
Abstract
Incidental pulmonary embolism (IPE) is defined as pulmonary embolism (PE) discovered on imaging studies performed for indications other than suspected PE. 1 Although thrombus burden tends to be lower in IPE than in symptomatic PE (SPE),2,3 several observational studies have shown that the clinical significance of IPE is comparable to that of SPE in terms of mortality and recurrence. 1 Most of the published studies on IPE have been conducted on cancer patients. 1 Although IPE can also be found in noncancer patients, the clinical significance of IPE in these patients is not well understood yet. 1 Thus, the aim of this retrospective study was to evaluate clinical characteristics and outcomes of IPE compared with SPE in noncancer patients.
Data were obtained from the medical records of adult patients who were hospitalized with PE diagnosed using multidetector-row computed tomography (CT) between January 2003 and December 2020 at Kyungpook National University Hospital (KNUH), a tertiary referral center in Daegu, South Korea. For patients who had PE in our department or were referred for PE from other departments, we retrospectively analyzed their entire electronic medical records. This study was approved by the Institutional Review Board of KNUH.
Based on the previous recommendations, 4 patients diagnosed with PE on CT performed for reasons other than a clinical suspicion of PE were allocated to the IPE group. Those who underwent CT to assess the presence of PE suspected as a primary differential diagnosis were allocated to the SPE group. IPE versus SPE was determined by reviewing medical records at the time of PE diagnosis. Clinical and radiologic characteristics of noncancer patients with IPE and SPE were then compared.
As described in a previous study, 5 PE-related in-hospital death was defined as in-hospital death with objective evidence that PE was a direct cause of death or death that could not be attributed to other causes and PE could not be excluded. An adverse outcome, the outcome of interest of this study, was defined as a PE-related in-hospital death or a serious clinical condition caused by PE requiring intensive care treatments, such as inotropic support and mechanical ventilation, impending respiratory failure or refractory hypoxia, cardiopulmonary resuscitation, or secondary thrombolysis. Patients in whom PE or deep vein thrombosis recurred at our institution were considered to have had a venous thromboembolism (VTE) recurrence. Follow-up after the first hospitalization was determined at the discretion of the attending physician at the time. The final analysis of clinical characteristics and outcome was based on the first hospitalization event only. Outcome variables were determined by consensus by two chest physicians (YHL and SIC) after reviewing medical records. To examine the association between IPE and clinical outcomes after adjusting for potential confounders, multivariable logistic regression analysis using Firth’s penalized likelihood method was performed.
Among 1620 initially identified patients with PE, those with chronic thromboembolic pulmonary hypertension or in situ thrombosis, those without available chest CT results, and those who were treated in outpatient settings were excluded (online supplementary material: Figure S1). After further excluding patients with cancer, the remaining 1220 patients were divided into IPE and SPE groups. The results of comparing clinical and radiologic parameters between IPE and SPE groups are presented in Table 1. Surgery or trauma and immobilization were more frequently identified in the IPE group than in the SPE group (p < 0.001). The proportion of patients with a high PESI score in classes IV–V and with central PE and right ventricular (RV) dilation on CT were all significantly lower in the IPE group (p < 0.001). In terms of clinical outcomes, there were significantly fewer patients with adverse outcomes (p < 0.001) and VTE recurrence (p = 0.004) in the IPE group compared with the SPE group. However, in multivariable analysis, IPE was significantly associated with a lower risk of adverse outcomes compared to SPE (p = 0.001), whereas it was not for VTE recurrence (p = 0.494; online supplementary material: Table S1).
Baseline and clinical characteristics of pulmonary embolism in patients without cancer (n = 1220).
