
Abstract
Background:
Data regarding the mortality trends in pulmonary embolism (PE)-related mortality in patients with concomitant pulmonary hypertension (PH) are lacking. We assessed the trends in PE-related mortality in patients with concomitant PH in the United States (US) over the past 2 decades and during the first year of the COVID-19 pandemic using data from the Centers for Disease Control and Prevention’s (CDC) Wide-ranging ONline Data for Epidemiologic Research (WONDER) dataset.
Methods:
Mortality data were retrieved from the publicly available CDC WONDER mortality dataset from 2003 to 2020. Age-adjusted mortality rates (AAMRs), per 100,000 population, were assessed using Joinpoint regression modelling and expressed as estimated average annual percentage change (AAPC) with relative 95% CIs and stratified by urbanicity, sex, age, and race/ethnicity.
Results:
Over the study period, the AAMR for PE/PH-related mortality linearly increased (AAPC: +4.3% [95% CI: 3.7 to 4.9], p < 0.001) without sex differences. The AAMR increase was more pronounced in White individuals (AAPC: +4.8% [95% CI: 4.1 to 5.5], p < 0.001) and in subjects living in rural areas (AAPC: +5.1% [95% CI: 3.8 to 6.4], p < 0.001) compared to those living in urban areas. During the first year of the COVID-19 pandemic there was a significant excess in PE/PH-related mortality among women, older than 65 years and living in rural areas.
Conclusions:
The rate of PE/PH-related mortality in the US is increasing. Although the early diagnosis of PH in patients with acute PE has become easier with improved diagnostic modalities, the mortality rate of these patients remains high.
Background
The hemodynamic response to acute pulmonary embolism (PE) is heterogeneous, ranging from a normotensive state to sudden cardiac death.1–4 Randomized controlled trial data demonstrate important short- and long-term hazards for patients with intermediate-risk PE, including many with an initial presentation of concomitant PH. Among patients assigned to anticoagulation, the short-term risk of death and hemodynamic collapse approached 5.6%. At two years, 18.5% of patients in the anticoagulation group had echocardiographic evidence of increased pulmonary artery systolic pressure. 5 The incidence and prevalence of pulmonary hypertension (PH) associated with acute PE and with chronic thrombus are not well established. Furthermore, in daily clinical practice, the temporal relationship of the PH to the PE remains often unclear. 6 Patients with acute PE with concomitant PH have a higher mortality risk, primarily driven by the higher prevalence of right ventricular dysfunction (RVD). 7 At present, there are limited medical therapies to acutely reduce elevated RV afterload in patients with PE: both inhaled nitric oxide (iNO) and diuretics8–12 have been proposed as potential therapeutic agents to optimize RV. However, the current impact of PH on mortality in patients with acute PE remains unclear. To partially fill this gap, the aim of the present study is to assess the trends in PE-related mortality in patients with concomitant PH in the United States (US) over the past 17 years and during the first year of the COVID-19 pandemic using data from the Centers for Disease Control and Prevention’s (CDC) Wide-ranging ONline Data for Epidemiologic Research (WONDER) dataset. 13
Methods
Data source and definitions
Data were retrieved through the publicly available CDC WONDER 13 dataset, which provides information from death certificates of all US residents according to the International Classification of Diseases, Tenth Revision (ICD-10). The database also includes demographic and geographical data such as age, sex, race, ethnicity, and urbanization category. The definitions of acute PE and PH used in this analysis, as well as their validation, are consistent with prior publications examining these conditions.13–16 ICD-10 codes have shown an acceptable accuracy for PH, with specificities and negative predictive values > 97.5%.16,17 Specifically, PE-related deaths were ascertained when the ICD-10 codes for acute PE I26, I82.8, and/or I82.9 were listed in any position on the death certificate. Conversely, the presence of PH was determined by the presence of ICD-10 codes I27.2, I27.8 and/or I27.9 listed as contributing causes of death in the multiple cause of death dataset. These ICD-10 codes cover PH that is not pulmonary arterial hypertension (PAH) and includes PH due to lung disease, cardiac disease, and chronic thromboembolic disease. Data regarding the temporal relationship between PE, PH, and mortality were not provided by the CDC WONDER dataset precluding the assessment of PH temporality in respect of the PE diagnosis. Therefore, PH could have preceded the onset of acute PE. In daily clinical practice, however, the management of patients with PE with PH remains problematic, independent from the etiology.
