
Abstract
Pulmonary embolism (PE), which comprises approximately one-third of all venous thromboembolism (VTE), 1 exhibits various clinical presentations, ranging from incidentally discovered emboli to hemodynamic instability and death, and its 1-year mortality rate has been reported to exceed 20%. 2 Ischemic stroke is one of the major cardiovascular disorders associated with thrombosis as a common pathology along with ischemic heart disease and VTE. 3 According to recent studies, the occurrence of PE in patients with ischemic stroke is associated with poor clinical outcomes.4,5 However, information on how the history of ischemic stroke affects patients with PE in terms of clinical manifestations and survival is limited. Thus, the objective of this retrospective study was to investigate whether clinical characteristics and outcomes might differ according to the history of ischemic stroke in patients with PE.
Data were collected from patients with PE who were hospitalized between January 2003 and May 2019 at Kyungpook National University Hospital (KNUH), a tertiary referral center in Daegu, South Korea. This study was approved by the Institutional Review Board of the KNUH, which waived the requirement for written informed consent due to its retrospective nature. Patients with PE diagnosed using multidetector-row computed tomography (CT) were included and divided into a stroke group (with a history of ischemic stroke) and a control group (without a prior ischemic stroke). The history of ischemic stroke before the diagnosis of PE was identified by comprehensively reviewing clinical diagnosis and past hospitalization from the medical records, regardless of the time of diagnosis. Clinical characteristics, blood biomarkers, and CT findings were compared between the two groups. To identify predictors of PE-related in-hospital mortality, multivariable logistic regression analysis was performed using Firth’s Penalized Likelihood method.
Results of comparisons of clinical characteristics, blood biomarkers, and CT findings are summarized in Table 1. Of 1339 patients with PE, 115 (8.6%) had a history of ischemic stroke. The median follow-up time was 306 days (IQR, 73–1082 days). The proportion of unprovoked PE was lower in the stroke group than in the control group (p = 0.003), whereas the frequency of immobilization was higher (p < 0.001). Comorbidities, including diabetes mellitus (p = 0.035), ischemic heart disease (p = 0.002), and atrial fibrillation (p < 0.001), were more common in the stroke group. Despite the insignificant difference between the two groups in PE severity index (PESI) and CT findings, PE-related in-hospital mortality was significantly higher in the stroke group than in the control group (p = 0.002). The patients were further reclassified into those with (n = 22) and without (n = 1317) PE-related in-hospital death (online supplementary material: Table S1). Variables with p < 0.05 in univariate analysis were included in the multivariable logistic regression analysis. Atrial fibrillation (odds ratio [OR], 3.64; 95% CI, 1.18‒11.29; p = 0.022), PESI class IV‒V (OR, 3.98; 95% CI, 1.72‒9.25; p = 0.001), right ventricular dilation on CT (OR, 3.52; 95% CI, 1.41‒8.78; p = 0.007), and stroke (OR, 4.87; 95% CI, 1.92–12.35; p < 0.001) were identified as an independent factor for predicting PE-related in-hospital mortality.
Clinical characteristics, blood biomarkers, and computed tomography findings.
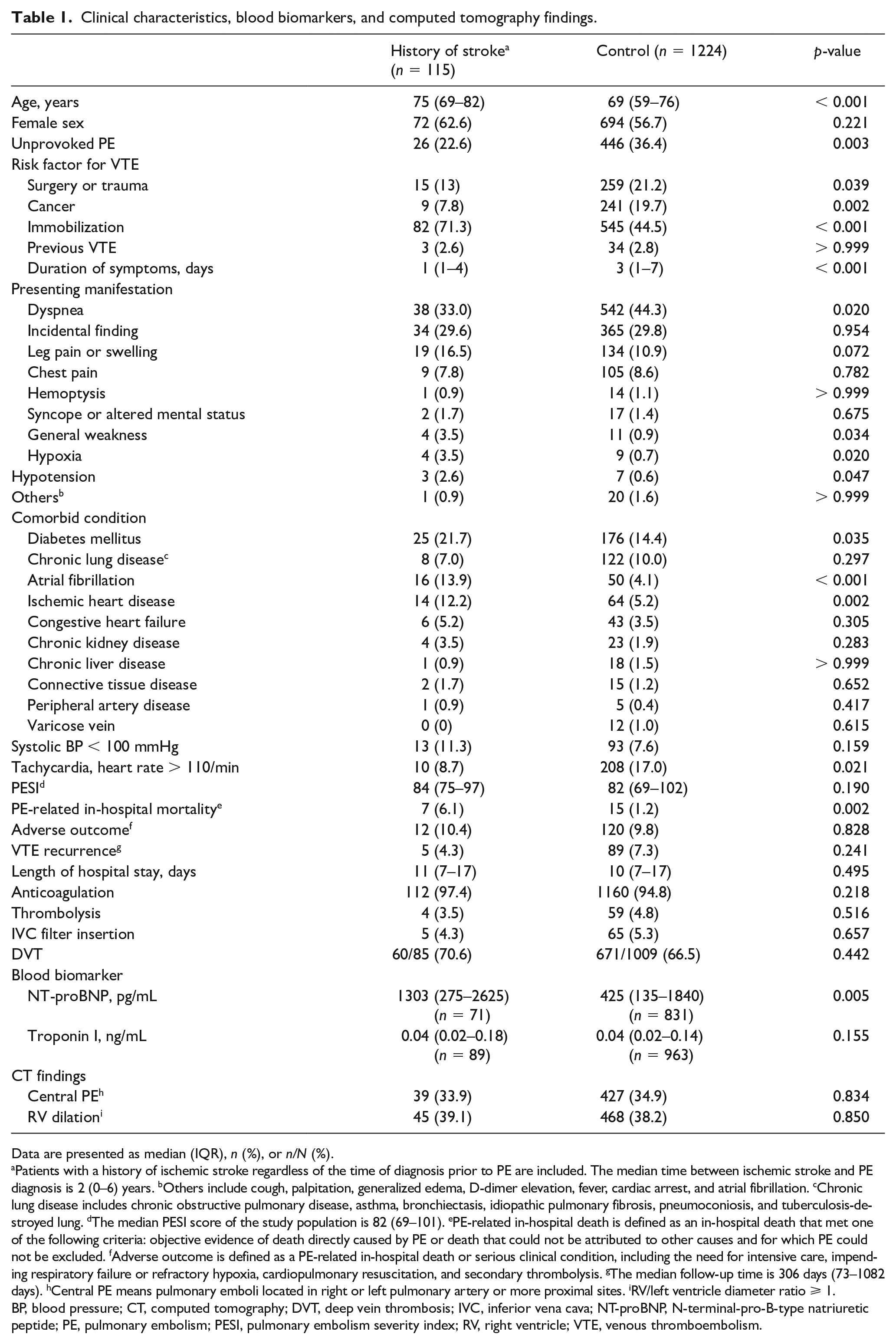
Data are presented as median (IQR), n (%), or n/N (%).
