
Abstract
Background:
Supervised exercise therapy (SET) is the cornerstone of medical therapy for symptomatic peripheral artery disease (PAD). Despite the efficacy of SET, initial reports following the 2017 Centers for Medicare and Medicaid Services (CMS) reimbursement decision indicate low SET uptake, referral, and completion. Vascular medicine specialists are key to the success of such programs. We examined rates of SET referral, completion, and outcomes in a health system with a robust SET program during the first 5 years of CMS reimbursement.
Methods:
A retrospective chart review of patients with PAD referred to SET between October 1, 2017 and December 31, 2022 was conducted. Patient demographic and medical characteristics, SET indication, referring provider specialty, SET participation (e.g., exercise modality, number of sessions, treadmill prescription), and outcomes were abstracted. Descriptive statistics, t-tests, and multiple linear regression were used to examine the sample, evaluate outcomes, and explore outcomes by relevant covariates (i.e., age, sex, referring provider specialty).
Results:
Of 5320 patients with PAD, N = 773 were referred to SET; N = 415 enrolled and were included in the present study. Vascular medicine and vascular surgery specialists were the two primary sources of referrals (30.6% and 51.6%, respectively). A total of 207 patients (49.9%) completed SET. Statistically significant and clinically meaningful improvements were observed in all outcomes.
Conclusion:
SET referral and completion rates are low in the 5 years following CMS reimbursement, despite the advocacy of vascular medicine specialists. SET is effective in improving patient functional capacity and quality of life. Additional efforts are needed to increase both SET availability and referrals as part of comprehensive treatment of PAD.
Keywords
Background
Current guidelines recommend the use of supervised exercise therapy (SET) to improve functional status and quality of life in people with symptomatic peripheral artery disease (PAD). 1 The Centers for Medicare and Medicaid Services (CMS) has reimbursed the cost of SET for beneficiaries with symptomatic PAD since May 2017. 2 Vascular medicine specialists were instrumental in the CMS decision to reimburse SET and play a key role in the uptake and success of such programs. Yet, despite a Class IA endorsement, 1 initial reports indicate low utilization and completion of SET. In an analysis by Divakaran and colleagues using data from the first 19 months of CMS reimbursement, only 1.3% of patients with claudication during the study period were enrolled in SET, with only 5.1% of those patients completing 12 weeks of SET. 3 Notably, the majority of patients enrolled in SET were in the Midwest region, comprising 48.1% of enrolled patients.
In comparison to other clinical exercise programs, such as cardiac rehabilitation and pulmonary rehabilitation, the effectiveness of SET is understudied. Preliminary evidence from clinical SET programs implemented prior to CMS reimbursement supports the effectiveness of SET,4,5 but the low uptake of SET has made similar analyses of CMS-reimbursed programs challenging. To further expand the evidence supporting the value of these programs and the importance of vascular medicine specialists who promote these programs as part of comprehensive care of patients with PAD, studies of referrals to and outcomes of robust clinical programs are needed.
SET for the treatment of symptomatic PAD has been available in the Twin Cities metropolitan area since approximately 2013. 6 As a result, these clinical sites are uniquely positioned to expand our understanding of the role of vascular medicine specialists in SET referral and uptake, as well as guide the establishment of benchmarks for SET-associated improvements in PAD symptoms to inform the development of high-quality SET programs in other regions. Herein we report the results of a retrospective study designed to address these gaps. Specifically, we sought to: (1) characterize rates and sources of referral to SET; (2) characterize patients who enrolled in and successfully completed SET; and (3) evaluate changes in physical function and quality of life following participation in SET.
Methods
The SET Registry and present study were reviewed and approved by the University of Minnesota institutional review board (STUDY00018920 and STUDY00019500, respectively). Only patients who did not ‘opt out’ of the use of their medical records for research purposes were included in the registry.
Design and setting
We conducted a retrospective study using a combination of medical record review and informatics services to obtain data on patients who completed a SET intake visit in the M Health Fairview system between October 1, 2017 and December 31, 2022. SET was provided through seven hospital-based cardiac and pulmonary rehabilitation programs in the health system, all within 60 miles of the Twin Cities metropolitan area.
The M Health Fairview system has had SET available to patients with PAD outside of clinical research studies since approximately 2013, initially through the hybrid phase III cardiac rehabilitation Wellness and Exercise for Life program and since October 2017 as a standalone, CMS-reimbursed SET program. Vascular medicine specialists within both vascular medicine and cardiology spearheaded the initial development and implementation of SET within the M Health Fairview system, prior to the CMS determination. This was instrumental in developing the infrastructure required for a successful launch of the CMS-reimbursed SET program. Soon after the CMS reimbursement decision, medical and rehabilitation center staff distributed information about the program to vascular medicine, vascular surgery, and primary care providers to facilitate referrals. In 2022, an outreach coordinator traveled to individual sites within the health system to further discuss program availability and outcomes with primary care providers.
