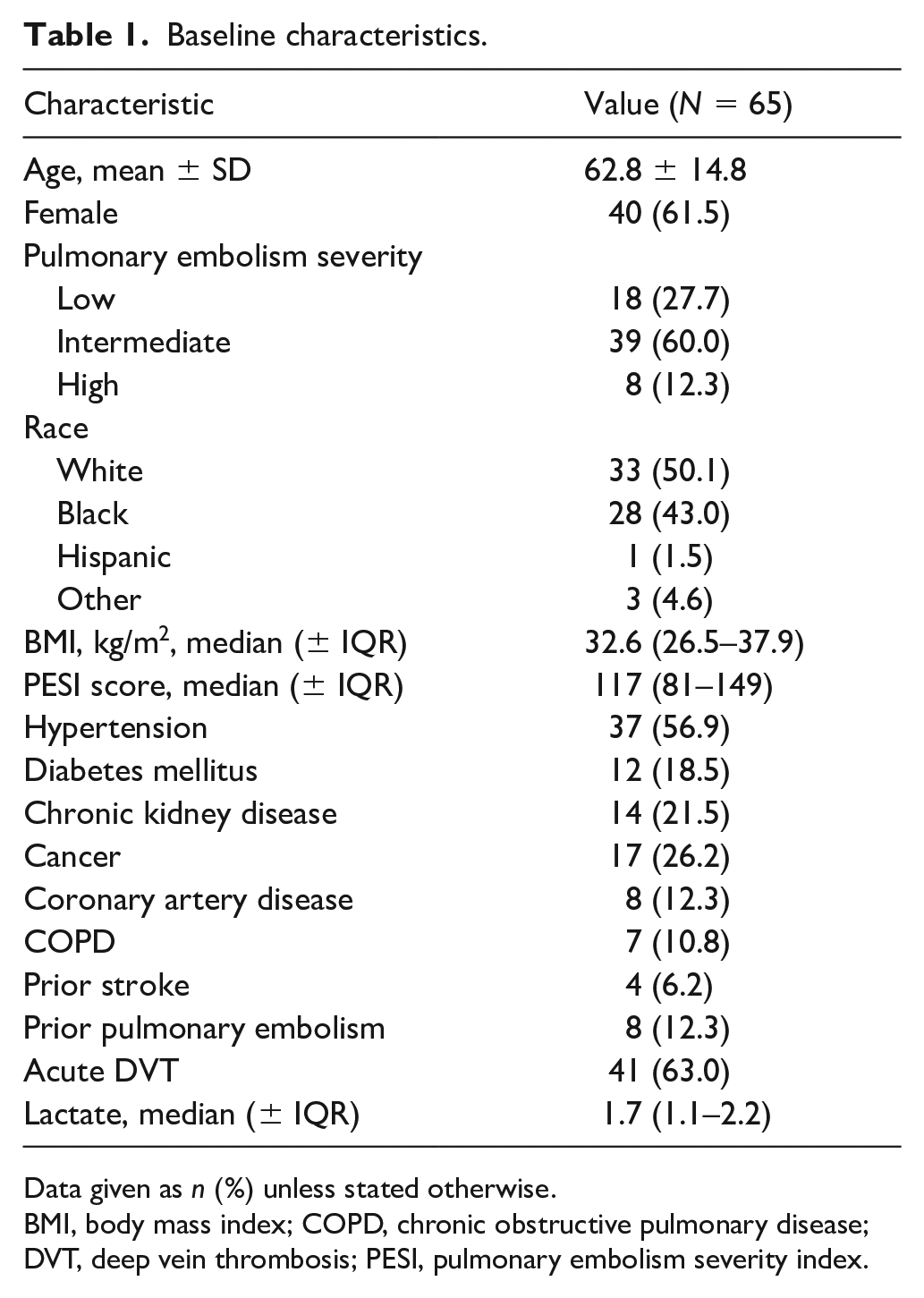
Data given as n (%) unless stated otherwise.
BMI, body mass index; COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; PESI, pulmonary embolism severity index.
Patients with greater severity PE had higher levels of Ang-2 (median values ± IQR: low risk = 3599 (2679–5124) pg/mL, intermediate risk = 3850 (3160–4773) pg/mL, and high risk = 11,461 (7032–25,600) pg/mL; p = 0.03).
