
Abstract
Keywords
Introduction
Supervised exercise therapy (SET) is an important element of care for persons with peripheral artery disease (PAD) 1 for improving functional status, quality of life (QoL), and reducing leg symptoms.2,3 Currently, the gold standard exercise therapy used in SET involves intermittent treadmill walking training (TM) to moderate levels of claudication.1,3 However, TM is not feasible for some patients with PAD who enroll in SET due to foot ulcers, severe ischemia, gait instability, or other relative contraindications.1,4
Another mode of exercise training commonly utilized in cardiac rehabilitation settings is total body recumbent stepping exercise training (TBRS).5,6 TBRS is a seated, low-impact training modality, which has been shown to significantly increase walking performance, aerobic fitness, and lower body strength in healthy adults and stroke survivors.5,7 Furthermore, TBRS may offer a safe, alternative form of exercise for patients with PAD who cannot perform TM due to presence of relative contraindications.8 –10 Lastly, due the minimal ankle joint biomechanics inherent to TBRS, the calf muscles have minimal recruitment and oxygen requirements compared to that of walking. Therefore, for some (depending on site of arterial occlusion), TBRS may not produce claudication. As a result, TBRS has the potential to provide a higher dose of exercise in SET programs relative to traditional TM training.
In 2019, a scientific statement was published by the American Heart Association, which reviewed and summarized the state of the science related to exercise therapy in patients with PAD. 3 In this statement, the authors recommended that future research be directed to exploring alternative (nontreadmill or walking) modes of exercise for the rehabilitation of PAD. 3 In support of this scientific statement, the primary objective of this study was to compare the feasibility and safety of TBRS relative to gold-standard TM for treatment of symptomatic PAD in SET programs. The second objective was to evaluate the preliminary efficacy of TBRS on walking and physical function and PAD-specific QoL relative to TM. The final objective was to evaluate the effects of exercise dose on change in walking capacity (i.e., dose–response relationship).
Methods
Design
This pilot "Stepper Study" was a single-blind, randomized trial of participants newly enrolled in SET programs. SET programs were housed in five outpatient cardiac and pulmonary rehabilitation facilities of a Midwestern hospital system, all within 60 miles of the Twin Cities metropolitan area. 11 The study was approved by the University of Minnesota Institutional Review Board (IRB: #STUDY00006764), and all SET sites were covered by the University of Minnesota IRB. The Stepper Study used a two-parallel group design to randomize participants to TM or TBRS on a 1:1 allocation ratio, after providing written informed consent and completion of baseline data collection. An analyst, not involved in data collection or intervention delivery, generated a block randomization sequence in Excel to balance sample size across groups. Group assignment was predetermined using random allocation in blocks of five and 10, resulting in three blocks. The blocks were then randomized. The allocation table was uploaded to REDCap’s electronic data capture tools hosted at the University of Minnesota. User privileges for the randomization table were limited to the analyst who generated the randomization scheme.
Sample
All participants in the study were referred to SET by a physician responsible for their PAD treatment. All participants in the study had to meet the standards for inclusion based on Centers for Medicare & Medicaid Services (CMS) guidelines, 12 meaning that they had a diagnosis of PAD and had lifestyle-limiting claudication. Ankle–brachial index (ABI) criteria are not included in eligibility criteria in these guidelines 12 and therefore were not used as inclusionary/exclusionary criteria for the Stepper Study. In addition to CMS guidelines, 12 to be eligible for the Stepper Study, participants had to be committed to participate in a 12-week SET program, have the capacity to provide informed consent, and possess no relative contraindications to performing treadmill exercise. 1
Experimental protocol
SET program
The Stepper Study exercise prescriptions for TM and TBRS exercise mirrored the American Heart Association (AHA) guidelines for SET. 1 Based on CMS recommendations, patients were encouraged to complete a maximum of 36, 1-hour SET sessions over the course of 12 weeks. 12 All site cardiac rehabilitation and study staff were trained on the Stepper Study exercise protocol and exercise prescription. After completion of the baseline assessment, the first exercise session was supervised by study staff. Thereafter, cardiac rehabilitation staff supervised the exercise sessions, and study staff checked in with participants weekly and were available as needed for questions or monitoring. Additionally, all exercise logs were reviewed weekly by the primary investigator (PI) exercise physiologist to ensure exercise prescription compliance.