SET structure and outcomes
SET in the M Health Fairview system consists of 12 weeks of up to 36 sessions of exercise training. SET in this setting has been previously described.5–7 Briefly, patients completed two to three SET sessions per week for 12 weeks consisting primarily of repeated bouts of treadmill walking exercise. Sessions followed an established protocol for patients with PAD 8 and were aligned with CMS requirements, 9 but were individualized according to patient needs and preferences.
During the initial evaluation, patients complete a medical history review, establish goals related to PAD and physical function, and complete assessments of baseline functional status. Patients then undergo treadmill familiarization and work with an exercise specialist to identify an initial treadmill grade and speed (treadmill prescription). After establishing an initial intensity, exercise intensity was gradually increased over 12 weeks. Although treadmill walking is the primary mode of exercise, total body recumbent stepping, cycling, upper body ergometry, and over-ground walking were integrated into the treatment plan depending on patient walking ability and therapy goals developed in collaboration with the exercise specialists. 6 For the SET Registry, patients were classified as using combination therapy if they used two or more exercise modalities in greater than or equal to two-thirds of sessions.
Evaluation of physical function and quality of life is performed at the patient’s initial evaluation and the time of discharge. Assessments include the 6-minute walk test, timed up and go test, and the Vascular Quality of Life Questionnaire-6.
6-Minute walk test (6MWT)
The 6MWT is a common performance-based functional measure in patients with PAD. 8 During the 6MWT, patients were instructed to walk as far as possible in 6 minutes. 10 The total distance walked in 6 minutes and the distance and time to claudication onset were recorded. Minimal clinically important differences following SET have been established for pain-free walking distance (24 meters) and total walking distance (12 meters). 11
Timed up and go (TUG) test
The TUG is used to evaluate functional mobility in older adults 12 by assessing the time in seconds required for the patient to rise from a chair, walk 3 meters (approximately 10 feet), turn around, walk back to the chair, and sit down.
Vascular Quality of Life Questionnaire-6 (VascuQoL-6)
The VascuQoL-6 is a six-item measure designed to assess health-related quality of life in patients with PAD. 13 Total scores range from 6 to 24 and an increase of 2.0 to 3.8 points has been proposed as a clinically meaningful improvement in patients with claudication undergoing SET. 14
Treadmill metabolic equivalent of task (MET)
For patients who completed a treadmill only or combination (treadmill + nontreadmill) program, treadmill MET change was computed. METs are commonly used as a performance measure of functional capacity in cardiac rehabilitation programs. 15 Treadmill METs were calculated using treadmill grade and speed. As the first two to three exercise sessions typically involve individualization of the appropriate workload for each patient, the initial treadmill METs were calculated using an average of the first and second or second and third sessions based on when exercise logs revealed that walking bouts were in the targeted time length (5–10 minutes) and claudication levels (mild/moderate: 2–3/4). 6 Because the last SET session is often the discharge appointment and patients may not have time to participate in a structured exercise session, treadmill METs at discharge were calculated using an average of the third to last and second to last sessions.
Data source
University of Minnesota Best Practices Integrated Informatics Core (BPIC)
Records of patients aged 18 or older referred to SET (CPT code 93668) from 2017 through 2022 were obtained. BPIC services were used to identify patients and extract the following data: age, sex, height, weight, race/ethnicity, smoking status, presence of comorbid conditions, ankle–brachial index (ABI), SET referring provider specialty, indication for SET referral, and the date of initial SET evaluation.
Referring providers were grouped into four specialty categories at the time of the referral for SET: (1) cardiology; (2) vascular medicine; (3) vascular surgery; and (4) other (family medicine, geriatric medicine, primary care, and students). For each patient/order, the referring provider’s affiliated specialties were identified. In most cases, providers had two to three specialties recorded. Providers with multiple specialties were categorized based on known area of practice, the combination of departments/specialties documented on the referral, and faculty biographies published on the health system website. For example, providers with ‘cardiovascular disease,’ ‘interventional cardiology,’ and ‘internal medicine’ specialties were included in the ‘cardiology’ category. Similarly, providers with ‘internal medicine’ and ‘cardiovascular disease’ specialties were included in the ‘vascular medicine’ specialty.