Mean arterial pressure (MAP) on presentation was highest among patients in the lowest Ang-2 tertile and decreased in a stepwise fashion between the middle and highest tertile groups. Presenting heart rate, respiratory rate, and oxygen saturation did not differ significantly between groups, though there was a trend towards lower oxygen saturation and higher respiratory rate among the highest Ang-2 tertile (Table 2).
Presenting vital signs and Ang-2 tertile.
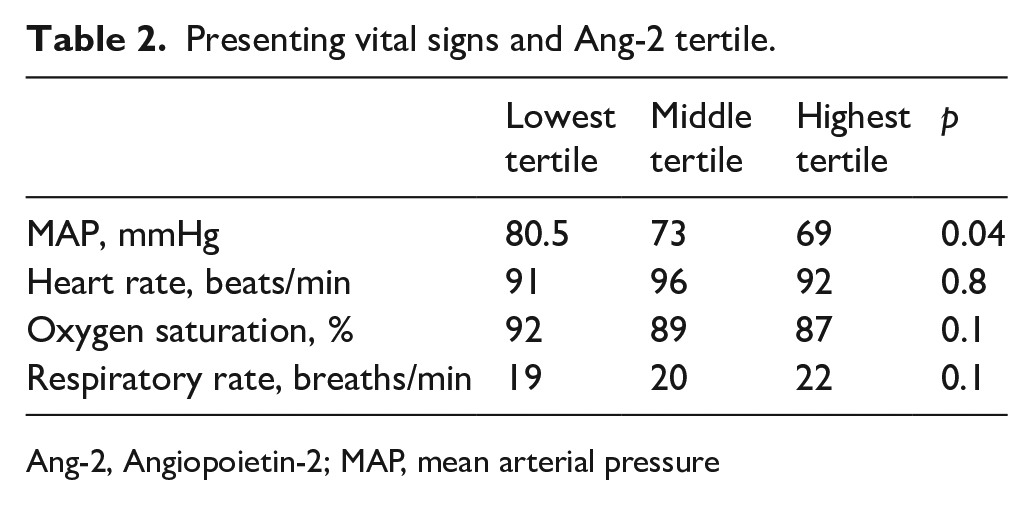
Ang-2, Angiopoietin-2; MAP, mean arterial pressure
On echocardiography, PASP was highest and RV AT and RVOT VTI were lowest among patients in the highest Ang-2 tertile. Although not statistically significant, there was a trend towards lower S′, TAPSE, and LVOT VTI among this group of patients (Table 3).
Echocardiographic findings and Ang-2 tertile.
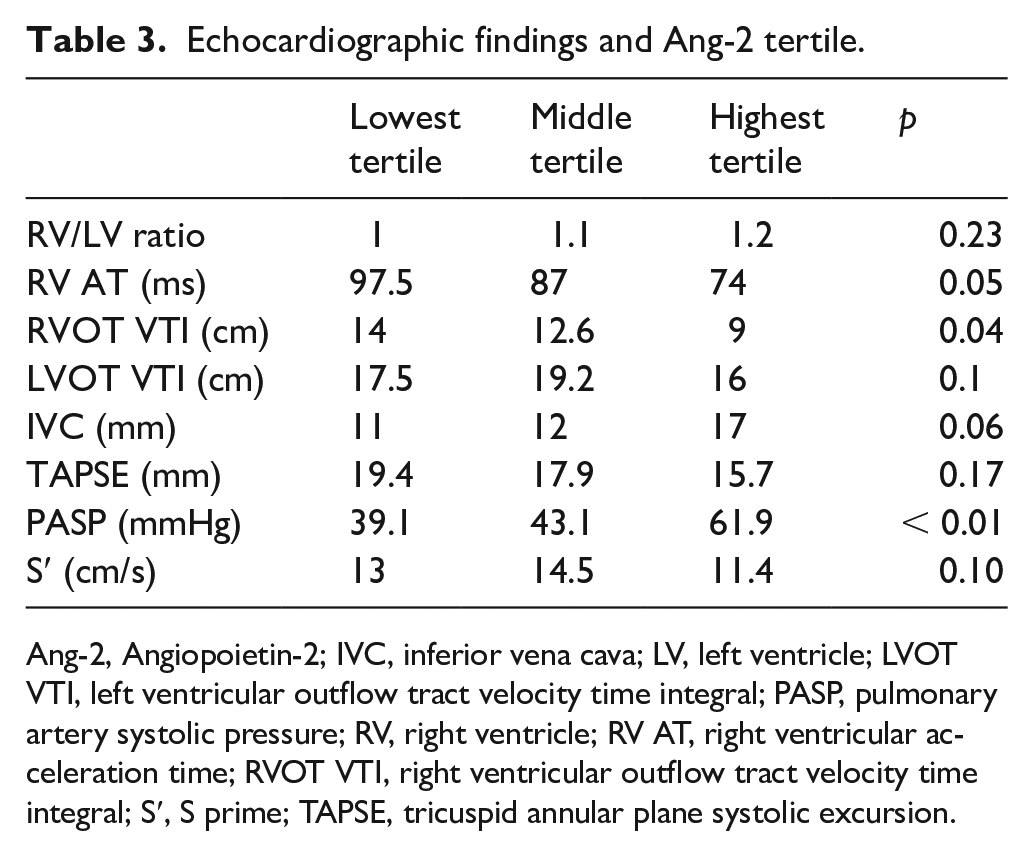