Treadmill group (TM)
Individuals in the TM group performed the exercise program at a self-paced speed while the incline was adjusted to induce moderate claudication (rated 3 to 4 on a scale of 0–5) within 5–10 minutes.1,4 Participants were then instructed to rest until pain subsided, at which point they began another walking bout at the same intensity. Exercise/rest cycles were repeated throughout each 60-minute exercise session. When a participant was able to walk for 10 minutes at the initial workload without having to stop because of moderately severe claudication, the treadmill speed or grade was increased by increments of 0.1 miles per hour (mph) or 1% in the subsequent training session based on participant preference.
Total body recumbent stepping group (TBRS)
TBRS was performed on the NuStep TRS 4000 T4 Recumbent Cross Trainer (NuStep, Ann Arbor, MI, USA) (Figure 1). Exercise prescriptions differed depending on whether the exercise training modality induced claudication.1,4 Participants were instructed to choose a comfortable pace (50–80 steps per minute [spm]) and a resistance that promoted ‘moderate’ effort. For participants who experienced claudication during TBRS, the exercise prescription mirrored that of the TM group and has been discussed previously. 1 For individuals who did not develop claudication during TBRS, TBRS exercise prescriptions were based on current cardiac rehabilitation guidelines to improve aerobic capacity.4,13
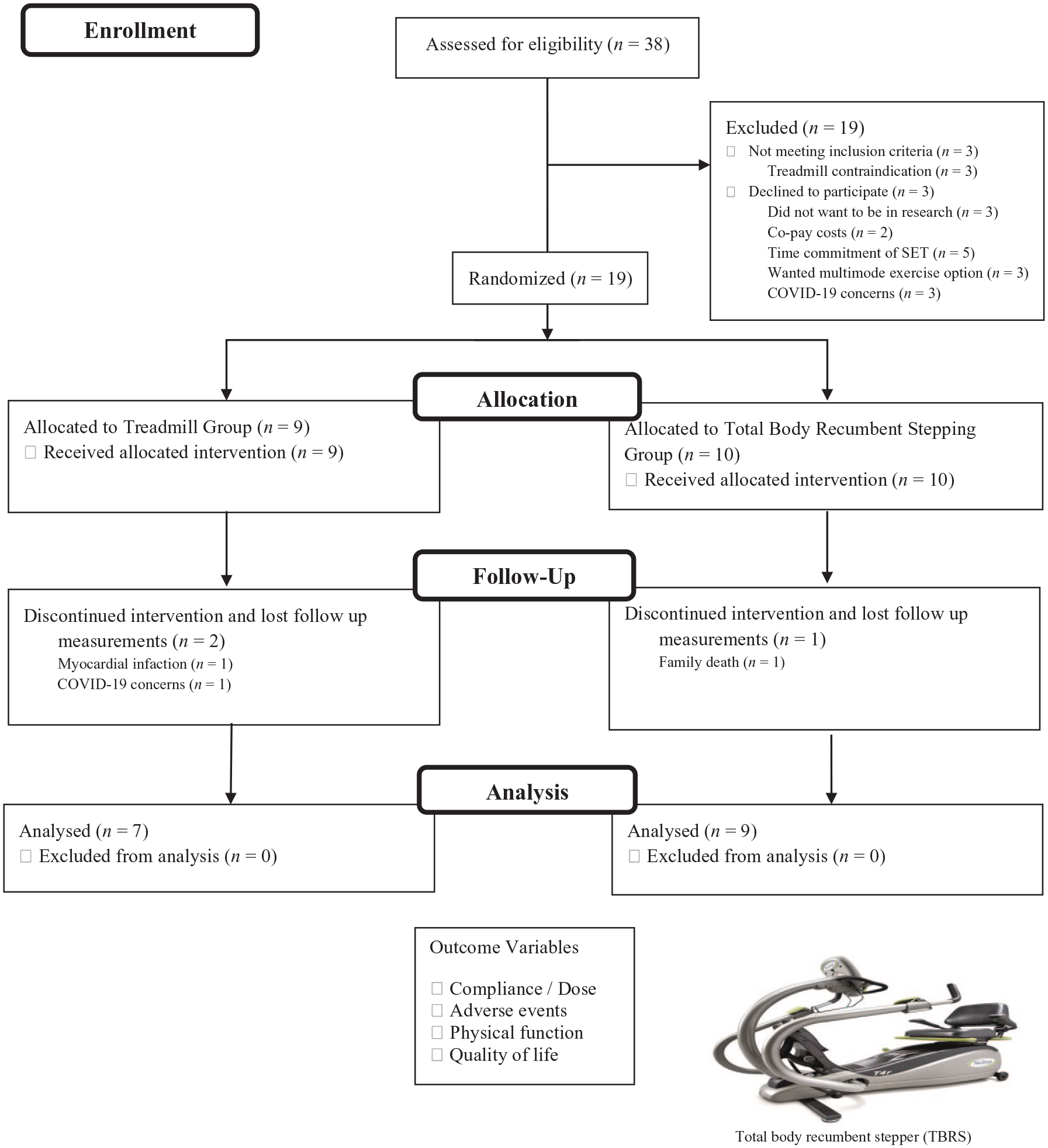
The Stepper Study participant flow diagram. Image of NuStep TRS 4000 T4 Recumbent Cross Trainer used with permission from NuStep (Ann Arbor, MI, USA)..
Outcome variables
Exercise compliance and dose
Attendance was recorded. Metabolic equivalents of task (MET) minutes were used to quantify dose of exercise accumulated over the course of the SET program. TM METS were estimated based on the speed and grade of walking recorded by staff during each exercise session. TBRS METs were calculated based on a regression equation from Dalleck and colleagues. 14 The MET value of each session was multiplied by the number of minutes exercised during the session and used to quantify session MET/min. Session MET/min were summed to quantify total dose.
Safety/adverse events (AE)
Data regarding nonstudy, study-related, and type of AEs were tracked throughout the study and used as a surrogate of safety-related outcomes. Nonstudy-related AEs were categorized as either ‘clearly not related to the study’ or ‘doubtfully related to the study’. Study-related AEs were categorized as an event ‘possibly’, ‘likely’, or ‘clearly’ related to the study. Further, type of AE (cardiac, limb, musculoskeletal, metabolic, or other) and incidence were recorded. Lastly, the severity of AE was categorized as (1) minor, (2) moderate, or (3) serious. All AEs were assessed and graded by study investigators. Study-related AEs per number of training hours were calculated for each group.