Although ICD-10 codes were implemented in the billing and care of patients at the end of 2015, the World Health Organization (WHO) originally authorized the publication of ICD-10 in 1999. ICD-10 codes were instituted for mortality coding and for classification of cause-of-death on patient death certificates in the US beginning in 1999 and spanning the entire study period.18,19 We used annual national population totals for sex, age group, race, and ethnicity obtained by the US Census Bureau. 20 The stratification between urban and rural counties was performed in accordance with the 2013 National Center for Health Statistics Urban-Rural Classification Scheme. Furthermore, mortality trends were also analyzed by the US census regions (Northeast, Midwest, South, and West). The study did not require institutional review board approval because the analysis utilized de-identified and publicly available data.
Data extraction
Data extraction and validation was performed by the study team (led by MZ). We abstracted the number of patients with PE, contributing causes of death, the population size from 2003 (first year with available data) to 2020, as well as data on age, sex, race, ethnicity, urbanicity, and census region in all US subjects, without any restriction for age. Subjects less than 65 years old were classified as premature deaths. Ethnicity was defined as Latinx/Hispanic or non-Latinx/Hispanic, whereas race was categorized as White, Black, American Indian/Alaska Native, and/or Asian/Pacific Islander.
Statistical analyses
PE-related PH age-adjusted mortality rates (AAMR) per 100,000 people, along with the relative 95% CIs, were calculated by standardizing the related deaths using the annual national population totals from the US Census Bureau and the 2000 US standard population.21,22 To calculate nationwide annual trends in PE-related PH mortality, we assessed the average percent change (APC) and average annual percent change (AAPC), both of which are reported with relative 95% CIs. We also carried out a further sub-analysis to assess the impact of SARS-CoV-2 infection during the first year of the pandemic (i.e., 2020) on PE-related PH mortality rates. Considering that the abstracted data contained 21 time points, we identified a maximum of four inflection points across the study period, as suggested by the current joinpoints guidelines. 