Ang-2, Angiopoietin-2; IVC, inferior vena cava; LV, left ventricle; LVOT VTI, left ventricular outflow tract velocity time integral; PASP, pulmonary artery systolic pressure; RV, right ventricle; RV AT, right ventricular acceleration time; RVOT VTI, right ventricular outflow tract velocity time integral; S′, S prime; TAPSE, tricuspid annular plane systolic excursion.
Invasive hemodynamic data were available in the 25 patients who underwent catheter directed thrombolysis. In this population, there was a positive correlation between invasively measured PASP and Ang-2 (r = 0.59, p < 0.01) and an inverse correlation with invasively measured CI (r = −0.47, p < 0.01) and PA pulsatility index (r = −0.5, p < 0.01) and Ang-2 (Figures 1A–C).
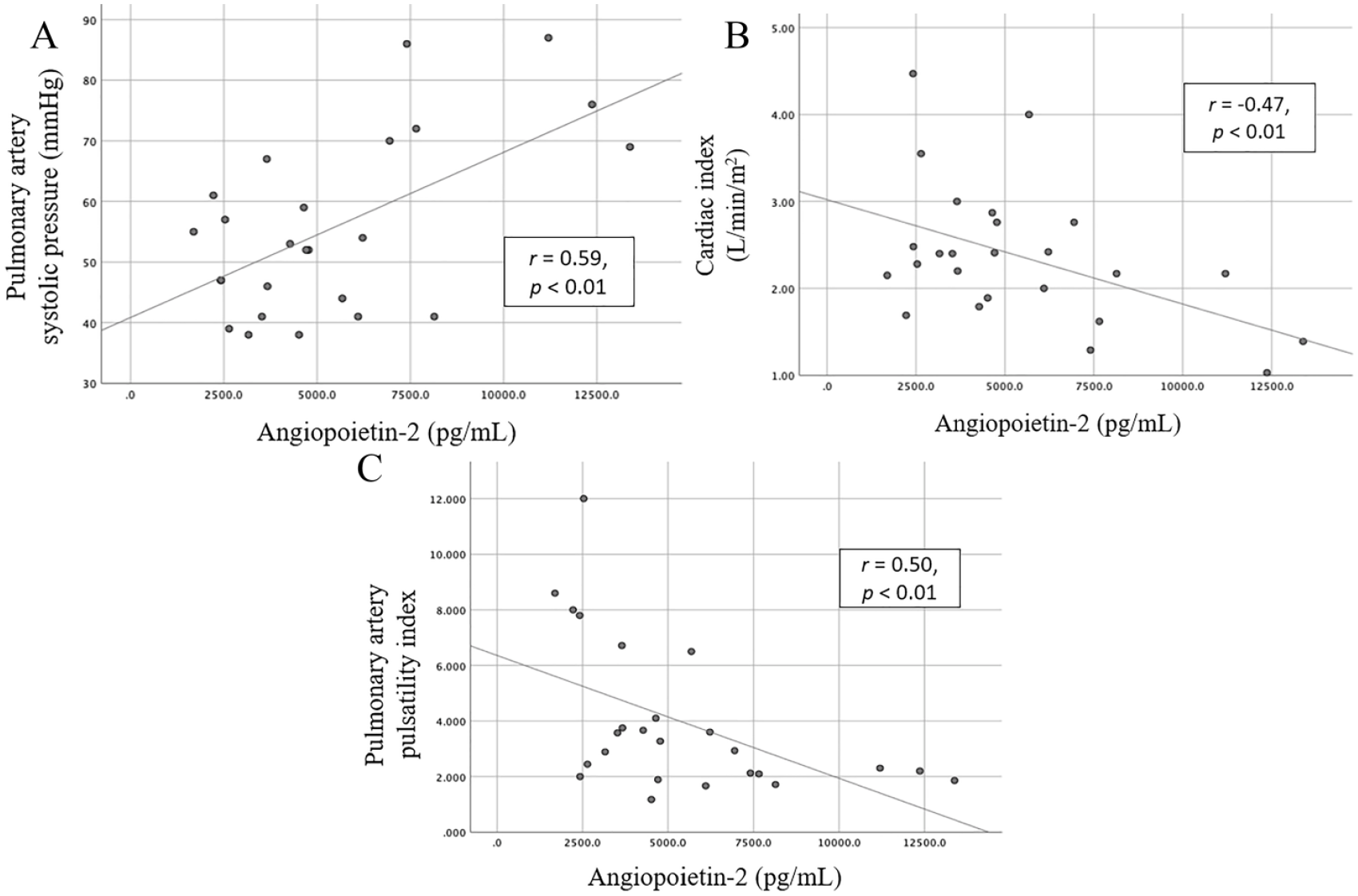
Scatter plot of Angiopoietin-2 and (A) invasively measured pulmonary artery systolic pressure, (B) cardiac index, and (C) pulmonary artery pulsatility index.