6-Minute walk test (6MWT)
The 6-minute walk test (6-MWT) was administered following standard guidelines. 15 Assistive devices were permitted, such as ankle braces, walkers, crutches, or canes. Participants were permitted to rest, with or without sitting, if necessary. Running or jogging was not permitted. Number of laps completed was quantified and used in the calculation of 6-minute walk distance, whereas the claudication onset distance (COD) was defined as the distance walked prior to the onset of claudication or ischemic limb symptoms. The 6MWT has been used extensively in cardiovascular research, including individuals with PAD, as a method of monitoring disease status and the effects of interventions. 16
4-Meter walk test (4mWT)
The 4-meter walk test (4mWT) was performed on a standard course with a starting line marked by a cone, a 4.0-meter finish line, and a 5.5-meter line (marked by a cone). The participant started one stride length behind the starting cone. Timing with a stopwatch began when the first foot passed the starting line and ended when the first foot passed the finish line.17,18 Participants were informed to walk to the second cone to ensure not slowing down before the finish line. Participants performed two trials with the time of both trials averaged. The 4mWT has been used extensively with older adults, including individuals with PAD, to evaluate functional status, disability, and risk of falling. 16
Repeated chair rise (RCR)
Participants were instructed to sit with their back against the back of a standard padded chair (43.20 cm) without armrests. Timing with a stopwatch began upon the participants’ initial upward movement and stopped when the patient achieved the seated position after the 5th repetition. Each repetition was said aloud so that the patient remained oriented. 17 The RCR test is a valid measurement of lower body strength in older adults. 19
Timed Up and Go test (TUG)
Participants were instructed to sit with their back against the back of a standard padded chair (43.20 cm) without armrests. Participants were instructed to stand up from a chair, walk 3 meters at their usual pace past a line on the floor, turn around, walk back to the chair, and sit down again with the back against the chair. 20 The TUG test is a valid test for assessment of dynamic balance and fall risk in older adults. 21
Peripheral Artery Disease Quality of Life (PADQOL) questionnaire
QoL was also assessed, using the PADQOL, a 38-item questionnaire designed to specifically examine PAD-related QoL. 22 The PADQOL contains five factors: social relationships and interactions, self-concept and feelings, symptoms and limitations in physical functioning, fear and uncertainty, and positive adaptation. Scores range from 0 to 100, with higher scores indicating better QoL.