20 Statistical analyses were performed using Joinpoint regression (Joinpoint, version 4.6.0.0; National Cancer Institute, USA). Joinpoint regression software determines the inflection points for each population of interest across the study period according to prespecified varying time intervals. A parallelism test was used to examine whether groups have similar or different trends. 23 Specifically, a significant p-value on this interaction test indicated that the two APCC trends were statistically significantly different from each other. Statistical significance was prespecified at p ⩽ 0.05 for findings in the entire population.
Results
Overall population
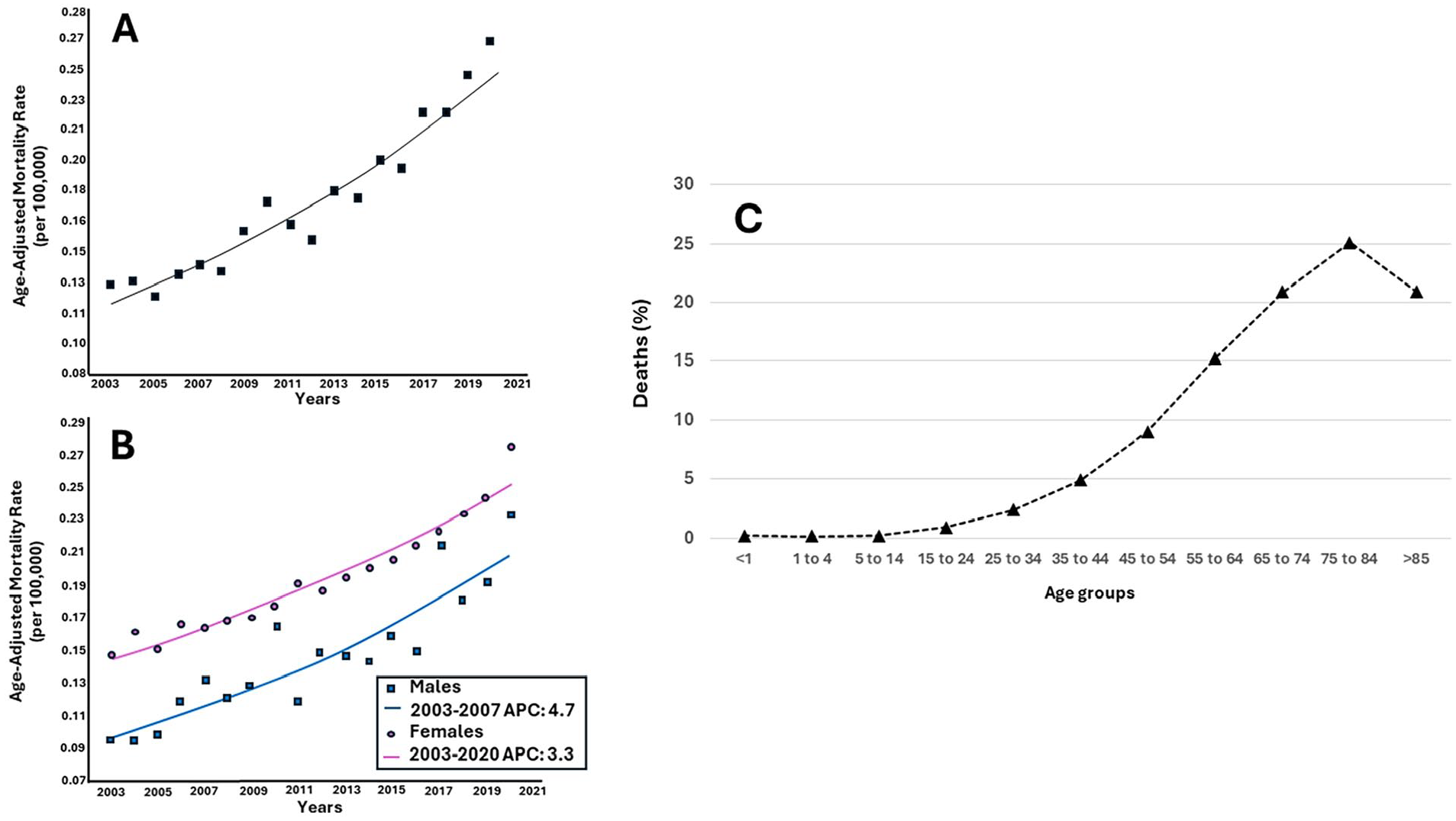
In the US, over a study period from 2003 through 2020, there were 590,368 patients (277,438 men and 312,930 women) who died from acute PE. Of these, PH was listed as the cause of death or underlying cause of death in 11,433 patients (1.9% of cases: 4240 men and 7193 women, respectively), equating to 635 mean deaths per year (Figure 1A). The proportional mortality, defined as the PH-related mortality in those who died from PE compared with those who died from all causes, followed a similar exponential increase (Figure 2). The absolute number of PH-related deaths in patients with PE increased from 376 subjects in 2003 (116 men and 260 women) to 1063 subjects (403 men and 660 women) in 2020. In the same manner, the AAMR for PE/PH-related mortality increased linearly, without evidence of joinpoints, from 0.13 (95% CI: 0.11 to 0.14) per 100,000 in 2003 to 0.15 (95% CI: 0.13 to 0.17) per 100,000 in 2020 (AAPC: +4.3% [95% CI: 3.7 to 4.9], p < 0.001) (Table 1 and Figure 1B). Over the same period, the AAMR for PE- (from 9.60 [95% CI: 9.49 to 9.71] to 9.86 [from 9.76 to 9.96]; AAPC: +0.3, 95% CI: 0.1 to 0.5, p = 0.04) and PH-related deaths (from 5.02 [95% CI: 4.94 to 5.11] to 7.56 [from 7.48 to 7.65]; AAPC: +2.3, 95% CI: 2.1 to 2.5, p < 0.001) showed similar increases (p for parallelism 0.23).
