
Abstract
Keywords
Prevalence of peripheral artery disease (PAD) is similar, or higher, in women compared with men. 1 Although few studies exist investigating sex differences in PAD, women appear to be asymptomatic more often than men and, when symptomatic, present rest pain or atypical symptoms more often. 2 This may contribute to lower PAD detection and delayed therapeutic care initiation. 1 Moreover, women show a faster functional decline over time than men. 3 Differences have also been suggested regarding early outcomes following endovascular revascularization. 4 Optimal medical treatment is insufficiently prescribed in women. 1
Supervised exercise training (SET) is among first-line therapies in patients with symptomatic PAD. 5 However, PAD trials not only include an insufficient number of women but also lack sex-specific analyses. Additionally, the effectiveness of exercise training in women with PAD remains heterogeneous and needs to be clearly determined. Some studies showed that women have lower improvements in treadmill performance following SET compared to men, although contradictory results are reported.6,7
This study investigated the effect of SET on treadmill performance, functional performance, and quality of life in women and men with symptomatic PAD.
Fontaine stage II patients with chronic PAD and lower limb claudication participating in a SET program were included. The SET program is described in the online Supplement 1. The study was approved by the local ethics committee and was conducted according to the Declaration of Helsinki. All subjects provided written, voluntary, informed consent before participation.
Before and following SET, treadmill performance, functional performance, and quality of life were assessed. Pain-free (PFWD) and maximal (MWD) walking distance were assessed during a constant-load treadmill test. 5 Functional performance was assessed using the six-minute walking test, 5 short physical performance battery (SPPB), 8 and stair climbing test (SCT). 9 The quality of life was assessed using the Medical Outcomes Study Short-Form 36 (SF-36) questionnaire. 5 Self-perceived walking (dis)abilities were evaluated using the Walking Impairment Questionnaire (WIQ). 5
Owing to missing data, an intention-to-treat approach was used performing linear mixed models (LMMs). The influence of covariates (age and diabetes) was assessed a priori with simple linear regressions. When appropriate, these covariates were added to the models. When LMMs showed a significant interaction effect, significance was determined using multiple comparisons. To compare baseline characteristics between women and men we used t-tests and chi-squared tests.
Ninety-four patients (women: n = 30; men: n = 64) with chronic symptomatic PAD were included. Baseline characteristics were similar between groups (see online supplemental material).
Overall, 18 patients (women: n = 6 (20%); men: n = 12 (19%)) did not complete the SET program. The reasons were: endovascular revascularization during SET (women: n = 1 (3%); men: n = 3 (5%)), worsening of claudication symptoms (women: n = 2 (7%); men: n = 0 (0%)), schedule conflict with work (women: n = 1 (3%); men: n = 1 (2%)), feeling anxious about participating during the pandemic period (women: n = 1 (3%); men: n = 1 (2%)), and other reasons not related to SET (women: n = 1 (3%); men: n = 7 (11%)). The attendance rate of SET was 82% in both groups.
Treadmill performance significantly improved following SET in both women and men, with no significant difference between groups (Table 1). The six-minute walking distance (6MWD) and SPPB score were also significantly improved in both women and men, with no significant difference between groups (Table 1). The SCT performance was significantly improved in both groups, and changes were significantly greater in women than in men (Table 1). Physical component, WIQ distance, and stair climbing scores were significantly improved in women only, whereas mental component and WIQ speed scores were significantly improved in both women and men with no difference between groups (Table 1).
Treadmill performance, functional performance, and quality of life prior and after supervised exercise training in women and men with symptomatic chronic lower-extremity peripheral artery disease.