Statistical analyses
All statistical analysis were performed using SPSS version 28.0 (IBM Corp, Armonk, NY, USA). The normality of data distribution and the homogeneity of variance were evaluated using Shapiro–Wilks and Levene’s tests, respectively. Baseline values and change scores for the 4mWT and TUG were log-transformed to normalize the distribution due to large positively skewed SDs. At baseline, group characteristics were compared by an analysis of variance (continuous variables) or chi-squared test (categorical variables). Independent samples t-tests were used to compare differences between groups regarding feasibility data, including attendance to SET and exercise dose. Differences between groups for walking and physical function and QoL outcomes were assessed by analysis of covariance (ANCOVA), adjusting for baseline values for each respective test. Relationship of SET attendance, program exercise dose (MET/min), and session exercise dose (MET/min/session) to change in 6-minute walk distance were assessed by Pearson’s correlation coefficient.
Results
The Stepper Study proposed to enroll 20 participants over the course of 14 months (September 2019 to November 2020), with a study end date of January 2021. However, due to the COVID-19 pandemic, recruitment of new participants was paused from April to September 2020. A total of 19 participants were enrolled in the study and 16 completed baseline and 12-week discharge measurements as part of SET, resulting in a sample comprising of seven patients in the TM group and nine patients in the TBRS group (Figure 1). There were three study-related attritions due to: (1) COVID-19 concerns, (2) myocardial infarction, and (3) family death.