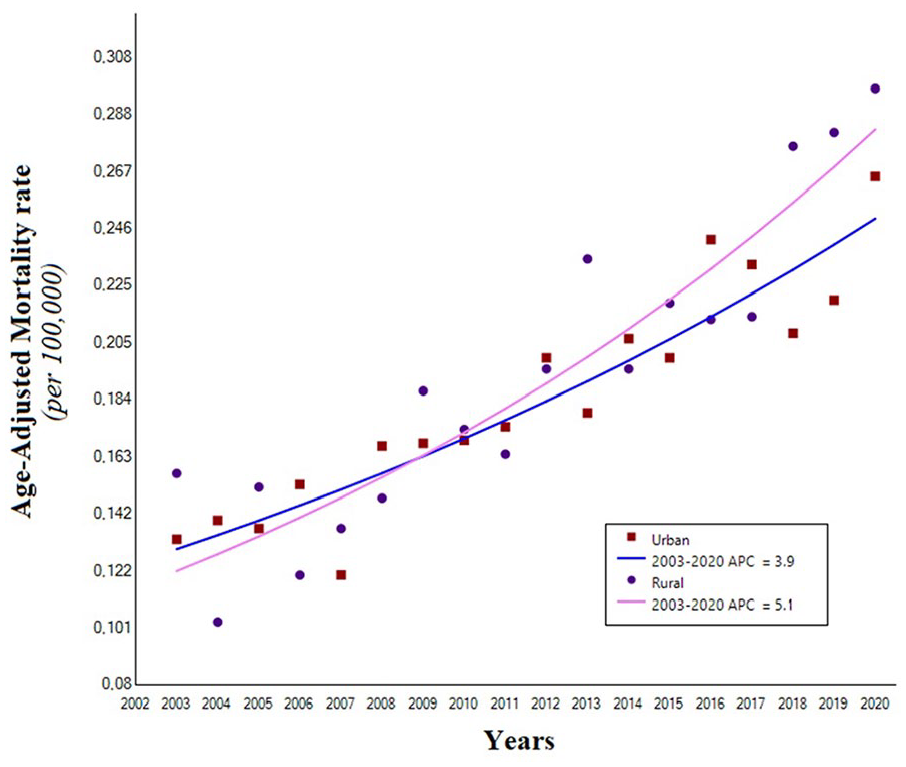
Trends in age-adjusted mortality rates due to pulmonary embolism/pulmonary hypertension-related deaths, stratified by urbanicity (urban = squares; rural = circles), in the United States, 2003–2020.
Age-adjusted mortality rate trend for pulmonary embolism/pulmonary hypertension-related mortality in the United States, 2003–2020, stratified by sex, race, and ethnicity.

Joinpoint regression software determines the inflection points for each population of interest across the study period according to prespecified varying time intervals.
AAMR, age-adjusted mortality rate, expressed as deaths per 100,000 population; AAPC, average annual percent change; APC, annual percent change.
Sex
Men and women had similar increases in AAMR for PE/PH-related mortality (p for parallelism 0.14). Specifically, in men, the AAMR increased from 0.09 (95% CI: 0.07 to 0.11) per 100,000 in 2003 to 0.24 (95% CI: 0.21 to 0.26) per 100,000 in 2020 (AAPC: +4.7% [95% CI: 3.6 to 5.8], p < 0.001). In women, the AAMR increased from 0.15 (95% CI: 0.13 to 0.17) per 100,000 in 2003 to 0.29 (95% CI: 0.27 to 0.31) per 100,000 in 2020 (AAPC: +3.3% [95% CI: 2.9 to 3.7]) (Table 1 and Figure 1C).
Race and ethnicity
In White individuals, the AAMR for PE/PH-related mortality rose from 0.10 (95% CI: 0.08 to 0.11) per 100,000 in 2003 to 0.25 (95% CI: 0.23 to 0.28) per 100,000 in 2020, without any inflection points (AAPC: +4.8% [95% CI: 4.1 to 5.5], p < 0.001). In non-Latinx/Hispanic Black individuals, the AAMR rose from 0.09 (95% CI: 0.07 to 0.11) in 2003 to 0.24 (95% CI: 0.21 to 0.26) in 2020 (AAPC: +2.9% [95% CI: 1.2 to 4.5], p = 0.001). Specifically, the AAMR in these subjects plateaued between 2003 and 2008 (APC: –1.7% [95% CI: –6.6 to 3.4], p = 0.47) and then significantly increased from 2008 to 2020 (APC: +4.9% [95% CI: 3.5 to 6.3], p < 0.001). Similarly, in Latinx/Hispanic individuals, the AAMR increased from 0.08 (95% CI: 0.06 to 0.15) per 100,000 in 2003 to 0.12 (95% CI: 0.08 to 0.16) per 100,000 in 2020 (AAPC: +2.9% [95% CI: 1.5 to 4.3], p < 0.001) (Table 1). Owing to the discontinuity of data and low estimates, we were unable to calculate specific trends for American Indians/Alaska Natives and Asians/Pacific Islanders. However, such cases were computed in both the general and sex-stratified analyses.
