
Abstract

Patients with peripheral artery disease exhibit limitations in performing physical activities. 1 In these patients, high sedentary time (ST) and/or low moderate-to-vigorous physical activity (MVPA) have been linked to adverse health outcomes. 2 However, the identification of patients with an unhealthy combined profile of ST/MVPA (i.e., co-occurrence of physical inactivity and elevated ST) remains challenging in clinical practice. Previous research has demonstrated that daily steps can be used to identify an unhealthy combined profile of ST/MVPA in older adults. 3 However, the proposed cut-off point may not be suitable for patients with peripheral artery disease and claudication symptoms. Herein, our aim was to establish specific cut-off points for distinguishing between healthy and unhealthy combined profiles of ST/MVPA among patients with peripheral artery disease and claudication symptoms.
This cross-sectional study recruited patients with peripheral artery disease (ankle–brachial index [ABI] ⩽ 0.90) with the practice of physical activity limited only by claudication symptoms at hospitals in Sao Paulo, Brazil. Patients were included according to the following criteria: (a) ⩾ 40 years old; (b) claudication symptoms in one or two legs; (c) absence of critical limb ischemia or rest pain; (d) absence of noncompressible vessels; (e) no amputated limbs and/or ulcers. This study was approved by the institutional ethics committee.
Patients’ characteristics were identified by clinician evaluation, medication use, and/or by medical record review. Body weight and height were measured, and body mass index was calculated. Peripheral artery disease severity was verified by the ABI as the highest systolic blood pressure in the posterior tibial or dorsalis pedis artery divided by the highest systolic blood pressure in the brachial artery in both limbs using a Doppler vascular monitor (Medmega DV160; Franca – SP, Brazil). The 6-minute walk test was performed using standardized procedures and the results were expressed in meters and relativized based on normative values of healthy individuals. 4
Daily steps, ST, and MVPA were assessed using the GT3X+ accelerometer (ActiGraph, Pensacola, FL, USA) for 7 consecutive days, following the standardized procedures. 5 The device was attached to an elastic belt and attached to the right side of the hip. Periods with consecutive values of zero for 60 minutes or longer were interpreted as ‘accelerometer not worn’ and excluded from the analysis. Physical activity data were included only if the participant had accumulated a minimum of 10 hours/day of recording for at least four days, including one weekend day. ST and MVPA were calculated using cut-off points for older adults (0–99 and ⩾ 1952 cpm, respectively). 6 Daily steps were calculated by the number of steps/day. Data analysis was adjusted for the time and number of days the device was worn. The combined profiles of ST/MVPA were defined as follows: (i) unhealthy: highest tertile of ST and lowest tertile of MVPA; (ii) healthy: lowest tertile of ST and highest tertile of MVPA. 3 The remaining combinations were classified as ‘neutral’.
Receiver operating characteristic (ROC) curves were constructed to assess the ability of daily steps to dintinguish patients with peripheral artery disease with healthy and unhealthy combined profiles of ST/MVPA. Cut-off points were obtained by minimizing the distance between points on the ROC curve and the upper left corner. Afterwards, the ABI and absolute and relative six-minute walk test distances were compared between the healthy, neutral, and unhealthy profiles using generalized linear models adjusted by age, time of diagnosis, ST, MVPA, diabetes, stroke, and use of vasodilator and antidiabetic medications. Data are presented as mean ± SD, or relative frequency, and p ⩽ 0.05 was accepted as significant.
