
Abstract
Introduction
Peripheral artery disease (PAD) is a significant medical concern as it is highly prevalent worldwide, affecting 202 million people. 1 Based on prevalence and size of published literature, PAD is ranked 15th of all chronic conditions in adults, similar to stroke and ahead of Alzheimer’s disease. 2 Additionally, PAD is costly, 3 and is associated with a high rate of all-cause and cardiovascular mortality. 4 A common symptom of PAD is claudication, 5 defined as lower extremity pain that is reproducibly induced by walking and relieved with rest, and which is secondary to inadequate blood flow to the exercising leg musculature. Consequently, claudication impairs ambulation, 6 physical function, 7 daily physical activity, 8 and health-related quality of life (HRQoL). 9
A primary recommendation for PAD patients is to improve claudication and HRQoL through supervised exercise therapy, 5 which has been given a Class IA recommendation supported by multiple randomized-controlled trials and meta-analyses.10,11 Home-based exercise studies have also demonstrated efficacy in improving claudication outcomes.12–16 Although reporting improvements in these outcomes following exercise rehabilitation programs is important to establish efficacy, determining the minimal clinically important difference (MCID) of outcomes in response to exercise intervention or longitudinal change is also an important consideration that has only recently been addressed in patients with PAD.17,18 The MCID represents the smallest threshold change in an outcome measure that patients consider beneficial. 19 Two approaches to determine MCID include the anchor-based and the distribution-based methods. The anchor-based method determines how much change in the outcome measure, such as daily physical activity, is needed for patients to perceive improvement in another health metric, such as HRQoL. The distribution-based method assesses the distribution of the daily activity outcome measures, as well as the variability and reliability to estimate effect size and standard error of the measurement.
Measurement of daily steps is a key metric for patients with PAD because it is the primary activity that elicits claudication, walking is the most common form of exercise performed by older adults,20,21 and steps are a basic unit of locomotion that can also quantify intensity of physical activity. 22 Thus, number of daily steps and step rate (i.e., cadence), and the time spent in moderate-to-vigorous physical activity (MVPA), 23 are clinically relevant and appropriate metrics to evaluate daily activity levels in patients with claudication. We have found that home-based and supervised exercise programs increase the daily physical activity levels of patients with PAD and claudication.12,13,24 However, the amount of change in daily steps and in time spent in MVPA needed to be clinically meaningful, as determined by MCID, have not been established in patients with PAD.
Therefore, in an exploratory analysis from our previous randomized-controlled trial, 13 our aim of this study was to estimate the MCID for small, moderate, and large changes in daily step counts and time spent in MVPA following both home-based and supervised exercise programs in patients with PAD and claudication.
Methods
Patients
Approval and informed consent
The procedures of this study were approved by the institutional review board at the University of Oklahoma Health Sciences Center. Written informed consent was obtained from each patient at the beginning of investigation.
Recruitment
Patients who had claudication and who were not currently exercising were recruited from vascular laboratories and vascular clinics from the University of Oklahoma Health Sciences Center for possible study enrollment. 13 Patients were screened on inclusion and exclusion criteria, as previously described. 13 Patients participated in the study from October 2006 to July 2012. 13
Medical screening
Patients were evaluated in the morning at the Clinical Research Center, at the University of Oklahoma Health Sciences Center. 13 Patients arrived fasted, but were permitted to take their usual medications. Patients were evaluated with a medical history and physical examination in which demographic information, height, weight, waist circumference, cardiovascular risk factors, comorbid conditions, claudication history, blood samples, and a list of current medications were obtained. After 10 minutes of supine rest, the ankle and brachial systolic blood pressures were obtained according to standard guidelines, 25 in which the higher ankle systolic pressure of each leg (posterior tibial or dorsalis pedis) and the arm with the higher brachial systolic pressure were used to calculate ankle/brachial index (ABI). Patients performed a standardized Gardner–Skinner graded treadmill protocol 6 to determine study eligibility, claudication onset time, and peak walking time, as previously described. 6 Furthermore, patients performed a 6-minute walk test in which two cones were placed 100 feet (i.e., 30.48 meters) apart in a marked corridor to determine 6-minute walk distance, as previously described. 26
Intervention and control groups
Home-based exercise rehabilitation program
The home-based exercise program consisted of 3 months of intermittent walking to mild-to-moderate claudication pain at least 3 days per week at a self-selected pace, in which exercise duration was progressively increased from 20 to 45 minutes per session, as previously described.12,13
Supervised exercise rehabilitation program
The supervised program consisted of 3 months of intermittent treadmill walking to mild-to-moderate claudication pain 3 days per week at a speed of approximately 2 miles/hour and at a grade equal to 40% of the highest workload achieved during the baseline maximal treadmill test.12,13,27 Exercise sessions progressively increased during the program from 15 to 40 minutes. 13
Attention-control, light resistance program
Light resistance training was performed three times per week, without any walking exercise, using a Pro-Form Fusion 6.0 LX weight system (ICON Health & Fitness Inc, Logan, UT). 13 Resistance training consisted of performing both upper and lower extremity exercises. One set of 15 repetitions was performed for each exercise.