Patients with a history of ischemic stroke regardless of the time of diagnosis prior to PE are included. The median time between ischemic stroke and PE diagnosis is 2 (0–6) years. bOthers include cough, palpitation, generalized edema, D-dimer elevation, fever, cardiac arrest, and atrial fibrillation. cChronic lung disease includes chronic obstructive pulmonary disease, asthma, bronchiectasis, idiopathic pulmonary fibrosis, pneumoconiosis, and tuberculosis-destroyed lung. dThe median PESI score of the study population is 82 (69–101). ePE-related in-hospital death is defined as an in-hospital death that met one of the following criteria: objective evidence of death directly caused by PE or death that could not be attributed to other causes and for which PE could not be excluded. fAdverse outcome is defined as a PE-related in-hospital death or serious clinical condition, including the need for intensive care, impending respiratory failure or refractory hypoxia, cardiopulmonary resuscitation, and secondary thrombolysis. gThe median follow-up time is 306 days (73–1082 days). hCentral PE means pulmonary emboli located in right or left pulmonary artery or more proximal sites. iRV/left ventricle diameter ratio ⩾ 1.
BP, blood pressure; CT, computed tomography; DVT, deep vein thrombosis; IVC, inferior vena cava; NT-proBNP, N-terminal-pro-B-type natriuretic peptide; PE, pulmonary embolism; PESI, pulmonary embolism severity index; RV, right ventricle; VTE, venous thromboembolism.
Few studies have reported the proportion of patients with a history of stroke in patients with PE. Based on data of 2488 patients hospitalized with VTE, Piazza et al. reported that 288 (11.6%) had a clinical history of stroke and that prior stroke was associated with an increased risk of short-term mortality compared with patients without stroke. 6 Given that VTE encompasses deep vein thrombosis (DVT) and PE, which are in the same disease spectrum, 7 our data are consistent with those of Piazza et al. 6 The finding that patients with prior stroke had a higher PE-related in-hospital mortality rate than those without a history of stroke might be partly explained by differences in the underlying conditions. Diabetes mellitus and heart diseases, such as atrial fibrillation and acute coronary syndrome, are known risk factors for ischemic stroke. 8 They were more commonly identified in the stroke group than in the control group in the present study. Moreover, immobilization has been previously demonstrated to be a potent predictor of fatal PE. 9 These vulnerable medical conditions, which were more frequent in the stroke group, might have impeded patients’ recovery from acute PE-triggered deterioration and affected the short-term mortality. Since this study was retrospectively conducted at a single center, selection bias was inevitable. The small number of PE-related in-hospital mortality, as an outcome variable, was another limitation.
In conclusion, patients with PE and a history of ischemic stroke had worse clinical outcomes such as PE-related in-hospital mortality. However, there were no significant differences in the PESI score and RV dilation on CT between patients with stroke and those without stroke. These results imply that patients with PE should be closely investigated for stroke history and that those with prior stroke would need more careful treatment and attention.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211055772 – Supplemental material for History of ischemic stroke associated with worse clinical outcomes in patients with pulmonary embolism
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211055772 for History of ischemic stroke associated with worse clinical outcomes in patients with pulmonary embolism by Yong Hoon Lee, Seung-Ick Cha, Jongmin Park, Jae Kwang Lim, Won Kee Lee, Ji-Eun Park, Sun Ha Choi, Hyewon Seo, Seung-Soo Yoo, Shin-Yup Lee, Jaehee Lee, Chang-Ho Kim and Jae-Yong Park in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.