ROC curve analysis showed that daily steps discriminated between patients with peripheral artery disease with healthy, neutral, and unhealthy combined profiles of ST/MVPA (Figure 1A and 1B). These findings support the use of daily steps as a clinically useful metric to discriminate between patients with peripheral artery disease with healthy and unhealthy combined profiles of ST/MVPA. The identified cut-off points derived from the ROC curves for healthy (⩾ 5700 steps/day) and unhealthy (⩽ 3137 steps/day) combined profiles of ST/MVPA were lower than those previously reported in older adults free of cardiovascular diseases (⩾ 7134 and ⩽ 5263 steps/day, respectively). 3 This difference may be attributed to the walking impairment of patients with peripheral artery disease and claudication symptoms, which is a major barrier to physical activity for them. 7
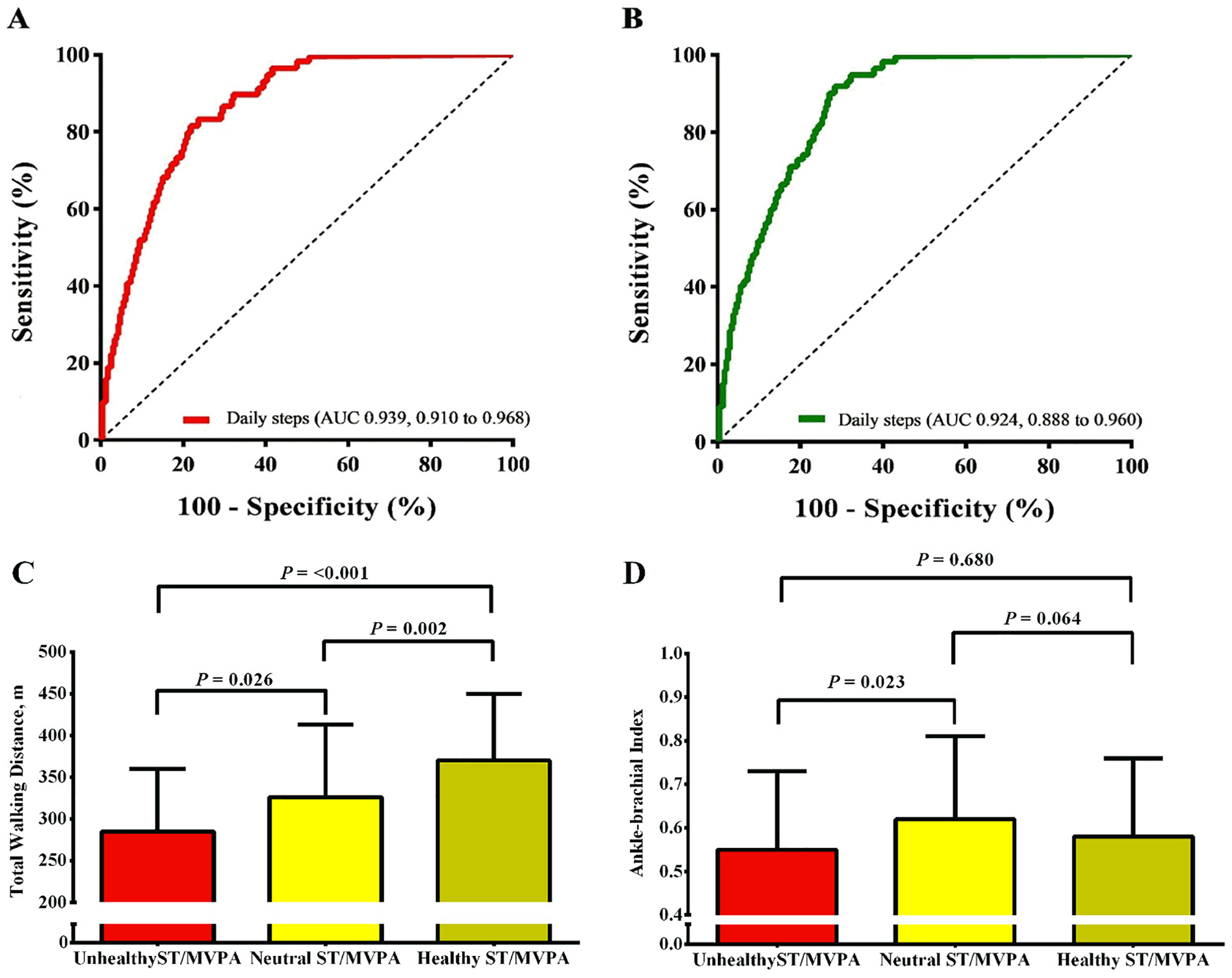
Receiver operating characteristic curve analysis using daily steps for identifying patients with peripheral artery disease with unhealthy
The patients’ characteristics according to combined profiles of ST/MVPA are included in online supplemental Table 1. Out of 233 patients (66 ± 9 years, 63% men, 27.4 ± 5.3 kg/m2, ABI 0.59 ± 0.19 [0.17; 0.89]), 66 patients were identified with healthy and 76 with unhealthy combined profiles of ST/MVPA, with the remaining 91 patients identified with a ‘neutral’ profile. Patients with an unhealthy profile were older compared to the neutral and healthy profiles (p < 0.05), and also had a longer time with the disease compared to those with a healthy profile (p < 0.05). Patients within the healthy profile spent more time in MVPA and less in ST compared to both the neutral and unhealthy profile groups. Overall, the ST/MVPA results are in accordance with previous data investigating physical activity and ST in patients with peripheral artery disease.8,9
Patients with a healthy combined profile of ST/MVPA had a greater relative (60 ± 25% healthy vs 46 ± 24% unhealthy; p = 0.004) six-minute walk test distance compared to the unhealthy profile, and greater absolute six-minute walk test distance compared to the neutral and unhealthy profiles (370 ± 80 m healthy vs 326 ± 87 m neutral vs 285 ± 75 m unhealthy; p < 0.05; Figure 1C). The ABI was higher in the neutral compared to the unhealthy profile (0.62 ± 0.19 neutral vs 0.55 ± 0.18 unhealthy, p = 0.023; Figure 1D). The six-minute walk test distance is strongly associated with mobility loss, adverse cardiovascular events, and mortality in patients with peripheral artery disease. 