
Abstract

Keywords
The evaluation of treatment methods for patients with peripheral artery disease (PAD) usually focuses on technical success, rather than on patient-reported clinical success or quality of life. However, patient-reported outcome measures (PROMs) are important additive variables when evaluating vascular treatments.1–3 One of the main goals of treating patients with intermittent claudication is to restore daily activities and thus quality of life. However, a patient with critical limb ischemia might benefit more from treatment that relieves pain and prevents tissue loss. By only focusing on technical success, one might fail to see other factors that influence patient satisfaction and patient perception of successful treatment.
In this observational cross-sectional study, we investigated the correlation between the objective technical outcome ankle–brachial index (ABI) and PROMs, by means of the VQ-6-NL (shortened and validated Dutch version of the VascuQoL-6, a disease-specific quality of life instrument 4 ) and patient satisfaction after treatment (improvement versus no improvement of symptoms). Power analysis showed that 94 patients were necessary to measure a significant improvement in VQ-6-NL (power 90%, α = 0.05). A random sample of 330 patients was selected from a previously described cohort that underwent revascularization for femoropopliteal artery disease between 2004 and 2015. 5 All interventions were technically successful.
Patient characteristics, comorbidities and preinterventional ABI were collected from patients’ files. The definitions of the comorbidities are presented below. Diabetes mellitus was defined as a previously established diagnosis of glucose intolerance or the use of oral hypoglycemic therapy or insulin. Hypertension was defined as a previous diagnosis of hypertension or the use of blood pressure-lowering drugs. Ischemic heart disease was defined as the presence of a history of angina pectoris, myocardial infarction or coronary revascularization. Congestive heart failure was defined as the presence of left or right ventricular failure. Atrial fibrillation was defined as documented by electrocardiogram or previously diagnosed. Chronic renal failure was defined as a glomerular filtration rate of less than 30 mL/min/1.73 m2. Chronic obstructive pulmonary disease (COPD) was defined as a previously diagnosed obstructive disease according to the GOLD guidelines 6 and/or the use of inhalation medication. Hypercholesterolemia was defined as a previously established diagnosis of high cholesterol stated in the medical report.
The postinterventional ABI and PROMs were measured at an outpatient visit. Patients were excluded if the preinterventional ABI was unknown or undetectable, if they underwent an amputation of the treated leg, in the event of death or in case of poor understanding of Dutch. All participants gave informed consent. The local ethics committee approved this study.
We conducted a linear regression analysis to examine the association between postinterventional ABI and ΔABI and the VQ-6-NL. Multivariate logistic regression analysis investigated the effects of patient-related variables on the improvement of symptoms. We calculated the minimally important difference (MID) for the ABI, which is the smallest change in ABI that is clinically relevant, by using an anchor-based approach. The anchor question was ‘improvement of symptoms’.
A total of 95 patients with a mean follow-up of 5.8 years (SD ± 2.4) were included (for patient characteristics, see online Supplemental Table 1). The mean pre- and postinterventional ABI were 0.59 and 0.91, respectively. The average improvement in ABI in the total cohort was 0.32 (SD ± 0.3). The majority of patients reported an improvement of symptoms postinterventionally (71%). The mean VQ-6-NL score was 17 (SD ± 4.8). Patients with improvement had a higher VQ-6-NL score compared to patients with no improvement (19 vs 13, p < 0.001).
As expected, postinterventional ABI of the treated limb was significantly improved compared with preinterventional ABI (p < 0.001). Univariate analysis revealed that VQ-6-NL was significantly associated with postinterventional ABI and not with ΔABI (p = 0.04 and p = 0.32, respectively; Figure 1). Multivariate analysis revealed no association between VQ-6-NL and postinterventional ABI and ΔABI (p = 0.22 and p = 0.75).