Demographics
The sample (n = 19) was 100% non-Hispanic White, 32% female, mean age of 69.9 (11.3 years), and mean ABI 0.67 [0.18]). There were no significant differences in demographic or clinical variables (Table 1) or physical function at baseline between groups.
Baseline demographic and clinical characteristics of each group.
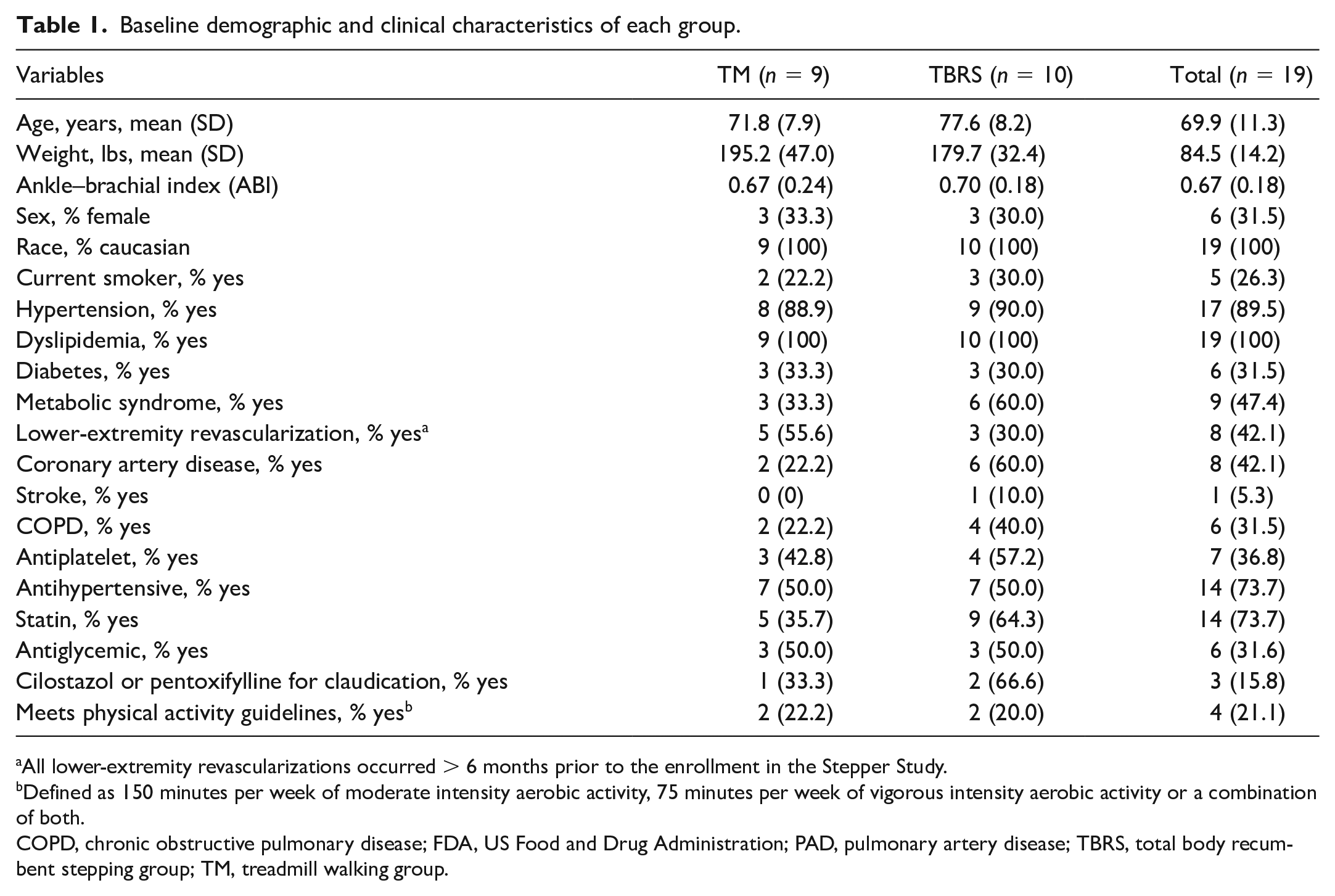
All lower-extremity revascularizations occurred > 6 months prior to the enrollment in the Stepper Study.
Defined as 150 minutes per week of moderate intensity aerobic activity, 75 minutes per week of vigorous intensity aerobic activity or a combination of both.
COPD, chronic obstructive pulmonary disease; FDA, US Food and Drug Administration; PAD, pulmonary artery disease; TBRS, total body recumbent stepping group; TM, treadmill walking group.
Exercise compliance and dose
The TBRS group attended 86% of the available 36 sessions over 12 weeks compared to 71% by the TM group (p = 0.07) (Table 2). Mean session dose of aerobic exercise was 144.7 [28.7] MET-min/session in the TBRS group compared to 117.6 [27.4] MET-min/session in the TM group (p = 0.08).
Supervised exercise therapy compliance and dose comparisons.
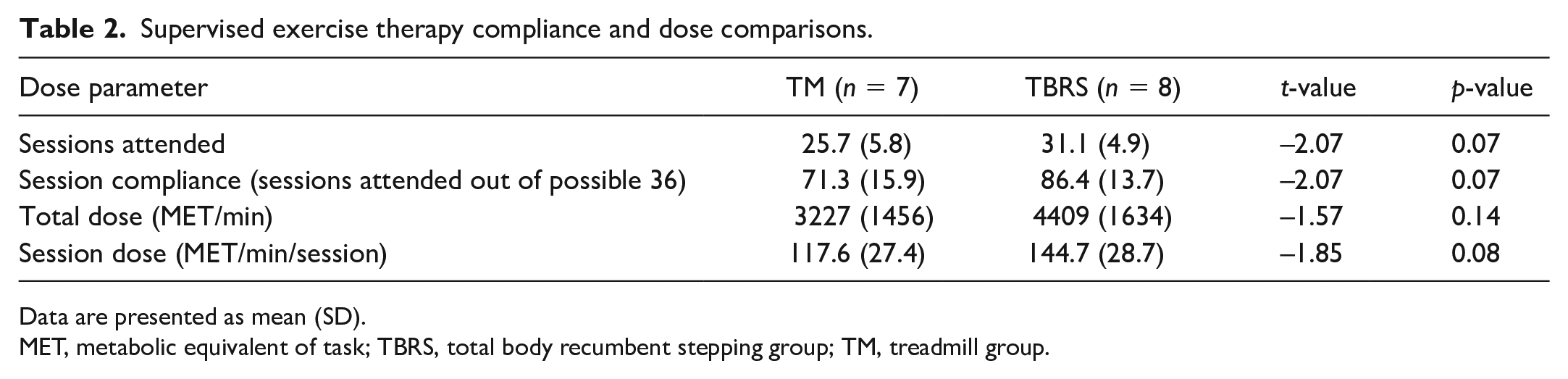
Data are presented as mean (SD).