Chart review
Details of individual SET sessions are integrated into the medical record via scanned paper logs. Patient records were reviewed for manual abstraction of the details of SET participation, including number of sessions attended, completion status, reason(s) for early discontinuation, initial and discharge treadmill prescriptions, mode of exercise, and outcomes of SET (6MWT distances, TUG time, and VascuQoL-6 scores). Data were abstracted by three authors (MOW, PM, DLS) into a customized Research Electronic Data Capture (REDCap) data collection form. 16
Data analysis
The normality of data distribution and the homogeneity of variance were examined using the Shapiro–Wilk and Levene tests, respectively. SET referral rates, source of referrals, and cohort characteristics were described using mean (SD) and n (percent), as appropriate. Paired t-tests were used to examine differences between baseline and follow-up in outcome variables. One-way analysis of variance (ANOVA) or analysis of covariance (ANCOVA) were used to compare baseline characteristics and improvements following SET by participant groups (e.g., sex, age, smoking status, referral source, adherence to SET, baseline function). Analyses were performed in IBM SPSS Statistics (version 28; IBM Corp., Armonk, NY, USA); p < 0.05 was considered statistically significant.
Results
Of 5320 patients with PAD, a total of 773 patients had the SET CPT code during the reference period. Figure 1 provides a flowchart describing the numbers of patients diagnosed with PAD, referrals to SET, enrollment in SET, discontinuation (with reasons), and completion of SET. Referral rate to SET (percentage of those with a diagnosis of PAD who received a referral to SET) and uptake into SET (percentage of referrals who completed a SET evaluation) were 14.5% and 56.4%, respectively. Apart from 2020, an average of 87 intakes were completed yearly (range 84–92). Among those who were referred to and completed a SET intake visit, N = 415 (95%) were included in the study. Common reasons for SET discontinuation were medical conditions (n = 39) and copay or financial concerns (n = 13), but most reasons for discontinuation were unknown or not recorded (n = 108).
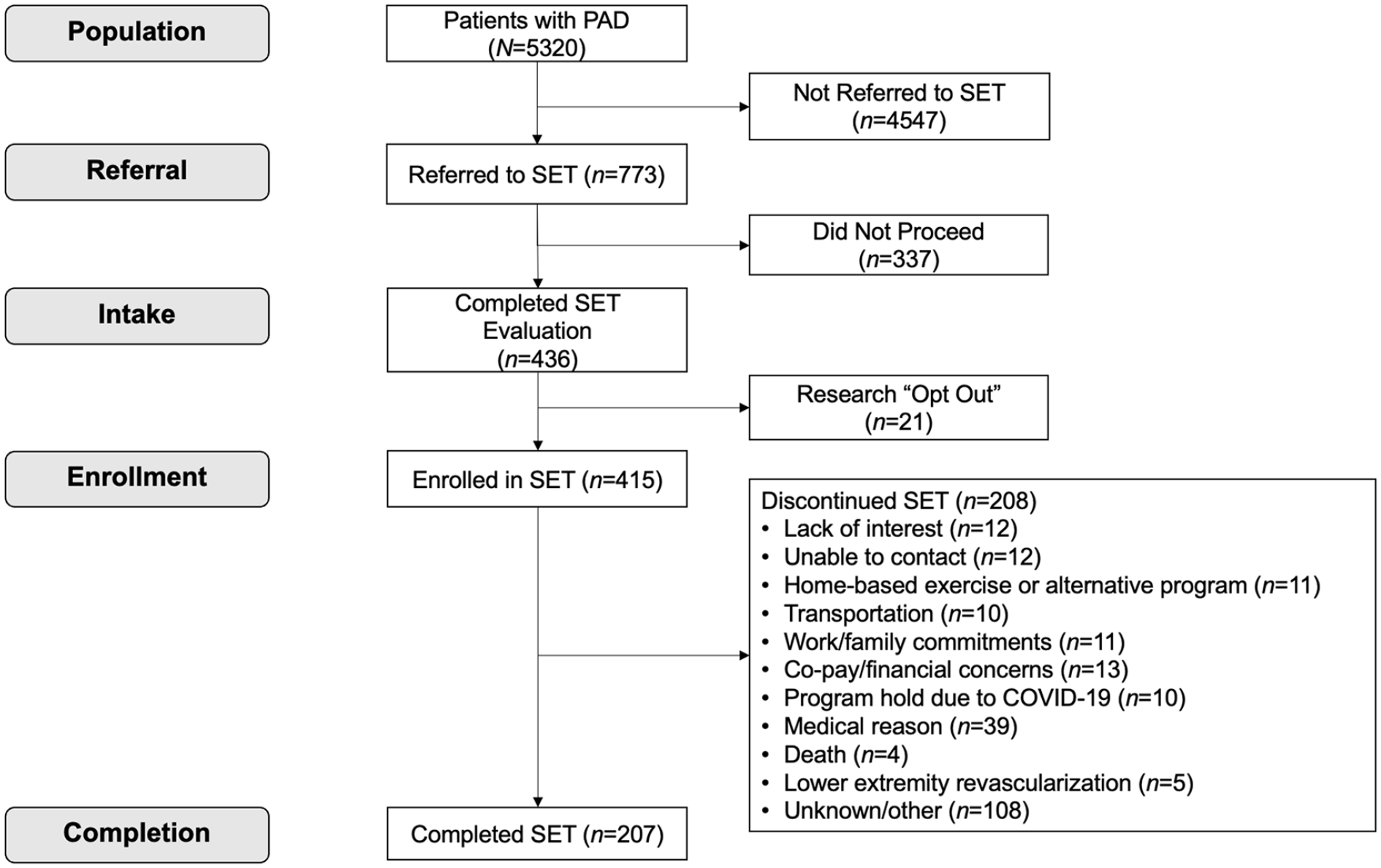
Flowchart of patients with PAD, referrals, and those included in the present study.