Age
From 2003 to 2020, 3762 subjects (1628 men and 2134 women) less than 65 years old accounted for 32.9% of all PE/PH-related deaths. These patients showed a similar increase in PE/PH-related deaths compared with patients 65 years or older over the entire study period (p for parallelism = 0.88). Indeed, the relative AAMR rose from 0.05 (95% CI: 0.04 to 0.06) per 100,000 in 2003 to 0.10 (95% CI: 0.09 to 0.11) per 100,000 in 2020 (AAPC: +4.2% [95% CI: 2.8 to 5.7], p < 0.001) (Table 2). In comparison, in subjects ⩾ 65 years with PE/PH-related deaths (7671 subjects; 3460 men and 4211 women), the AAMR increased from 0.34 per 100,000 (95% CI: 0.28 to 0.42) in 2003 to 0.49 per 100,000 (95% CI: 0.47 to 0.52) in 2020 (AAPC: +4.1% [95% CI: 3.6 to 4.7], p < 0.001) (Table 2).
Age-adjusted mortality rate trend for acute pulmonary embolism/pulmonary hypertension-related mortality in the United States, 2003–2020, stratified by age.
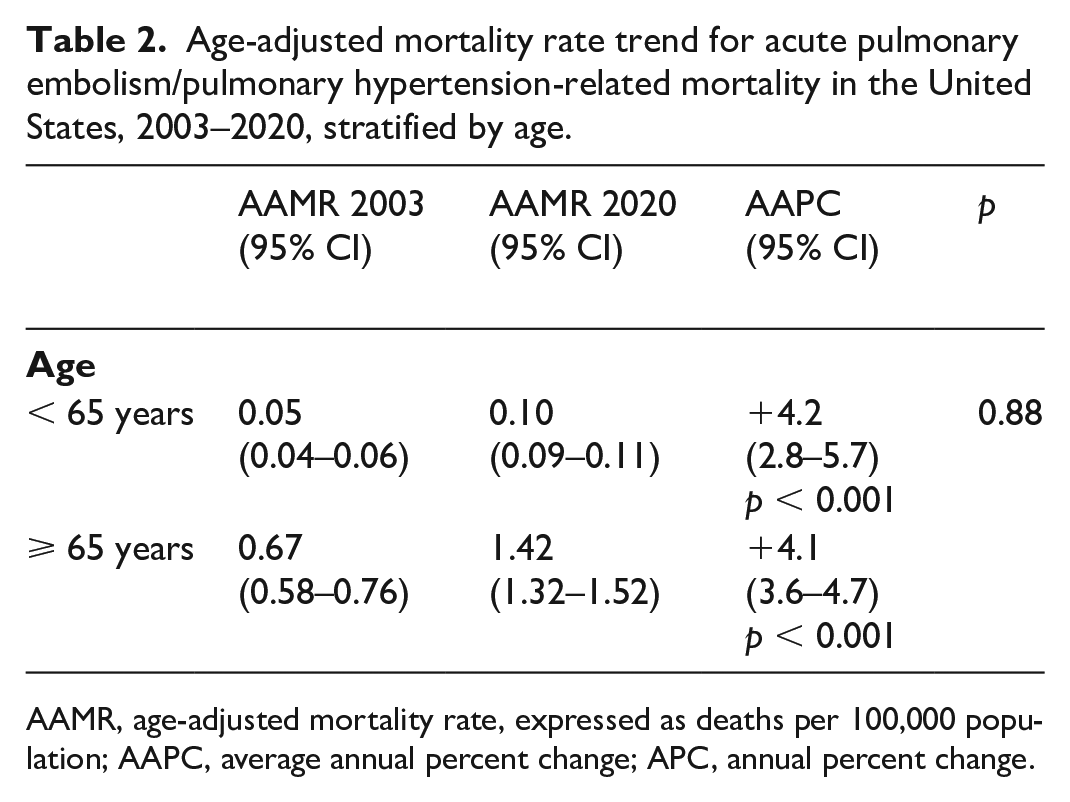
AAMR, age-adjusted mortality rate, expressed as deaths per 100,000 population; AAPC, average annual percent change; APC, annual percent change.
Urbanization and census region patterns
Over the study period, the AAMR for PE/PH-related deaths showed a similar increase in both rural (AAPC: +5.1% [95% CI: 3.8 to 6.4], p < 0.001) and urban areas (AAPC: +3.9 [95% CI: 3.1 to 4.8], p < 0.001) (p for parallelism 0.22) (Table 3 and Figure 2). The percentages of PE/PH-related deaths, however, were higher in the South compared with other census regions (Supplementary File 1).
Age-adjusted mortality rate trend for acute pulmonary embolism/pulmonary hypertension-related mortality in the United States, 2003–2020, stratified by urbanicity.