MET, metabolic equivalent of task; TBRS, total body recumbent stepping group; TM, treadmill group.
Safety/AE
Overall, there were 12 minor, study-related (likely caused by intervention) AEs. Of these, nine (in 236 training hours) occurred in the TBRS group, and three (in 180 training hours) occurred in the TM group. A summary of ratings of individual AEs by group are summarized in the online supplementary material.
Physical function tests and PADQOL
Following SET, there were no significant differences in change scores for 6-minute walk distance (mean [SD]: TM: 133.2 [53.5] vs TBRS: 154.8 [49.8] ft; p = 0.77) after adjusting for baseline 6-minute walk distance. Likewise, there were no significant differences between the TM and TBRS groups regarding change scores for COD, 4mWT, RCR, and TUG after adjusting for baseline (Table 3). Lastly, there were no significant differences between groups for change in the five factors of the PADQOL (Table 3).
Effects of supervised exercise therapy on secondary outcomes.
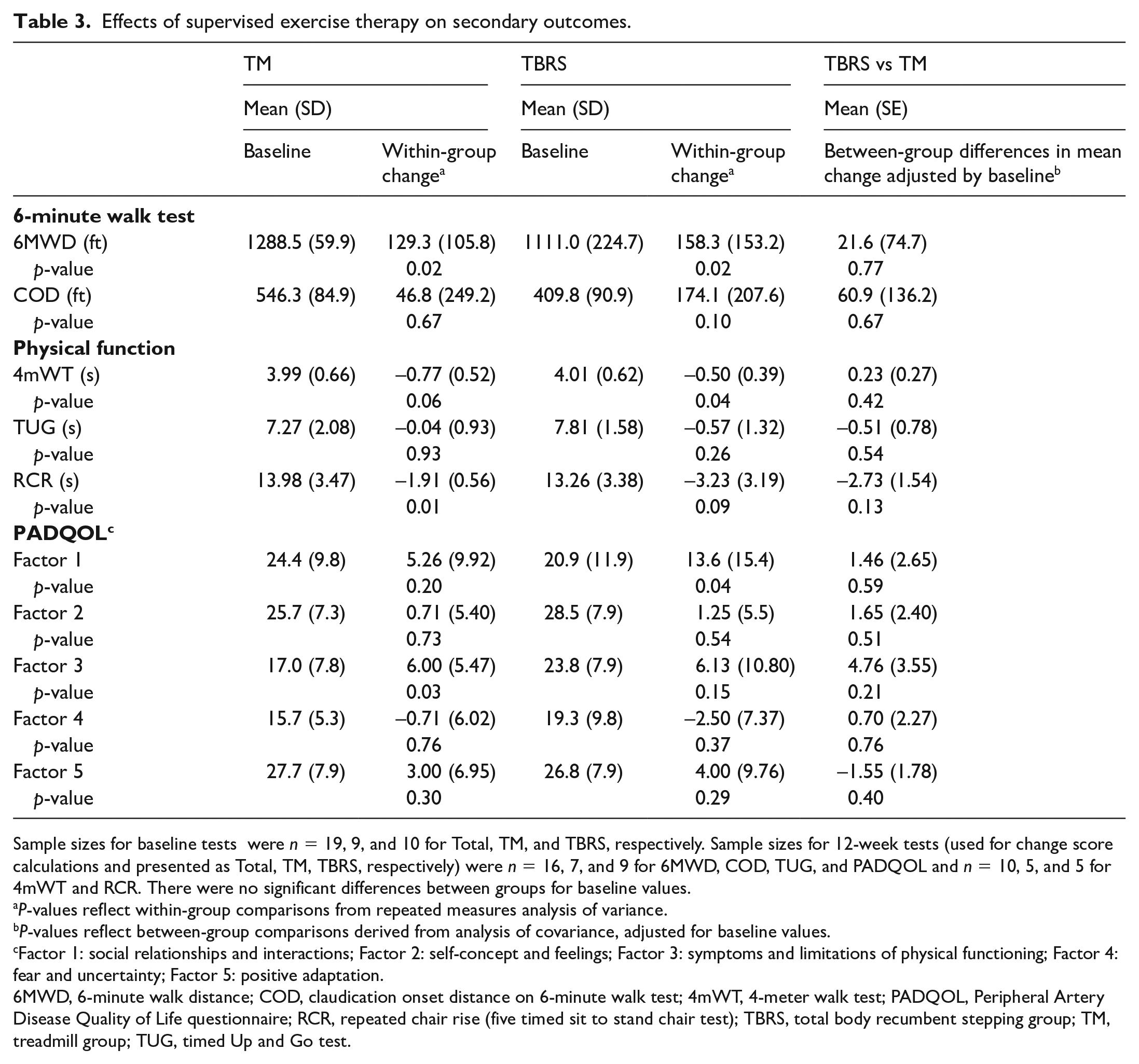
Sample sizes for baseline tests were n = 19, 9, and 10 for Total, TM, and TBRS, respectively. Sample sizes for 12-week tests (used for change score calculations and presented as Total, TM, TBRS, respectively) were n = 16, 7, and 9 for 6MWD, COD, TUG, and PADQOL and n = 10, 5, and 5 for 4mWT and RCR. There were no significant differences between groups for baseline values.
P-values reflect within-group comparisons from repeated measures analysis of variance.
P-values reflect between-group comparisons derived from analysis of covariance, adjusted for baseline values.
Factor 1: social relationships and interactions; Factor 2: self-concept and feelings; Factor 3: symptoms and limitations of physical functioning; Factor 4: fear and uncertainty; Factor 5: positive adaptation.
6MWD, 6-minute walk distance; COD, claudication onset distance on 6-minute walk test; 4mWT, 4-meter walk test; PADQOL, Peripheral Artery Disease Quality of Life questionnaire; RCR, repeated chair rise (five timed sit to stand chair test); TBRS, total body recumbent stepping group; TM, treadmill group; TUG, timed Up and Go test.
Dose–response