Using a ROC curve, we identified an Ang-2 level of 4101 pg/mL had a sensitivity and specificity of 68% for ICU admission. In univariate analysis, an Ang-2 level of > 4101 pg/mL had an odds ratio (OR) of 7.4 (95% CI: 1.53–12.5, p < 0.01) for ICU admission. ORs for other commonly evaluated prognostic markers including D-dimer, PESI score, brain natriuretic peptide (BNP), and troponin are shown in Table 4. Optimal cut-off values for each marker were determined using ROC curves. In a multivariate analysis including troponin, BNP, and Ang-2, no marker was found to be significantly associated with ICU admission; however, Ang-2 demonstrated a strong trend towards significance (OR 3.7, 95% CI: 0.97–13.9, p = 0.056) (Table 4).
ORs for ICU admission by risk predictor.
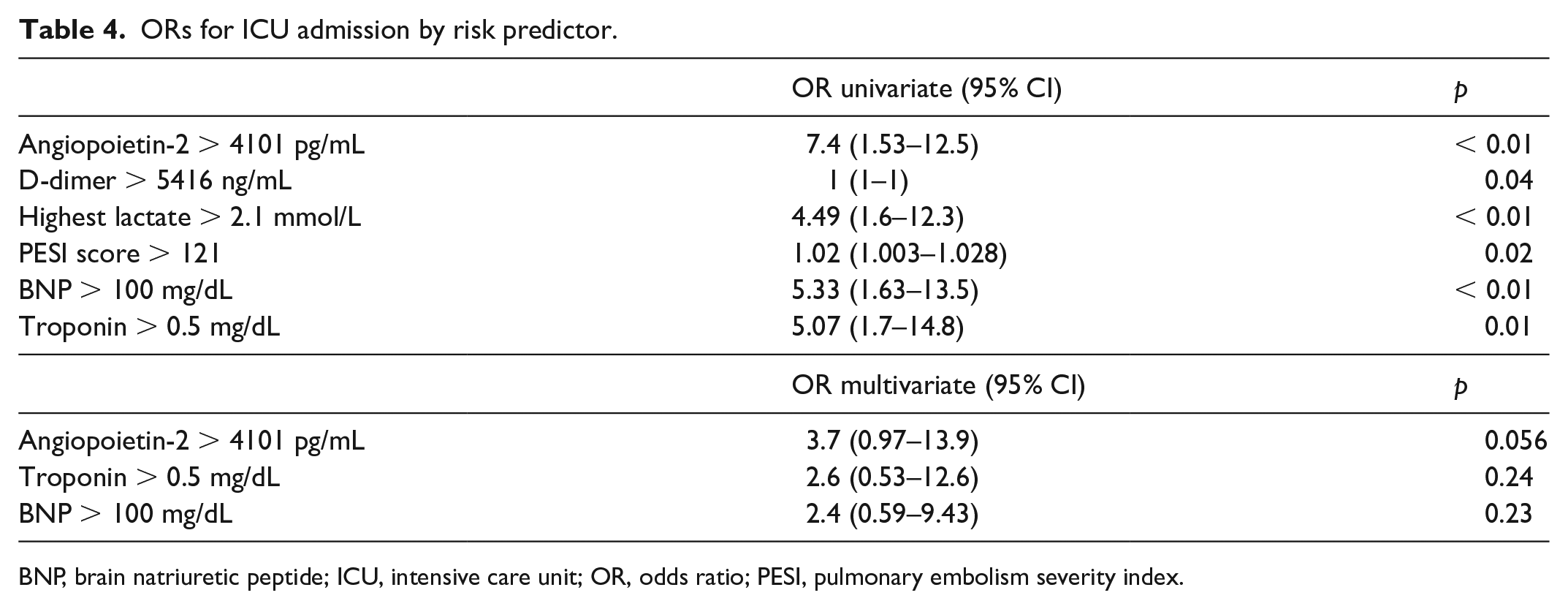
BNP, brain natriuretic peptide; ICU, intensive care unit; OR, odds ratio; PESI, pulmonary embolism severity index.