Descriptive statistics on patients who completed a SET evaluation, including age, sex, race, medical comorbidities, and referral source are reported in Table 1. Patients were referred by 65 unique referred providers, most frequently by vascular medicine and vascular surgery specialists (30.6% and 51.6%, respectively). The number of individual patients referred by each provider ranged from one to 49 (a vascular surgeon). The most common indication for SET was International Classification of Diseases, 10th Revision (ICD-10) code I70.2 (atherosclerosis of native arteries of the extremities).
Demographic and medical characteristics of patients who completed a supervised exercise therapy evaluation, 2017–2022 (N = 415).
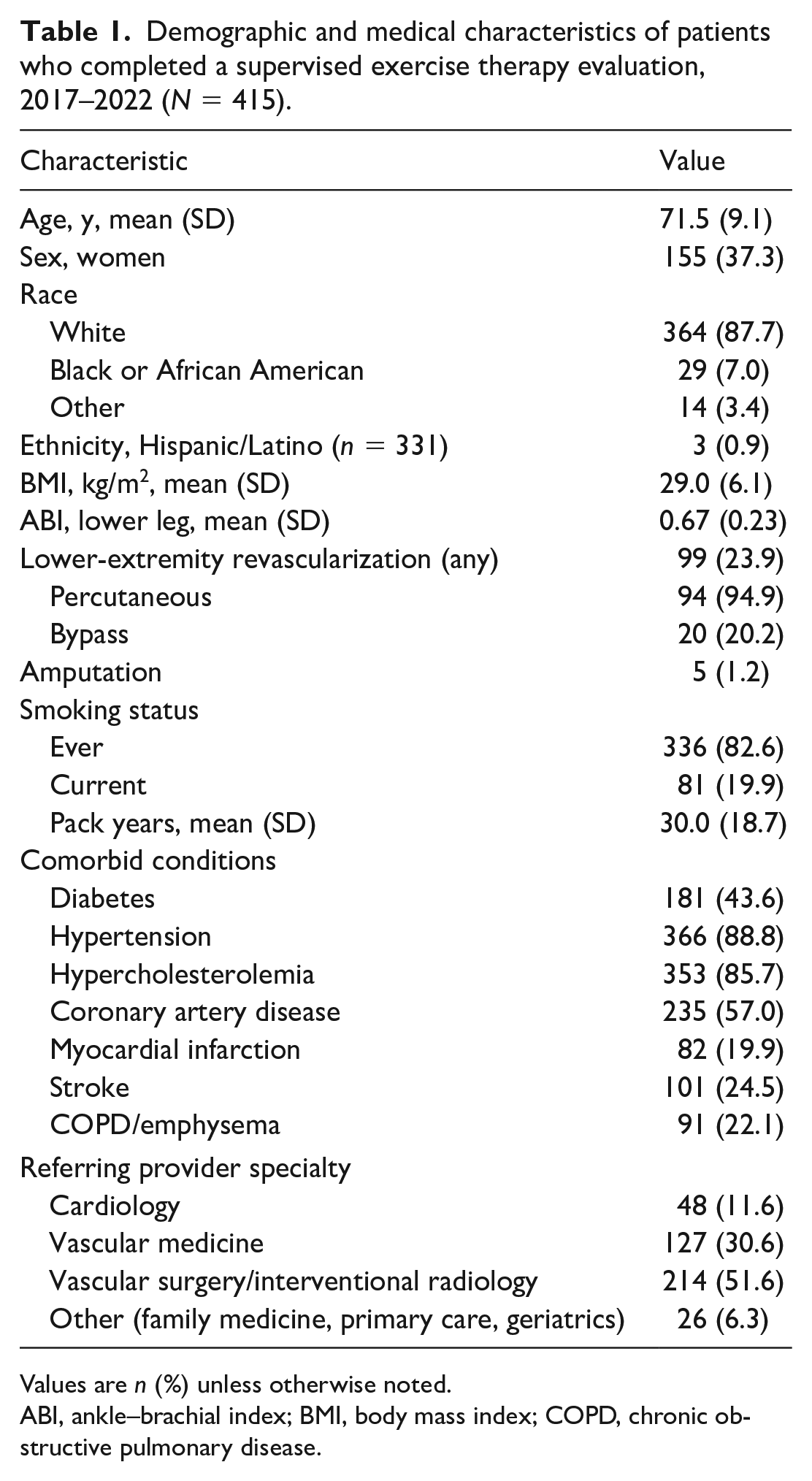
Values are n (%) unless otherwise noted.