Number of sessions attended was moderately correlated to change in 6-minute walk distance in the entire sample (r = 0.63; n = 16; p = 0.01) and strongly correlated in the TBRS group (r = 0.87; n = 9; p < 0.01). Total dose (MET-min) was moderately correlated to change in 6-minute walk distance in the entire sample (r = 0.52; n = 16; p = 0.05) and specifically in the TM (r = 0.50; n = 7; p = 0.26) and TBRS groups (r = 0.54; n = 9; p = 0.17).
Discussion
The primary finding in this study was that TBRS was a feasible mode of exercise for SET participants. Specifically, the TBRS group attended 86% of total sessions compared to 71% seen in the TM group and the currently reported 45% in CMS-reimbursed SET programs. 23 The TBRS group was able to achieve high MET (i.e., intensity) and duration targets (40–50 minutes/session) (Table 2). Likewise, TBRS was well tolerated by SET participants, with nine study-related, minor AEs in 236 training hours. The higher intensity and dose of exercise experienced by the TBRS group may have contributed to some of the minor AEs experienced by three of the participants, such as hypertensive response (3×), hypoglycemia (3×), and residual knee soreness (3×) (online supplementary material). Therefore, exercise providers should be aware of these potential minor AEs, particularly in patients that can achieve moderate–vigorous intensity workloads for prolonged durations on the TBRS.
This study supports the previous findings that nonwalking-focused, aerobic exercise programs can improve walking capacity in persons with symptomatic PAD;24 –27 the TBRS group saw a 13% increase in 6-minute walk distance (p = 0.02). Again, there were no significant differences between groups for any walking and physical function and QoL outcomes after adjusting for baseline scores (Table 3), suggesting that improvements were comparable to TM. It should be noted that using dose as a covariate did not change these findings, specifically as it pertained to 6-minute walk distance. In this model, dose as a predictor of 6-minute walk distance change was nonsignificant (p = 0.10), and the estimated marginal means for change in 6-minute walk distance (mean [SD]) was 145.3 (53.2) feet for the TM group and 140.7 (49.4) feet for the TBRS group (p = 0.91).