Finally, to determine whether elevated Ang-2 provided additive value beyond commonly used PE prognostic scoring systems, we created a modified version of the sPESI 6 score, which also granted a point for an Ang-2 > 4101 pg/mL. In the subsequent ROC curve analysis evaluating for ICU admission, the modified sPESI score had an area under the curve of 0.682 compared to the traditional sPESI score which had an area under the curve of 0.638 (Figure 2).
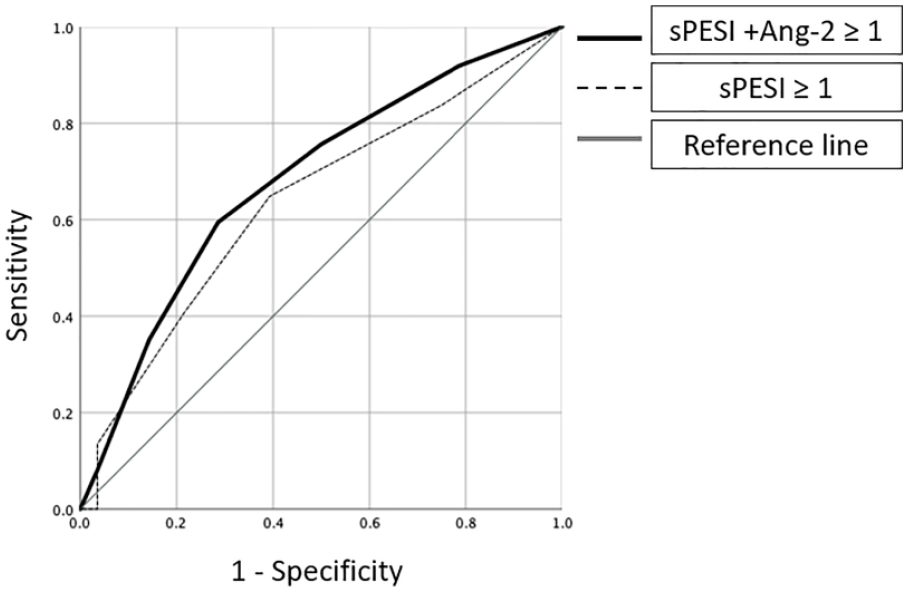
Receiver operating characteristic curves for ICU admission using the sPESI score compared with a modified sPESI score which also incorporates an elevated Ang-2 (i.e., > 4101 pg/mL).
Discussion
Our study evaluated the relationship between Ang-2 and PE severity, echocardiographic and invasive hemodynamic markers of RV dysfunction, and need for ICU admission. We identified the following novel findings: (1) Ang-2 was highest among patients with the highest-risk PE; (2) Ang-2 was associated with echocardiographic and invasive hemodynamic markers of RV dysfunction; (3) Ang-2 was correlated with need for ICU admission; and (4) in a bivariate logistic regression model, Ang-2 had a signal for predicting ICU admission, whereas troponin and BNP were not significant explanatory variables.