ABI, ankle–brachial index; BMI, body mass index; COPD, chronic obstructive pulmonary disease.
Overall, 49.9% of patients completed the SET program (defined as completing a formal discharge visit). In the entire sample, n = 87 (21.0%) patients completed ⩾ 30 sessions, 49 (11.8%) completed 24–29 sessions, and 279 (67.2%) completed < 24 sessions over the 12 weeks. Despite the wide range of participation, on average, participants completed approximately 18 out of the 36 training sessions, collectively a 49.7% session adherence rate. Adherence was 72% among patients who completed the program and 24.9% among patients who discontinued SET prior to formal discharge (Table 2).
Supervised exercise therapy session attendance and adherence among all patients (N = 415) and those who completed the supervised exercise therapy (n = 207).
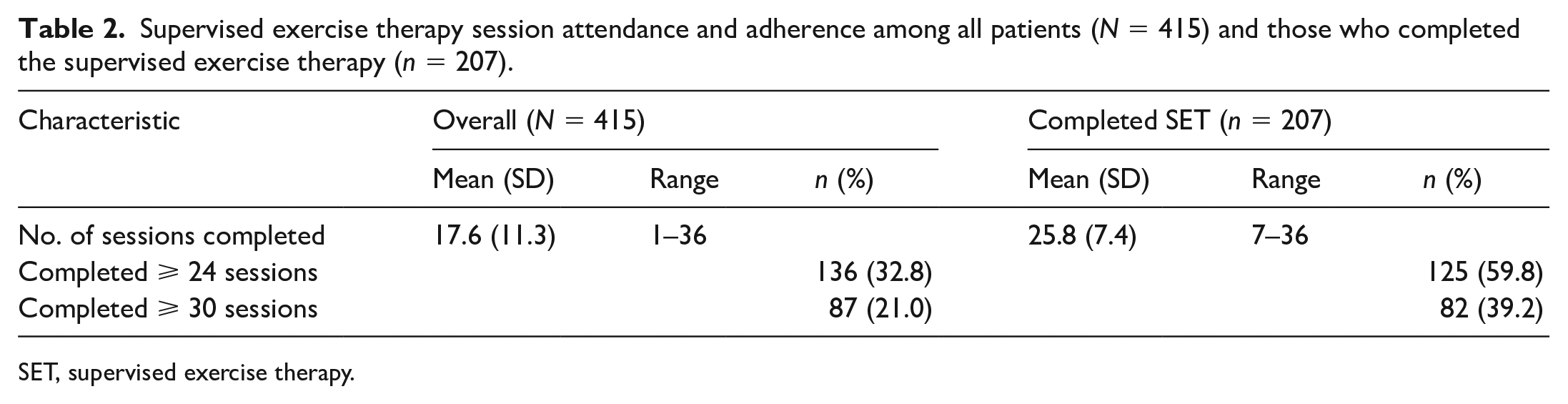
SET, supervised exercise therapy.
Changes in 6MWT, TUG, and VascuQoL-6 are reported in Table 3. Statistically significant improvements were observed in all outcomes. The mean improvement in 6MWT total distance was 28.1% (range: 75% decline to 419% improvement) and the mean improvement in treadmill METs was 43.7% (range: 10% decline to 181% improvement). A total of 78% of patients achieved at least a small, clinically meaningful improvement in 6MWT total distance and 65.3% of patients who reported symptoms during the 6MWT achieved a clinically meaningful improvement in 6MWT claudication onset distance.
Changes in physical function outcomes following 12 weeks of supervised exercise therapy (n = 207).