Outcome measurements
Patients were evaluated on daily step counts and HRQoL outcome measurements during baseline testing and after the 3-month intervention period, as described below.
Ambulatory activity monitoring
Daily walking was measured using a step activity monitor (StepWatch3™; Orthoinnovations, Inc., Oklahoma City, OK, USA) during 7 consecutive days, as we have previously described.8,28–31 Patients were instructed to wear the monitor during waking hours, to remove it before retiring to bed and while showering, and to engage in their normal routine daily activities. To be truly representative of normal daily activities, we only performed activity monitoring as an outcome measure during 7 consecutive days before and after the study, and not during the 12-week intervention phase. By proceeding in this manner, we did not mix exercise intervention sessions from three different exercise groups into the weekly assessment of the normal physical activity pattern of patients.
The step activity monitor was attached to the right ankle above the lateral malleolus using a Velcro strap, and continuously recorded the number of steps taken on a minute-to-minute basis. We quantified the total number of daily steps, and the amount of time spent in MVPA in the community setting, defined as exceeding a cadence of 60 steps per minute by patients with claudication. 8 This cadence represents a level beyond purposeful stepping in adults,32,33 exceeds 60% of the maximal cadence of patients with claudication during a 6-minute walk test, 26 and exceeds 67% of the average cadence of supervised treadmill exercise training sessions completed by patients with claudication. 13 The daily ambulatory steps were further analyzed by the software program, and quantified into the following variables: maximum cadence for 5 and 30 continuous minutes of ambulation each day. The accuracy of the step activity monitor exceeds 99 ± 1% in patients with intermittent claudication, 8 and the test-retest intraclass reliability coefficient (IRR) for the measurement of total daily steps during a 7-day period is IRR = 0.87. 8
Medical Outcomes Study Short-Form 36 (MOS SF-36 – RAND, Version 1.0)
The self-reported physical function subscale of HRQoL was assessed from this instrument. 34 We previously found that the physical function subscale was the most impaired subscale in patients with symptomatic PAD compared to national norms. 35 Thus, we selected the physical function subscale as the anchor for the anchor-based method to determine small, moderate, and large MCID values for the daily step count outcome measures.
The physical function scale is comprised of 10 questions about performing daily activities with answer selections that include the following: limited a lot, limited a little, and not limited at all. A change in one level of a question (e.g., a pretest response is limited a lot, and the post-test response is limited a little) is equal to a 5% change in the total physical function subscale. We considered a one-level change in any one of the 10 questions for the physical function subscale to represent a small MCID of 5%. 17 Based on our data, we selected a 25% change and a 40% change in the physical function subscale to represent moderate and large MCIDs, respectively. 17 These changes are equivalent to five levels of improvement among the 10 questions, in any combination, for a moderate MCID, and eight levels of improvement for a large MCID.