Ang-2 has been associated with worse prognosis in a variety of disease processes including congestive heart failure, 14 cardiogenic shock,15,16 pulmonary hypertension, 17 and acute lung injury and sepsis. 18 In our study, there was an increase in Ang-2 with increasing severity of PE. There are multiple plausible explanations for this finding. Because hypoxia is a trigger for Ang-2 release, 19 the observed increase in Ang-2 with increasing PE severity could be reflective of worsened hypoxia among the highest risk group. Although not statistically significant, we found a trend towards worsened hypoxia among patients in the highest Ang-2 tertile. Alternatively, Ang-2 is known to be a mediator of the inflammatory process 20 and greater elevations of Ang-2 among patients with higher-risk PE in this study may be indicative of a more robust inflammatory response.
We also found that Ang-2 was associated with lower invasively measured CI and PA pulsatility index and higher PASP. A prior study investigated Ang-2 in patients with cardiogenic shock, and in line with our study found Ang-2 to be inversely correlated with both cardiac power index and mixed venous oxygen saturation. 15 Similarly, in a population of patients with idiopathic pulmonary arterial hypertension, Ang-2 was found to correlate directly with pulmonary vascular resistance and inversely with both CI and mixed venous oxygen saturation. 17
While the invasive hemodynamic data in our study were available in only 25 patients that underwent catheter directed thrombolysis, all patients included in the study underwent echocardiography and we therefore evaluated the association between Ang-2 and echocardiographic markers of cardiac function and pulmonary pressures in the overall cohort. In line with the invasive hemodynamic data, we found the group of patients comprising the highest tertile Ang-2 group had the highest PASP, shortest RV AT, and lowest RVOT VTI. These findings are consistent with a greater degree of pulmonary hypertension and RV dysfunction among patients with greater degrees of elevation of Ang-2. Whether these findings are indicative of a specific role of RV failure in stimulating Ang-2 production, or are merely reflective of increasing PE burden and the resultant hypoxia and inflammatory response that accompanies it, cannot be delineated in this observational, retrospective study.
Finally, we found that Ang-2 was predictive of ICU admission among patients presenting with PE. As previously stated, Ang-2 has been found to be a useful prognostic marker in several disease states.16–18 Although a multitude of clinical prediction models exist to aid in risk stratification of patients with acute PE, a recent multicenter study found four commonly used scores had only a modest correlation with 7- and 30-day mortality. 9 In our study, an Ang-2 level greater than 4101 pg/mL had an OR of 7.4 for ICU admission and appeared to be a stronger predictor of ICU admission than D-dimer, highest lactate, troponin, BNP, and PESI score. Further, in ROC analysis, addition of Ang-2 to the sPESI score resulted in an increased area under the curve for prediction of ICU admission. If validated in larger studies, this suggests that incorporation of Ang-2 into clinical care could improve the performance of commonly used risk prediction scores for acute PE. Whether Ang-2 correlates with mortality in this patient population is the subject of our ongoing investigations.
In a population of patients with cardiogenic shock, a decrease in Ang-2 in response to therapy was found among patients who survived, but not among those who died. 15 Whether changes in Ang-2 are predictive of response to therapy in the PE population is also under investigation.
Study limitations
The present study should be interpreted in the context of several limitations. First, this was a single center study with a limited patient population and most patients had either low- or intermediate-risk PE. Second, owing to the limited patient population, we were unable to assess whether Ang-2 correlates with mortality. Third, Ang-2 is currently an investigational biomarker that is processed in our translational research laboratory. Although results can be analyzed the same day at our center, the absence of Ang-2 from most clinical laboratories limits its direct clinical application at this time. However, if our findings are validated in a larger study, the addition of Ang-2 to routine clinical care could be warranted. Fourth, while Ang-2 correlated with many markers of RV dysfunction and increased illness severity in our study, there were several clinical, echocardiographic, and invasive hemodynamic variables with which Ang-2 had no definitive correlation. This warrants further investigation in future studies with larger patient populations. Finally, because blood samples were drawn at only a single time point, we are unable to determine whether Ang-2 changed in response to therapy.
Conclusions
In conclusion, Ang-2 is associated with PE severity, echocardiographic and invasive markers of RV dysfunction, and need for ICU admission. Further evaluation of Ang-2 as a marker of mortality in patients with acute PE is necessary to determine if it could aid in risk stratification.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by a grant from the Loyola University Chicago Health Science’s Campus Cardiovascular Research Institute. The funder had no role in the study design, data analysis, or manuscript preparation.