Of importance, session attendance and total dose of exercise were moderately correlated with improvements in 6-minute walk distance. We believe that this is the first study that has demonstrated a dose–response using the 6-minute walk distance in CMS-SET programs. This finding provides evidence for exercise providers when educating their patients on the importance of both session attendance and compliance to the intensity and duration targets for improving walking capacity. Interestingly, in the TM group, session dose (MET-min/session) was moderately correlated (r = 0.52) to change in 6-minute walk distance. This preliminary finding suggests that persons who achieve a low dose of treadmill walking due to either a reduced intensity or walking duration may not see desired improvements in their walking capacity. This is an important consideration when evaluating patient progress, particularly early in the SET program. However, due to the small sample, this finding should be tested in future studies. Finally, given the important goals of secondary prevention of cardiovascular disease (CVD) events and management of CVD risk factors in the management of PAD, 2 achieving a high dose of exercise should be encouraged, given the well-known dose–response relationship regarding peak oxygen consumption 28 (i.e., the biggest predictor of CVD-related morbidity and mortality 29 ) and CVD risk factors.30,31
The primary strength of this study was that it employed current state-of-the-science exercise prescriptions and outcome measurements that are used by CMS-reimbursed SET programs across the country, 1 and thus help translate science into practice. Second, the setting of this study has had an abundance of collaborative experiences in exercise rehabilitation of PAD with the study investigators, dating before the start of CMS-reimbursed SET programs. This was vital in ensuring high treatment fidelity of the study participants.
Study limitations
Since this was a pilot study, sample size was an inherent study limitation. A lack of a true control group may be perceived as a study limitation. Lack of ethnic diversity in the sample limits the generalizability of the findings. It should be mentioned that enrollees in CMS-SET programs have been overwhelmingly non-Hispanic White, 23 and more efforts need to be undertaken to increase SET referrals and participation in ethnic groups who are at higher risk for PAD. Additionally, SET therapists instructed their participants to increase their physical activity outside of SET sessions. Upon arrival for each session, participants were instructed to recall their non-SET exercise participation. However, participants expressed difficulty quantifying their physical activity and it was not monitored objectively via accelerometry; therefore, inability to account for outside exercise or physical activity was a study limitation. Additionally, as intended, dose was not controlled (i.e., there was no iso-caloric match between exercise modalities), as the researchers wished for the protocols to mimic the current SET exercise recommendations. 1 However, we provided dose–adjusted statistical analyses for 6-minute walk distance. Finally, this study was initiated prior to, but finished during the COVID-19 outbreak, which affected enrollment and some data collection. Physical function measurements including the 4mWT and RCR tests (not part of the hospital-based SET evaluation and discharge) were additional measurements gathered by study research assistants. Owing to restrictions for in-person interactions with study participants that were administered by the university, 12-week tests for the RCR and 4mWT were missed in some participants, which accounts for the lower sample of these outcome measurements.
Conclusion
This is the first randomized study comparing TBRS to TM exercise in SET for patients with PAD using current guidelines. This study showed that TBRS is a safe and feasible exercise option for SET to improve walking and physical functioning, with the potential to provide a high dose of exercise. Although limited by sample size, this study provides preliminary efficacy of the use of the TBRS exercise modality in SET programs following current guidelines. Future, larger sample studies should be implemented to confirm these findings.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X211068888 – Supplemental material for Total body recumbent stepping vs treadmill walking in supervised exercise therapy: A pilot study
Supplemental material, sj-docx-1-vmj-10.1177_1358863X211068888 for Total body recumbent stepping vs treadmill walking in supervised exercise therapy: A pilot study by Dereck L Salisbury, Kari Swanson, Rebecca JL Brown and Diane Treat-Jacobson in Vascular Medicine
Footnotes
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was funded by the University of Minnesota via the Grant-in-Aid of Research, Artistry, and Scholarship Award (no. 323844).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.