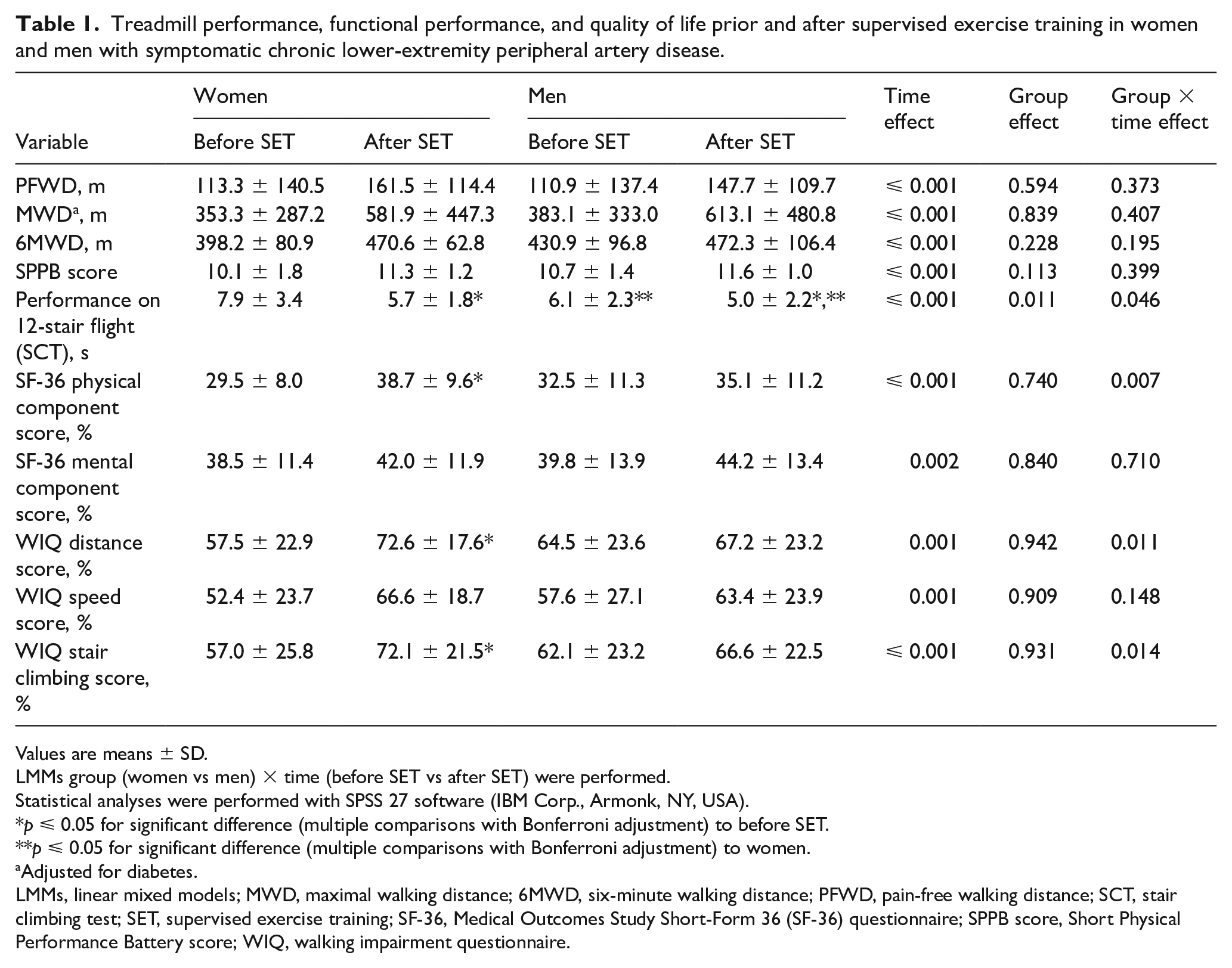
Values are means ± SD.
LMMs group (women vs men) × time (before SET vs after SET) were performed.
Statistical analyses were performed with SPSS 27 software (IBM Corp., Armonk, NY, USA).
p ⩽ 0.05 for significant difference (multiple comparisons with Bonferroni adjustment) to before SET.
p ⩽ 0.05 for significant difference (multiple comparisons with Bonferroni adjustment) to women.
Adjusted for diabetes.
LMMs, linear mixed models; MWD, maximal walking distance; 6MWD, six-minute walking distance; PFWD, pain-free walking distance; SCT, stair climbing test; SET, supervised exercise training; SF-36, Medical Outcomes Study Short-Form 36 (SF-36) questionnaire; SPPB score, Short Physical Performance Battery score; WIQ, walking impairment questionnaire.
The present study showed that symptomatic women with PAD, compared to men, similarly improved treadmill performances following SET. This is the first study showing that women similarly improved functional performance (6MWD, SCT, and SPPB) following SET compared to men. Previous studies have shown similar,7,10 or lesser,6,11 benefits in walking performance following SET in women compared to men. Moreover, the only study reporting generic (SF-36) and disease-specific (WIQ) quality of life showed that women improved less on WIQ scores during and following SET compared to men, whereas no differences were observed in generic quality of life. 6 In our study, physical component, WIQ distance, and WIQ stair climbing scores were significantly improved in women following SET. The discrepancies among studies may be related to different training protocols and patients’ baseline characteristics. Whether sex plays a significant role in the better improvement in self-reported quality of life and functional impairment observed in women still needs to be further investigated and likely mechanisms explained. This highlights the need for future research.
The first limitation of the study is its small sample size. Therefore, results may not be generalized. Second, men were more represented than women. Third, 20% of both women and men did not complete the SET program, leading to missing data during post-SET evaluation. This high rate of failure in both groups and the associated reasons are similar to previous observations. 12
These findings suggest that women with PAD should be highly recommended to participate in SET programs.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221149454 – Supplemental material for Sex-based differences in supervised exercise therapy outcomes for symptomatic peripheral artery disease
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221149454 for Sex-based differences in supervised exercise therapy outcomes for symptomatic peripheral artery disease by Stefano Lanzi, Anina Pousaz, Luca Calanca and Lucia Mazzolai in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.