Statistical analyses
The data are presented as means and SD for continuous variables, and frequencies with proportions for categorical variables. The normality assumption for continuous variables was checked based on Shapiro–Wilk tests. The p-values for multiple group comparison were obtained from the ANOVA/Wilcoxon/Kruskal–Wallis tests and Pearson’s chi-squared/Fisher’s exact tests for continuous and categorical variables, respectively, as appropriate (Table 1). The equality of variance for pairwise group comparison is evaluated based on F-tests. The magnitudes of meaningful changes were calculated based on a distributed-based method by using the effect size with the formula
Baseline clinical characteristics of each group, as previously described. 13
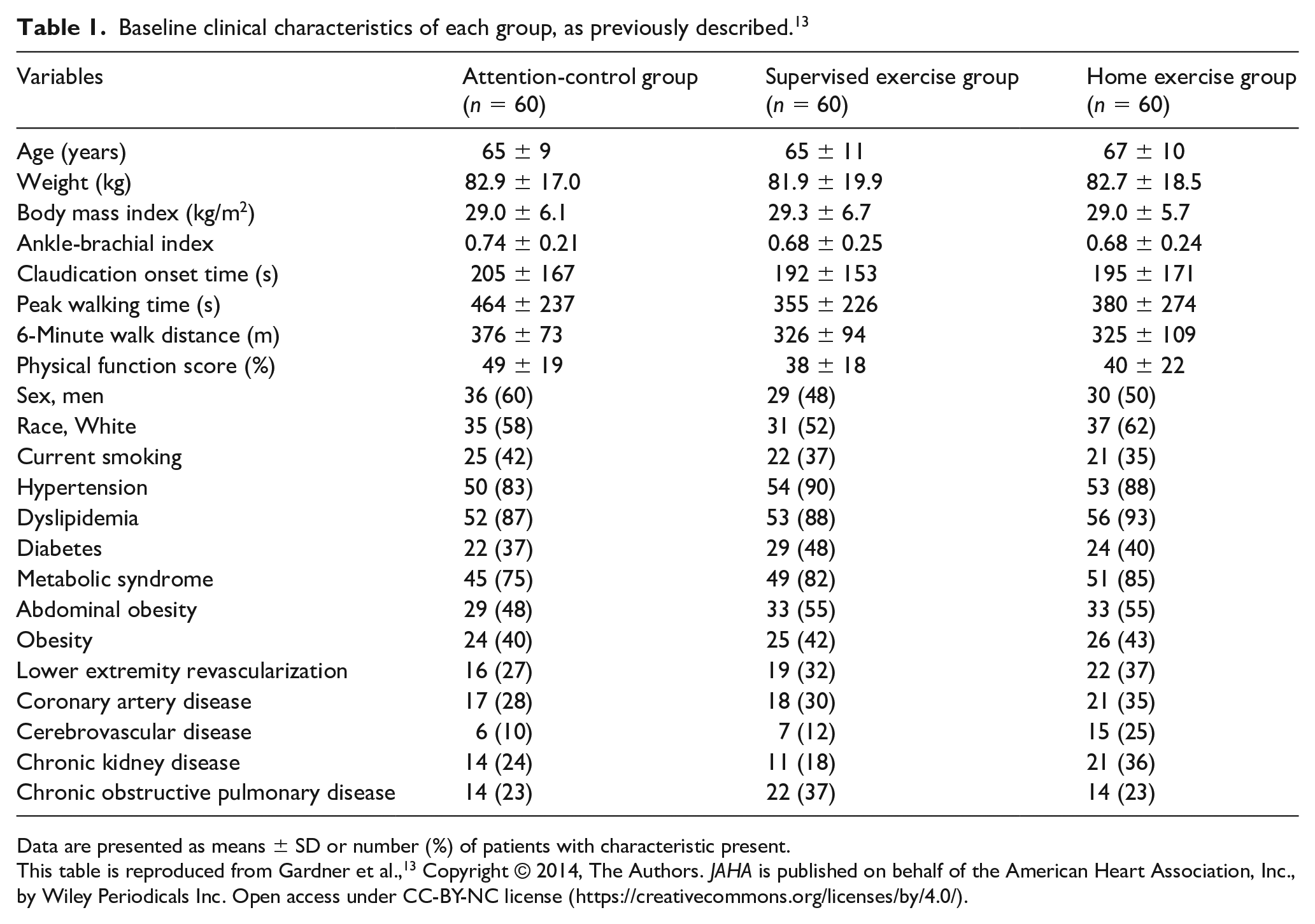
Data are presented as means ± SD or number (%) of patients with characteristic present.
This table is reproduced from Gardner et al., 13 Copyright © 2014, The Authors. JAHA is published on behalf of the American Heart Association, Inc., by Wiley Periodicals Inc. Open access under CC-BY-NC license (https://creativecommons.org/licenses/by/4.0/).
Results
The baseline clinical characteristics of the three groups are shown in Table 1. None of the baseline characteristics were significantly different among the groups. As described in the original investigation, 13 156 patients completed the trial and 24 did not.