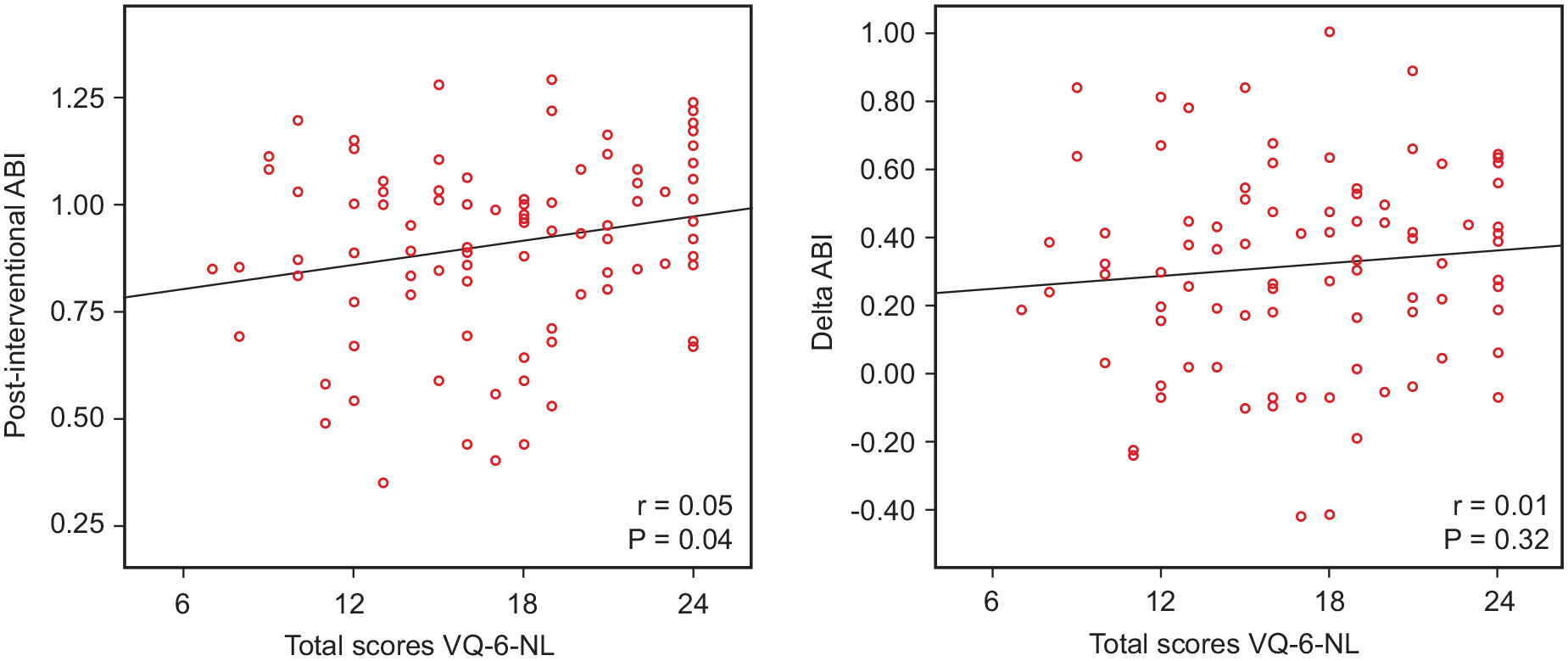
Scatterplot of postinterventional ABI and delta ABI versus total VQ-6-NL scores.
Patient satisfaction (improvement versus no improvement of symptoms) was significantly associated with a higher VQ-6-NL (p < 0.001; OR 1.5; 95% CI 1.3–1.9) and a shorter observation duration (p = 0.03; OR 0.7; 95% CI 0.5–1.0). The MIDs were 0.32 and 0.03 for improvement and deterioration, meaning that patients with a ΔABI of ⩾ 0.32 had improved in a clinically relevant way and an increase of less than 0.03 points is experienced as deterioration.
Interestingly, patients with a high VQ-6-NL did not have a higher postinterventional ABI or ΔABI compared with patients with a low VQ-6-NL score. These results are congruent with previously reported findings and underscore the importance of the additional use of clinical parameters for assessing revascularization procedures in PAD patients.7–9 Besides this, there had to be a ΔABI of at least 0.32 before patients experienced an improvement of symptoms. This finding is in contrast to the increase in ABI of at least 0.15 currently used by many clinicians and researchers as a clinically meaningful improvement.10–12
A limitation of this study is the large number of patients who could not participate. Many patients from the random sample were deceased, could not be reached, or refused to participate. The main reasons for nonparticipation were comorbid symptoms or hospitalization. This could imply that the study represented a selected group, and that our results may not be generalizable to a broader population. Secondly, no baseline VQ-6-NL score was known, so no comparison could be made for quality of life before and after intervention.
In conclusion, ABI was not independently associated with the clinical parameters VQ-6-NL or the reported symptomatic benefit after intervention. A high VQ-6-NL score was significantly associated with improvement of symptoms. A MID of ⩾ 0.32 of ΔABI was required to experience an improvement in symptoms, which might be a reason to reconsider this threshold. Our results show that ABI alone is not sufficient to evaluate treatment success and that PROMs are an important addition in the evaluation of revascularization methods.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221138879 – Supplemental material for Correlation of patient-reported outcome measures and the ankle–brachial index in patients who underwent revascularization for peripheral artery disease
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221138879 for Correlation of patient-reported outcome measures and the ankle–brachial index in patients who underwent revascularization for peripheral artery disease by Rianne J Vossen, Dianne Ras, Anco C Vahl, Vanessa J Leijdekkers, Alexander D Montauban van Swijndregt, Willem Wisselink and Ron Balm in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.