10 Patients with an unhealthy combined profile of ST/MVPA exhibited lower absolute and relative six-minute walk test distances, the latter considering sex, age, and body mass index when measuring walking distance. This demonstrates that the establishing of combined profiles of ST/MVPA seems to be more sensitive in detecting walking impairment in these patients. A previous study 11 has shown a positive association between MVPA and the six-minute walk test distance in patients with peripheral artery disease, and that reallocating 30 minutes per week from ST to MVPA was associated with a greater six-minute walk test distance, highlighting the beneficial effect of increasing MVPA in this population. On the other hand, the ABI, considered one of the best prognostic indexes in peripheral artery disease, has limited correlation with MVPA, 12 which aligns with the ABI values observed in our study.
A limitation that can be highlighted in this study is the use of a research-grade device instead of a commercially accessible one, which restricts its relevance in real-world settings, even though the accelerometer serves as the gold standard for physical activity and ST measurement and wearable devices are validated through accelerometer data.
In conclusion, our data derived from the receiver operating curves indicate that patients with peripheral artery disease who achieve ⩾ 6000 steps/day, which is an informative metric to facilitate clinician–patient communication, have the healthiest combined profile of ST/MVPA. Therefore, this number of steps could be a target for these patients. On the other hand, patients who take less than 3000 steps per day are highly likely to present an unhealthy combined profile of ST/MVPA, requiring closer and more tailored care. Based on previous evidence, 13 it is suggested that increasing daily step counts by ⩾ 1000 steps can provide health benefits and should be recommended for patients with an unhealthy combined profile of ST/MVPA. Considering the widespread availability of wearable technologies and smartphone apps that allow the assessment and monitoring of daily step counts, our findings have important and meaningful implications for various healthcare professionals in their daily practice, as any person in possession of a wearable device could monitor themselves and set step count goals in their daily lives.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231214476 – Supplemental material for Using daily steps to identify patients with peripheral artery disease with high sedentary time and low physical activity
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231214476 for Using daily steps to identify patients with peripheral artery disease with high sedentary time and low physical activity by Eduardo Caldas Costa, Gustavo Oliveira da Silva, Yuri A Freire, Hélcio Kanegusuku, Nelson Wolosker, Gabriel Grizzo Cucato, Marilia de Almeida Correia and Raphael Mendes Ritti-Dias in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Conselho Nacional de Desenvolvimento Cientifico e Tecnologico (CNPq) #409707/2016-3 and # 310508/2017-7, FAPESP #2016/16425-9, CAPES #01.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.