The group change scores of physical activity and physical function variables following 3 months of intervention are shown in Table 2. A comparison among the three groups found that the change scores were significantly different for time spent in MVPA (p = 0.02), and maximum 30-minute cadence (p < 0.01). Within the home-based exercise group, significant increases in change scores were found for time spent in MVPA (p < 0.05), maximum 5-minute cadence (p < 0.05), maximum 30-minute cadence (p < 0.01), and the physical function subscale (p < 0.01). Within the supervised exercise group, significant increases in change scores were found for maximum 5-minute cadence (p < 0.05), and the physical function subscale (p < 0.01). Within the attention-control group, none of the change scores increased significantly (p > 0.05).
Group change scores of physical activity and physical function variables following 3 months of intervention.
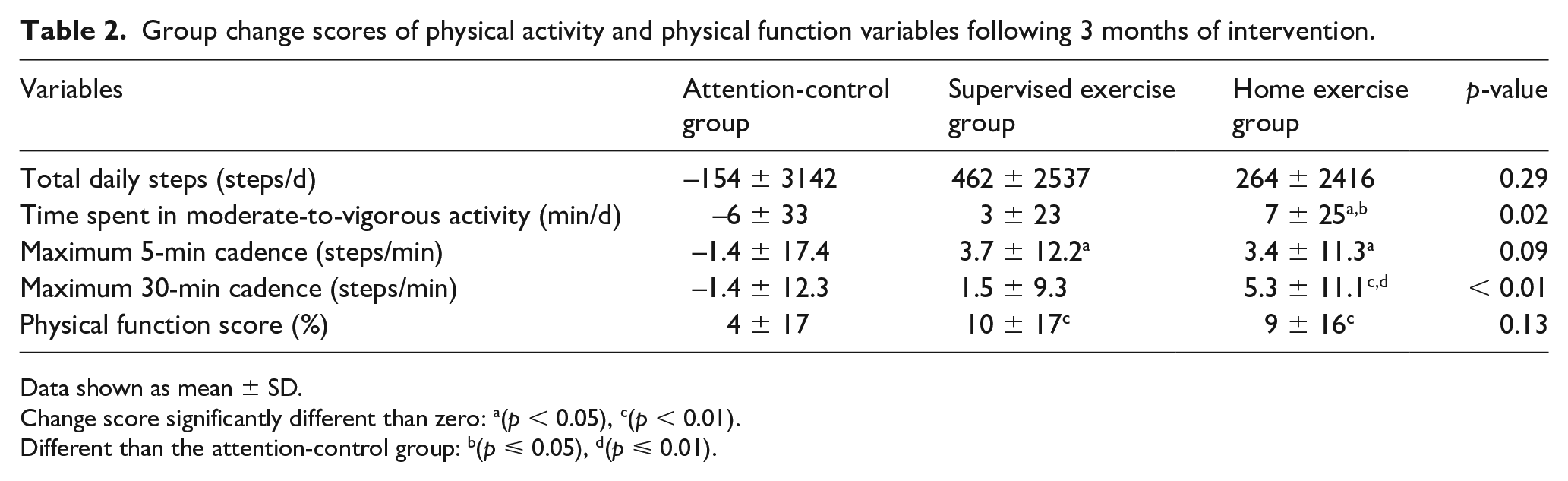
Data shown as mean ± SD.
Change score significantly different than zero: a(p < 0.05), c(p < 0.01).
Different than the attention-control group: b(p ⩽ 0.05), d(p ⩽ 0.01).
Based on effect size calculations, the distribution-based method to determine MCID for small, moderate, and large changes in physical activity variables following 3 months of intervention are shown in Table 3. The MCID for small, moderate, and large changes in total daily steps in the home-based exercise group were 558, 1396, and 2233 steps/d, respectively, and the corresponding changes in the time spent in MVPA were 6, 15, and 23 minutes. The respective MCID values for the maximum 5-minute cadence were 2.9, 7.3, and 11.7 steps/min, and for the maximum 30-minute cadence they were 2.3, 5.8, and 9.3 steps/min. Similar change score values were noted between the home-based and supervised exercise groups (Table 3).
Distribution-based method to calculate MCID for small, moderate, and large changes in physical activity variables following 3 months of intervention.