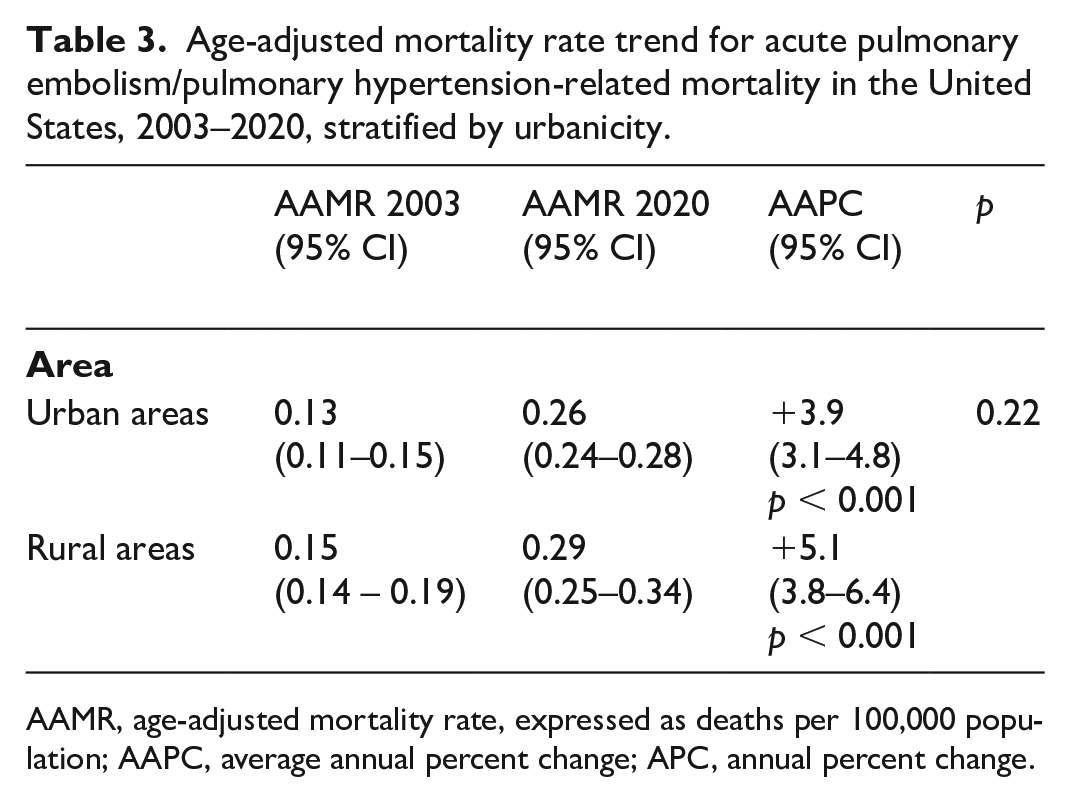
AAMR, age-adjusted mortality rate, expressed as deaths per 100,000 population; AAPC, average annual percent change; APC, annual percent change.
Underlying cause of death
The most common root causes of mortality in PE-related deaths in patients with concomitant PH (⩾ 1%) were chronic obstructive pulmonary disease (COPD) (n = 1272, 9.3%), interstitial lung disease (n = 515, 3.8%), acute myocardial infarction (n = 490, 3.6%), lung cancer (n = 345, 2.5%), and breast cancer (n = 134, 1.0%).
Impact of the COVID-19 pandemic
During 2020 (first year of the COVID-19 pandemic), 768 PE/PH-related deaths were registered in the US. Of these, 536 (69.7%) and 232 (30.3%) were recorded in individuals with and without SARS-CoV-2 infection, respectively. Specifically, the PE/PH-related AAMR was higher in individuals ⩾ 65 years, especially in those with SARS-CoV-2 infection. Moreover, the PE/PH-related AAMR in patients with COVID-19 was greater in women than in men (0.78; 95% CI 0.74 to 0.81 per 100,000 vs 0.69; 95% CI 0.66 to 0.73 per 100,000). Both Black and White individuals with COVID-19 infections had the highest PE/PH-related AAMR. Furthermore, the PE/PH-related AAMR in patients with COVID-19 was greater in subjects living in rural areas, as well as in those living in the West and Midwest, compared with those living in metropolitan areas and other census regions, respectively (Table 4).
Age-adjusted mortality rate trend for pulmonary embolism (PE)-related mortality in patients with concomitant pulmonary hypertension (PH) in the United States, among subjects with and without COVID-19.