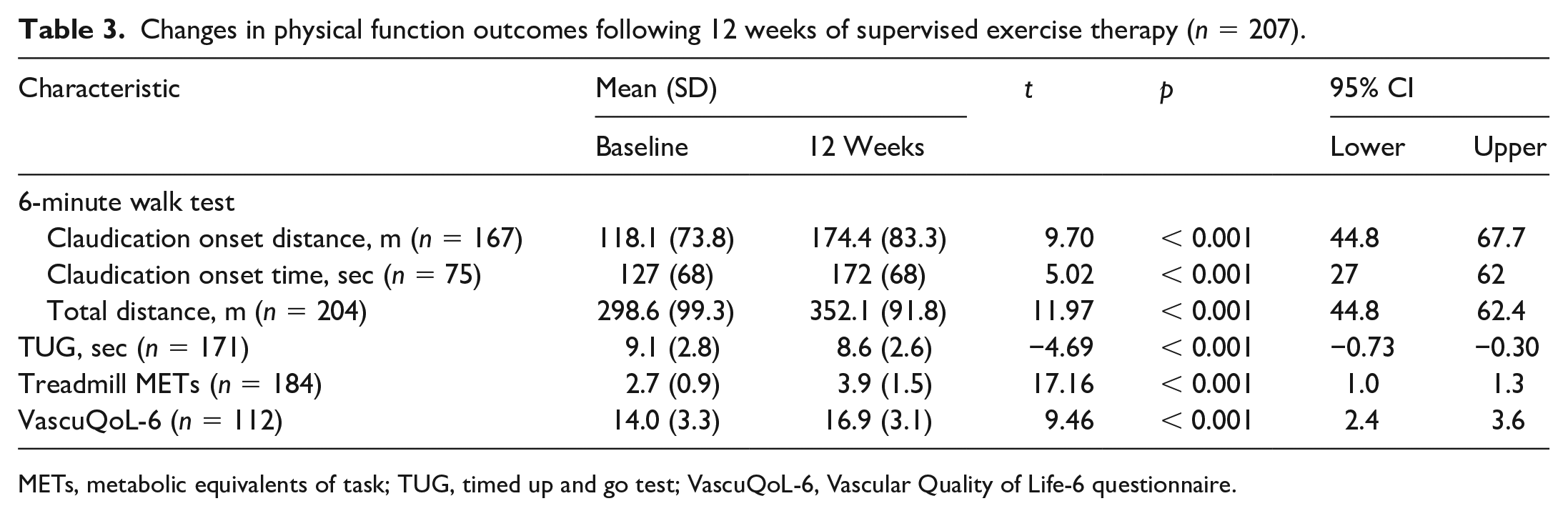
METs, metabolic equivalents of task; TUG, timed up and go test; VascuQoL-6, Vascular Quality of Life-6 questionnaire.
Analyses were repeated adjusting for age, sex, BMI, ABI, diabetes, current smoking, and prior lower-extremity revascularization. Of the included covariates, only current smoking was significantly related to change in 6MWT total distance (Table 4). Current smoking was associated with a 32-meter smaller improvement in 6MWT total distance, compared to nonsmokers (B = −32.1, p = 0.019). None of the included covariates were significantly associated with 6MWT claudication onset distance or claudication onset time. There were no differences in SET completion rates or outcomes based on referring provider specialty.
Multiple linear regression examining the relationship between changes in 6MWT total distance following supervised exercise therapy, adjusting for age, sex, ankle–brachial index, diabetes, current smoking, and lower-extremity revascularization.
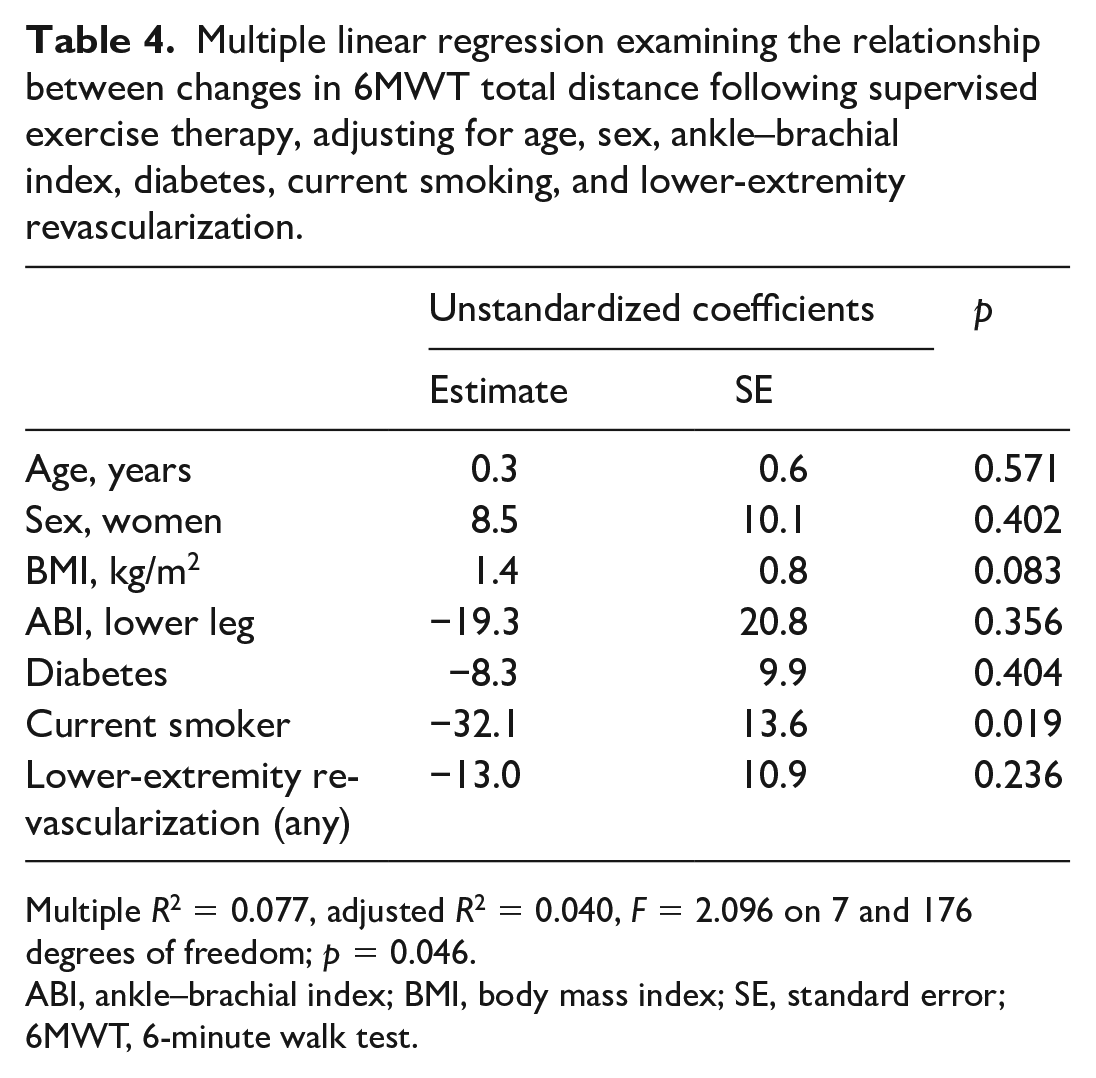
Multiple R2 = 0.077, adjusted R2 = 0.040, F = 2.096 on 7 and 176 degrees of freedom; p = 0.046.
ABI, ankle–brachial index; BMI, body mass index; SE, standard error; 6MWT, 6-minute walk test.
Discussion
This retrospective review of patients referred to SET during the first 5 years of CMS reimbursement revealed low rates of SET referral and completion despite an excellent clinical infrastructure. Despite the low overall rates of referral, the volume of intake visits remained relatively stable across the 5 years. Currently, there are few data available regarding referral and uptake into SET programs. In this study, of the 5230 patients who were eligible for SET, only 8.1% enrolled in SET. This is worse than the low 20% uptake reported for cardiac rehabilitation programs. 17 Furthermore, the 14.5% referral rate to our SET program is lower than the current rate reported for cardiac rehabilitation programs, 17 but higher than reports from the first 2 years of CMS-reimbursed SET. 3 For example, a review of Medicare data (June 1, 2017 to December 31, 2018) regarding SET referrals and participation by Divakaran and colleagues