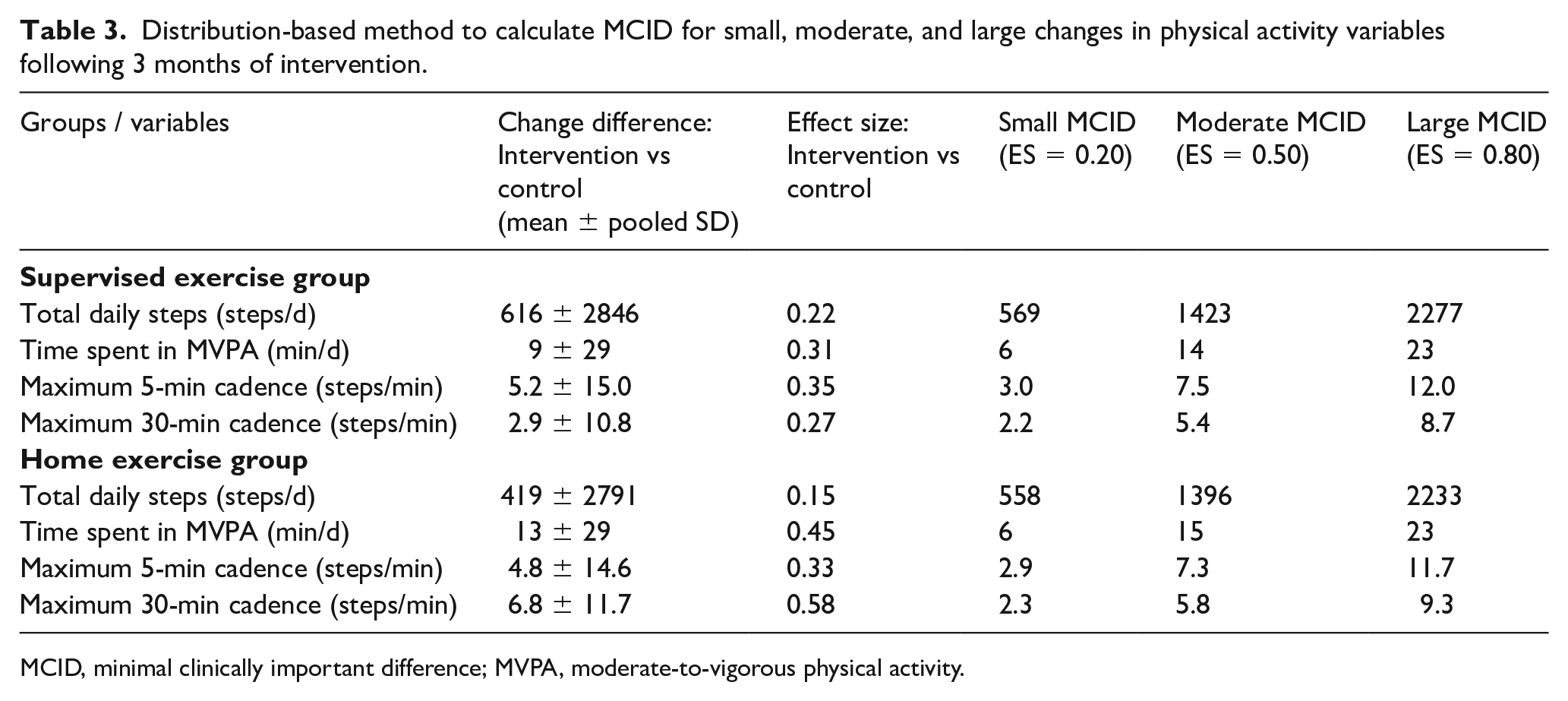
MCID, minimal clinically important difference; MVPA, moderate-to-vigorous physical activity.
The anchor-based method to calculate MCID for small, moderate, and large changes in physical activity variables following 3 months of exercise intervention is displayed in Table 4. To have a larger sample size for the anchor-based method, we pooled the patients from the supervised and home-based exercise groups to obtain more stable exercise estimates. The anchor-based MCID for small, moderate, and large changes in total daily steps following exercise intervention were 770, 784, and 1211 steps/d, respectively, and the corresponding changes in the time spent in MVPA were 4, 5, and 11 minutes. The respective anchor-based MCID values for the maximum 5-minute cadence were 0.9, 2.1, and 5.0 steps/min, and for the maximum 30-minute cadence they were −0.4, −0.3, and 4.7 steps/min. Thus, increases in maximum cadence for 5 and 30 continuous minutes need to approach 5 steps/min to translate to large anchor-based MCID values for changes in HRQoL, with changes below this level providing less reliable estimates of small and moderate MCID values.
Anchor-based method to calculate MCID for small, moderate, and large changes in physical activity variables following 3 months of exercise intervention.