Estimates were too low to perform dedicated sub-analyses for Asian/Pacific Islanders and American Indians/Alaska natives. However, such estimates were included in the analysis stratified for sex, urbanicity, and census regions.
AAMR, age-adjusted mortality rate, expressed as deaths per 100,000 population.
Discussion
The present study provides US nationwide estimates of PH-related mortality in patients with PE from 2003 to 2020 and demonstrates that, over the past 17 years, the AAMR in patients with PE and concomitant PH significantly increased. PH contributed to PE-related mortality in 1.9% of cases, which is a small but not negligible population. Though there was variability in the initial AAMR both by sex and by age, the AAMR trend from 2003 to 2020 in these cohorts followed similar patterns without significant differences by subgroup. When trends were examined by race and ethnicity, the greatest increase in mortality was observed among White individuals, despite a notable increase in the APC in Black individuals after 2008. By urbanization, there were similar AAMR increases in PH-related deaths in patients with PE in both urban and rural areas. There was a higher percentage of PE/PH-related deaths in the South compared to other geographical census regions. Finally, the COVID-19 pandemic generated a significant mortality increase in patients with PE and concomitant PH.
To the best of our knowledge, this is the first investigation assessing the PE/PH-related nationwide mortality rates over a prolonged, contemporary period. There are several possible explanations for the observed trends. Firstly, evolution in diagnostic testing and accuracy—for example, there has been a well-documented increase in the use of echocardiography over recent years that may have contributed to the increased recognition of acute PE and nonpulmonary arterial hypertension (PAH), along with increased awareness of both conditions.24,25 The true prevalence of PH is not known and the landscape of PH itself has also shifted, with increasing incidence of both PAH and non-PAH PH noted over recent years. 26 Of note, common underlying causes of death, such as COPD, interstitial pulmonary disease, or cancer could have contributed to the AAMR rise as well as to a delayed PE and/or PH diagnosis. Furthermore, the AAMR trends that were observed in this analysis were likely also driven by shifting epidemiologic risk factors for both PH and PE. Older age, for example, is a risk factor for both conditions and the continued aging of the US population has therefore likely contributed to increased prevalence of both PE 15 and PH. 26 Additionally, patients with PE with concomitant PH during the acute phase of the disease are typically older compared with those without. 27 Additional risk factors such as obesity have likely contributed, given the association of increased body mass index with a higher risk of acute PE, PH, and subclinical RVD.28–30
Based on these considerations, the trend for the observed increasing mortality rate seems to reflect a true increase in disease incidence. Alternative explanations, however, warrant consideration. Increased adoption of multidisciplinary PE response teams may have driven greater recognition of PE as a cause of death and may also increase utilization of cardiovascular imaging—such as echocardiography for risk stratification—that may assist in both PH and PE diagnoses. Regardless of whether PH existed before acute PE or resulted from the PE, the combination of PE plus PH constitutes a particularly ominous relationship associated with a higher mortality risk. 31 Moreover, in the acute setting, the distinction between an acute PE with PH and an ‘acute on chronic’ PE with concomitant PH remains challenging and represents a potential cause of misdiagnosis and treatment delay. 32 Further analyses are needed to identify novel treatment modalities for patients with simultaneous PE and PH.