showed that only 1.3% of patients with a SET-eligible ICD-10 code enrolled and completed at least one SET session. Likewise, the average attendance during the 12-week SET program is on par again with findings from Divakaran et al.; however, this paper did not differentiate attendance between patients who did and did not complete SET.
These low rates of referral also present an opportunity for increased engagement in and awareness of these programs. Vascular medicine specialists serve a key role in increasing SET program uptake. Although efforts were made to increase provider awareness of the availability of SET programs in our health system, it is unclear if all potential referring providers were aware of the program. A 2020 report by Dua and colleagues of a sample of 135 respondents (94% of whom were vascular surgeons), indicated there was low availability of SET programs. Additionally, about half of the respondents had ever referred a patient to SET but 98% would refer patients with claudication to SET if available. 18 Patients in the present study were referred by a total of 65 unique providers, approximately 32% of whom were vascular medicine specialists. This is despite the fact that there are twice as many vascular surgeons and interventional radiologists as vascular medicine specialists in the M Health Fairview system. The percentage of patients referred to SET by vascular medicine specialists may underestimate their true impact, as advocacy by vascular medicine specialists likely influenced referral patterns among vascular surgeons.
Inclusion of a SET referral in vascular order sets system-wide may be a strategy toward increasing knowledge of SET availability and the rate of referral among all specialties. Additional efforts are needed to not only increase program availability, but also awareness and understanding of the benefits of such programs. SET is an important component of guideline-directed medical therapy yet SET remains a major gap in the care of patients with PAD. 19 Vascular medicine specialists are essential in supporting the growth of these programs and improved patient outcomes through referral, patient education, and advocacy.