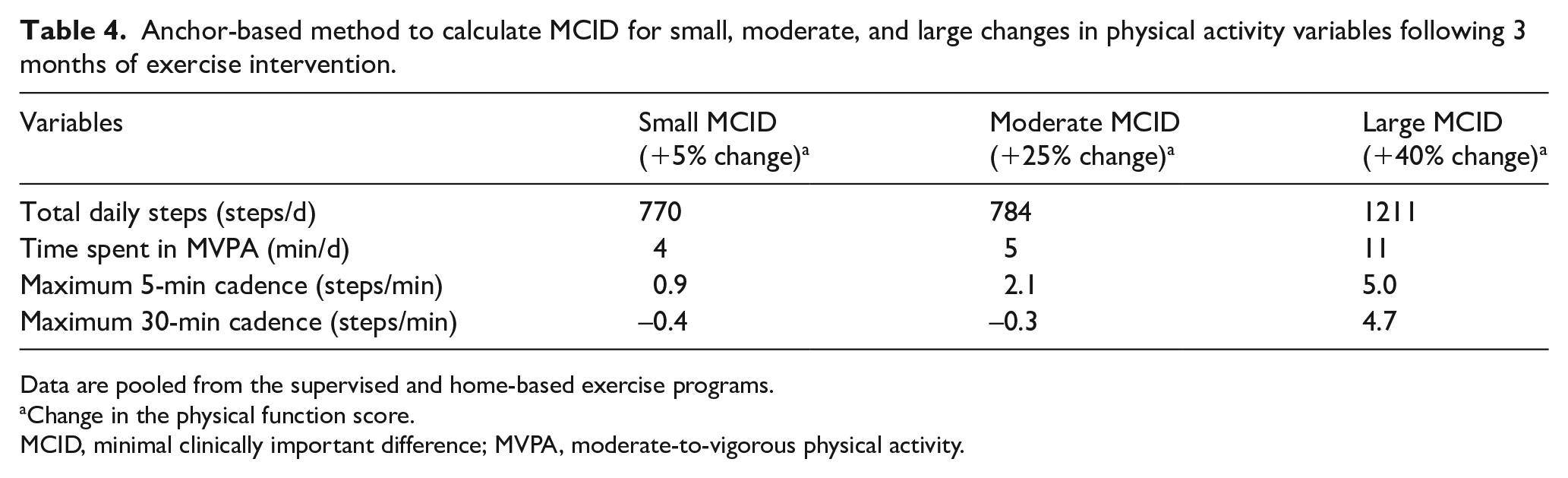
Data are pooled from the supervised and home-based exercise programs.
Change in the physical function score.
MCID, minimal clinically important difference; MVPA, moderate-to-vigorous physical activity.
The number of patients needed per exercise group to detect meaningful changes in a between-group comparison with the nonexercise control group with 80% power are shown in Table 5. The small, moderate, and large clinically meaningful changes in total daily steps in the home-based exercise group require group sample sizes of 498, 81, and 32 patients, respectively. For all of the outcomes in the home-based exercise group, a sample size between 28 and 36 patients was required for a large MCID change to be statistically significant, whereas a group sample size between 71 and 90 patients was required for a moderate MCID to be statistically significant. More than 400 patients per group were necessary for a small MCID in the daily step count variables to be statistically significant.
Patients needed per exercise group for 80% power in a between-group comparison with the nonexercise control group for 3 months of intervention.