Increasing recognition of social determinants of health has shed light on the widespread disparities in PE and PH diagnosis and management between ethnoracial and geographic subgroups.33–35 In the current analysis, White individuals had a higher AAMR increase in PE/PH-related mortality, although there was an increasing trend in the APC among Black patients starting in 2008. The differential prevalence of cardiovascular risk factors, incidence of cardiovascular events, risk factors for venous thromboembolism (VTE), and access to healthcare are likely to be contributors of the increasing trend in this demographic group.36,37 Because Black patients have a higher PE-related mortality rate, it is also possible that they may have died suddenly before being diagnosed with PH.38,39
A similar increase in PH-related deaths in patients with PE was observed in subjects living in both urban and rural areas, although the absolute AAMR was greater in rural areas. This trend echoes prior findings in PH demonstrating a general rise in AAMR in both settings, with overall increased mortality in the rural population. 40 Though the overall trend likely reflects the shifting epidemiology in the US population, the specific urban–rural discrepancy may be related to regional-specific risk factors and management. Access to PH specialty management may be challenging in rural areas, which may further exacerbate difficulty in treating certain forms of PH in which therapeutic options are limited. 41 Furthermore, care delivered in rural regions may be further complicated by a decreased availability of advanced PE strategies including catheter-based reperfusion treatment as well as differential awareness and risk factors for cardiovascular disease. 41 The increasing prevalence of some conditions associated with secondary PH, such as valvular heart disease, left-sided heart failure, COPD, and restrictive lung disease have probably influenced the epidemiology of PH and impacted mortality. Such concomitant conditions have also been associated with disparities based on race, regional location, and ethnicity.41,42
The increased trend in mortality among patients with PE/PH in rural areas and the South may be due to several factors, including poor cardiopulmonary health and limited access to advanced treatments. 40 Conversely, in urban areas, increasing pollution, drug abuse, and exposure to environmental toxicants may increase the prevalence of PE and PH associated with certain conditions such as lung disease, culminating in an increased risk of mortality.43,44
Finally, the higher AAMR in patients with PE/PH and COVID-19 that was observed in the present analysis is in accordance with data offered by recent studies. In hospitalized patients with PH, SARS-CoV-2 infection is associated with severe consequences. 45 Similarly, a large analysis based on the National Inpatient Sample (NIS) revealed that patients with COVID-19 and PH had a higher risk of acute PE and myocardial infarction during hospitalization. 46 Moreover, after multivariate adjustment, patients with COVID-19 with concomitant PH experienced considerably higher in-hospital mortality, longer hospital stays, and higher costs of hospitalization when compared to patients with COVID-19 without PH. 46
Limitations
Our study has several limitations. Consistent with real-world clinical practice, it remains often difficult to categorize patients with concomitant heart and lung disease using only ICD-10 codes, such that we were unable to group PH by the current WHO classification system. Data regarding the temporal relationship between PE, PH, and mortality were not provided by the CDC WONDER dataset, precluding the assessment of PH temporality with respect to the PE diagnosis. However, this closely mirrors the common clinical conundrum faced by many regarding the temporal relationship of the PH to the PE, which often remains unclear because of the presence of other comorbid conditions that may contribute to PH and lack of prior assessments of pulmonary artery pressures. 47 Furthermore, being able to provide data regarding outcomes in such patients is potentially informative given the frequency of this clinical challenge. Regardless of the cause, the management of patients with PE and PH remains problematic and challenging. 44 Furthermore, like any study relying on large nationwide administrative databases, we cannot exclude potential miscoding and/or misclassification which may have impacted the accuracy of our results. Moreover, the CDC WONDER dataset did not report any data regarding the previous cardiovascular history, functional heart status, or information regarding the possible competing causes of death, further limiting our analysis. Observational cohort studies suggest that the proportion of subsegmental disease relative to overall PE is increasing. Accordingly, within the context of the limitations of the CDC WONDER dataset, we cannot exclude that a proportion of the patients in this analysis had subsegmental PE and that the association of this diagnosis with PH and mortality would be less clear. 48 Though the use of ICD-10 codes may be associated with intrinsic limitations and potential biases, and the CDC WONDER dataset did not allow for independent validation, previous investigations based on both the US population and other countries have shown an acceptable accuracy of ICD-10 codes for PH, with specificities and negative predictive values > 97.5%.15,17
Conclusions
The rate of PE/PH-related mortality in the US appears to be increasing. Although the early diagnosis of PH in patients with acute PE has become easier with improved access to echocardiography, there remains significant variation in mortality between demographic populations, urban versus rural care settings, and US geographic locations. The observed trends may be influenced, at least in part, by social determinants of health, disparities in care delivery, differences in cardiovascular risk, and prevalence of underlying comorbid conditions. Further investigation to better characterize and understand PE/PH mortality trends, in particular the temporal relationship of PH to the PE and associated outcomes, is needed to help direct management and guide therapy.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241257165 – Supplemental material for Pulmonary hypertension-related deaths in patients with acute pulmonary embolism in the United States, 2003 to 2020
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241257165 for Pulmonary hypertension-related deaths in patients with acute pulmonary embolism in the United States, 2003 to 2020 by Marco Zuin, Roberto Badagliacca, Eileen Harder, Bridget McGonagle, Christie Greason and Gregory Piazza in Vascular Medicine
Footnotes
Data availability statement
Declaration of conflicting interests
Gregory Piazza received research support from Bristol-Myers Squibb/Pfizer Alliance, Bayer, Janssen, Alexion, Amgen, and Boston Scientific Corporation, and consulting fees from Pfizer, Boston Scientific Corporation, Janssen, and Amgen. The other authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.