Despite low rates of referral, patients who completed 12 weeks of SET exhibited statistically and clinically meaningful improvements in all measured outcomes. On average, patients had a 53.6 meter improvement in 6MWT total distance, which is considered a large change (defined by Gardner and colleagues as 34 meters) and 78% of patients exhibited at least a small, clinically meaningful improvement (12 meters). 11 Similarly, 65.3% of patients achieved a clinically meaningful improvement in claudication onset distance (defined as 24 meters). 11 These improvements are in alignment with clinically meaningful improvements previously established in patients with PAD 11 and in cardiac and pulmonary rehabilitation 20 programs. Notably, although most patients’ walking ability improved following SET, benefit was not universal. Approximately 14% of patients who completed SET did not demonstrate an improvement in 6MWT total distance at 12 weeks. Additional work is needed to better understand how to optimize outcomes for all patients with PAD.
Although clinical SET programs are in their infancy, other clinical programs such as cardiac and pulmonary rehabilitation programs have registries to guide the establishment of clinical performance and quality measures. Recently, the American College of Cardiology and American Heart Association have provided an update to a comprehensive measure set of six performance and three quality measures. 20 These were initially established with the goal of enhancing the structure, process, and outcomes of care for patients eligible for cardiac rehabilitation services. Using data from established programs, these measures could be incorporated into developing SET programs as quality indicators. For instance, Performance Measure 3: ‘Cardiac Rehabilitation Patient Referral from an Outpatient Setting’ and Performance Measure 5B: ‘Cardiac Rehabilitation Enrollment’ could be implemented in SET programs for PAD. In the present study, Performance Measure 3 (defined as the percentage of patients with an ICD-10 code eligible for SET that were referred to SET) is 14.5%. Likewise, Performance Measure 5B (percentage of patients with an ICD-10 code eligible for SET that attended at least one SET session) is 8.1%.
Additionally, the American Association of Cardiovas-cular and Pulmonary Rehabilitation offers specific performance measures for improvement in functional capacity at completion of cardiac rehabilitation that could be adapted into SET programs. 15 These include the percentage of patients who increase their functional capacity measured by either (1) peak METs (increase in METs by at least 40%) or (2) 6MWT distance (increase in distance by 10%). When looking at our registry, 44% of patients improved peak METs by ⩾ 40%, and 60% of patients saw improvements of ⩾ 10% on 6MWT. The establishment of performance and quality measures for SET programs and further development of SET registries to help guide these measures represent a future direction of study. As with cardiac rehabilitation, the establishment of performance and quality measures for SET will represent a potential to: (1) identify key performance and quality measures for new and developing SET programs; (2) increase referrals by all specialties by demonstrating the effectiveness and structure of SET programs; and (3) improve outcomes in patients with PAD.
Study limitations
This study has several limitations. First, the use of a registry from a single health system in the Midwest with low representation of non-White patients limits the generalizability of our findings. Patient composition and rates of referral, completion, and outcomes are likely to vary by site. 21 However, this study provides insight into a large health system with a robust SET program, which may serve as a guide for other health systems seeking to establish their own programs. Additionally, patients who chose to ‘opt out’ of the use of their medical record for research were not included. Second, because ‘vascular medicine’ as a specialty is not captured in the electronic medical record at our health system, some misclassification of referring provider specialty may have occurred. Third, as patients who discontinued SET did not complete discharge, much of their outcome data are unavailable. Although not explicitly stated, patients may have discontinued due to lack of observed improvement. Although previous work has not identified clear factors in lack of response to SET,7,22 clinically available SET programs may provide a unique opportunity to better individualize SET sessions and intervene earlier with alternative modes of exercise23,24 or other strategies to maximize response. Also, as we were limited to data reported in the medical record in our health system, we were unable to track patients who chose to proceed with SET at an outside institution. Notably, of the patients who completed an intake visit but chose not to proceed with SET (n = 208), only one patient (0.5%) indicated they planned to enroll in SET at another institution. Finally, we did not examine long-term outcomes of SET in this study, although some patients had already enrolled in a second set of 36 sessions during this period. Additional work is needed to understand the value and optimal timing of these additional sessions.
Conclusion
SET referral and completion rates are low in the 5 years following the CMS-reimbursement determination, despite significant improvement in patient functional capacity and quality of life. Data support the value of SET and the critical role of vascular medicine specialists in connecting patients with available programs. In addition, developing a registry to establish clinical performance and quality measures will be key as we work to expand the availability of SET programs across the country as part of comprehensive treatment of PAD.
Footnotes
Data availability
The datasets generated and analyzed during the current study are not publicly available due to privacy reasons but are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research reported in this publication was supported by a Building the Evidence Base for Vascular Medicine Award from the Society for Vascular Medicine and by the National Institutes of Health through the National Institute of Arthritis Musculoskeletal and Skin Diseases (K12AR084223) and the National Center for Advancing Translational Sciences (UL1TR002494). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.