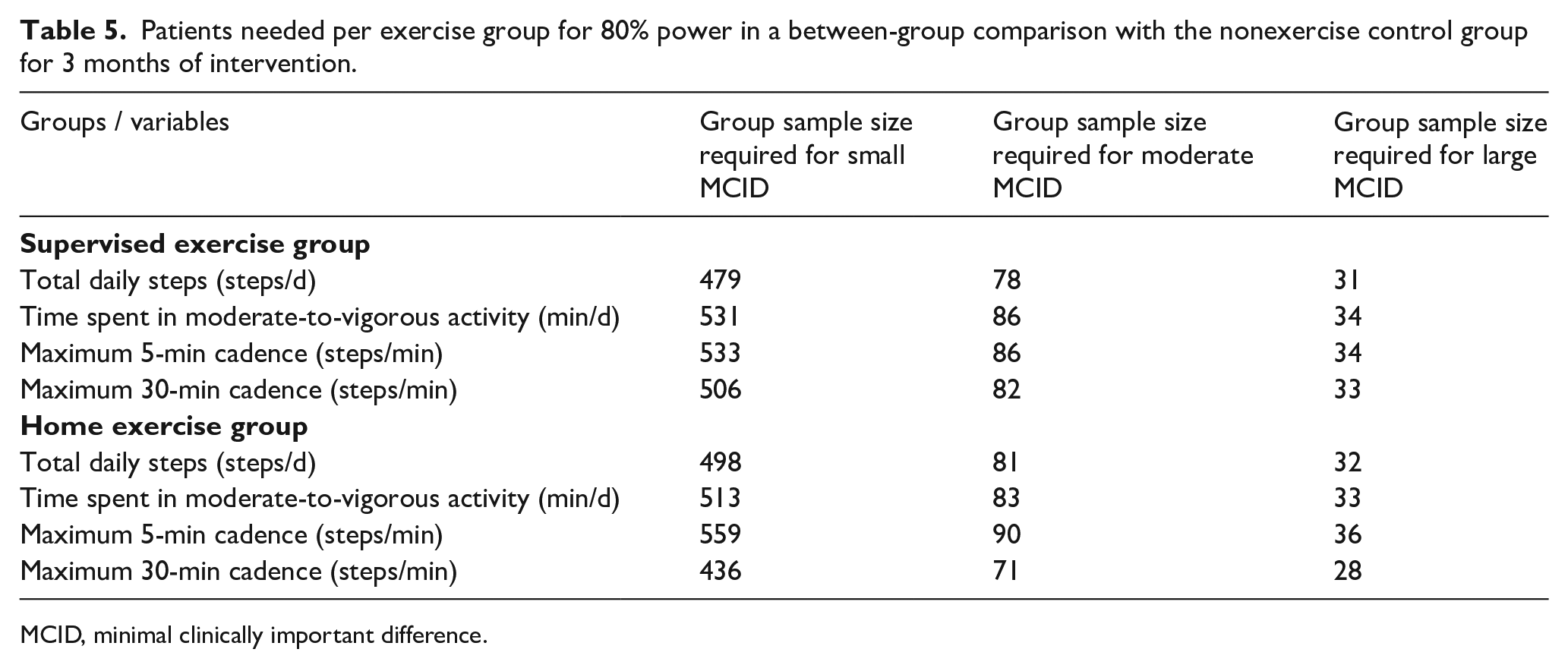
MCID, minimal clinically important difference.
Discussion
The primary novel finding was that following 3 months of home-based and supervised exercise programs for patients with PAD and claudication, an increase of 11 minutes in time spent in MVPA and an increase of 1211 total daily steps were associated with large anchor-based MCID increases in HRQoL. Given that the anchor-based MCID values are associated with changes in HRQoL, they may have the greatest clinical relevance for patients with PAD. Using the distribution-based method, the MCID values for small, moderate, and large changes following the home-based exercise program were 6, 15, and 23 minutes spent in MVPA, and 558, 1396, and 2233 total daily steps, respectively. Similar distribution-based MCID scores were noted for the supervised exercise group.
MCID for daily step counts and MVPA time
The issue of what constitutes a meaningful change in daily step count parameters following exercise interventions in patients with PAD and claudication is an important clinical research consideration. Community-based daily step counts and time spent in MVPA deserve attention as key metrics in defining the overall success of an exercise program because step counts and MVPA time indicate whether the well-described improvements in laboratory-based outcomes 11 obtained from a treadmill test and a 6-minute walk test translate to ambulatory improvements in a real-world setting. Additional clinical significance is placed on daily step counts and time spent in MVPA because they represent a health behavior associated with lower risk of all-cause and cardiovascular mortality, lower risk of cardiovascular diseases, improved physical function, and improved HRQoL in adults, 23 and has protective benefits for patients with PAD as well.37–40 Thus, measurement of daily step count and MVPA time change scores have clinical relevance from both the standpoint of serving as outcomes in a clinical trial, and serving as metrics of behavioral change that may improve the clinical course of patients with PAD.
A primary finding in this study was that an increase in MVPA of only 11 minutes each day was associated with a large anchor-based MCID increase in HRQoL. This change is important to appreciate because it is a relatively small increase in time that is feasible for patients with PAD to achieve, and because it is associated with a patient-based interpretation of improved HRQoL related to physical function. The increase in MVPA of 11 minutes each day was accomplished by walking at faster cadence in the community-based setting, which supports a recent study that found increases in walking speed of 0.05 and 0.15 m/sec over 10 meters in the laboratory corresponded to small and substantial MCID increases in patients with PAD. 41 Similar to the time spent in MVPA, an increase of 1211 total daily steps was associated with a large anchor-based MCID increase in HRQoL. This may be a more feasible goal for patients who are more severely diseased and functionally limited, as the total steps can be completed at a lower cadence (i.e., intensity) of walking. From a practical perspective, patients could achieve this daily step threshold by walking an additional 20 minutes each day at a relatively slow pace, which is associated with a patient-perceived large improvement in HRQoL. This supports our recent report that a modest amount of walking of more than 7000 steps each day is associated with greater ambulatory function and HRQoL in patients with PAD. 42 Furthermore, our current findings are in agreement with the few reports that exist on MCID determinations of daily physical activity outcomes, as several studies found MCID values to range between 350 and 1100 daily step counts for patients with chronic obstructive pulmonary disease.43–45 To our knowledge, the our current study is the only study to report MCID values on daily physical activity metrics besides step counts, such as time and steps spent in MVPA, and on daily cadences.
Our distribution-based results were congruent with the anchor-based findings. For time spent in MVPA, increases of 6 and 14–15 minutes each day following either home-based or supervised exercise programs were required to achieve small and moderate MCIDs, respectively. Thus, the large anchor-based threshold of 11 minutes each day is between the small and moderate distribution-based thresholds. In examining total daily steps, a similar pattern was noted for the distribution-based results. For example, increases of approximately 560 and 1400 total daily steps were required for small and moderate distribution-based MCIDs, respectively. Thus, the large anchor-based threshold of 1211 total daily steps is between the small and moderate distribution-based thresholds. Collectively, these results suggest that an effect size change following an exercise program between 0.20 (small) and 0.50 (moderate) is required to yield a large anchor-based MCID increase in HRQoL for both total daily steps and time spent in MVPA. This information may be particularly useful in designing future exercise trials to improve both daily step counts and HRQoL in patients with PAD.
MCID for daily cadences
In addition to the time spent in MVPA and the total daily steps, sustained ambulation at maximum cadence of various durations is an important metric to consider. We previously found that daily ambulatory cadences were positively associated with the gold-standard measurements of peak walking time and claudication onset time in patients with PAD and claudication, 31 indicating that higher sustained daily ambulatory cadences were associated with better claudication outcome measures. Our current study found that a large anchor-based MCID increase in HRQoL was associated with an increase in the daily maximum 5-minute and 30-minute cadences of 5.0 and 4.7 steps per minute. These large anchor-based thresholds in cadences are between the small and moderate distribution-based MCID thresholds. Given that the step length of PAD patients is approximately 2 feet, 46 our current findings related to cadence suggest that walking an additional 10 feet (3 meters) each minute for 5 and 30 consecutive minutes is associated with a large MCID in HRQoL. These findings suggest that the maximum ambulatory cadence that patients with claudication can maintain for up to 30 consecutive minutes in a free-living setting is a key metric that is related to HRQoL.
Study limitations
Although this study has determined MCID in common outcome measures for patients with PAD, several limitations exist. It is possible that there was a self-selection bias related to study participation, as patients were volunteers and may represent those with the highest interest in participating, the best access to transportation, and the best health compared to nonvolunteers. There is a limitation associated with our assessment of daily step counts, which does not measure other potential physical activities performed throughout the day, such as nonweight-bearing and nonambulatory activities. However, we believe this limitation is minimal because walking is required to complete many activities of daily living, and walking is the most common form of exercise for older adults. 21 Furthermore, the step activity monitor used in this study is considered the gold-standard to measure step counts, as it is the most accurate device available on the market. 47 Another limitation is that these results are only applicable to patients with PAD and claudication, and may not generalize to patients with different disease severity. A final limitation is that although patients were randomized into one of the groups prior to intervention, the possibility that those who participated in home exercise were more motivated than other patients cannot be ruled out. However, these results are generalizable to symptomatic patients with PAD who typically have high prevalence of comorbid conditions.
Conclusion
Following 3 months of home-based and supervised exercise programs for patients with PAD and claudication, increases of 11 minutes in time spent in MVPA and 1211 total daily steps were associated with large anchor-based MCID increases in HRQoL. The clinical implication is that patients with PAD and claudication should be encouraged to increase daily steps, particularly by walking an additional 11 minutes each day in MVPA, which is associated with a large meaningful increase in HRQoL.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by grants from the National Institute on Aging (R01-AG-24296) and General Clinical Research Center (M01-RR-14467) sponsored by the National Center for Research Resources.