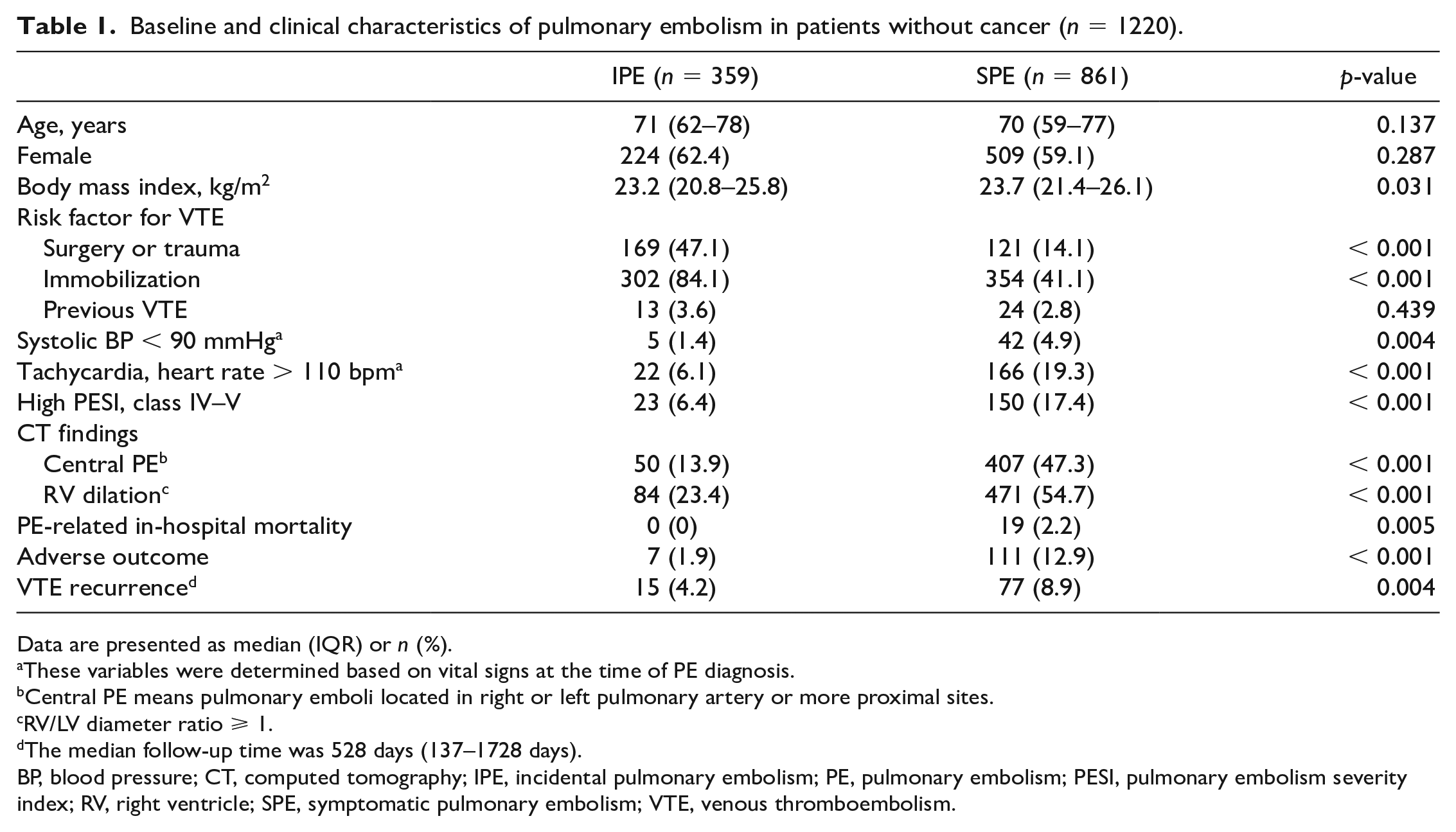
Data are presented as median (IQR) or n (%).
These variables were determined based on vital signs at the time of PE diagnosis.
Central PE means pulmonary emboli located in right or left pulmonary artery or more proximal sites.
RV/LV diameter ratio ⩾ 1.
The median follow-up time was 528 days (137–1728 days).
BP, blood pressure; CT, computed tomography; IPE, incidental pulmonary embolism; PE, pulmonary embolism; PESI, pulmonary embolism severity index; RV, right ventricle; SPE, symptomatic pulmonary embolism; VTE, venous thromboembolism.
Approximately 29% of the patients were diagnosed incidentally with PE, which was somewhat consistent with a recent study by Wysokinska et al. where IPE accounted for 23% of noncancer patients with PE. 6 These findings suggest that the incidence of IPE could be non-negligible in noncancer patients. Many patients in the IPE group of our study had provoking risk factors, including immobilization, surgery, and trauma. At our institution, surgical patients with trauma such as fractures often routinely underwent CT scans for VTE surveillance, even in the absence of specific symptoms and signs. These patients might have undergone CT more frequently than other patients. Thus, PE was more likely to be detected incidentally.
Few studies have reported clinical outcomes of IPE in noncancer patients. The study by Wysokinska et al. has compared IPE and SPE in patients with or without cancer, 6 with the IPE group showing a higher mortality than the SPE group in noncancer patients. In that study, nevertheless, the death rate at 3 months, suggestive of short-term prognosis, was not significantly different between IPE and SPE patients. On the other hand, in the current study, the IPE group had lower PESI scores and less frequent central PE and RV dilation on CT, indicating a less severe form of PE, which was also significantly associated with a lower risk of adverse outcome. For the risk of VTE recurrence in our study, there was no significant difference between IPE and SPE, which was similar to the study by Wysokinska et al. 6 These subtle discrepancies in the results on the prognostic impact of IPE in noncancer patients need to be validated in future research. Since this retrospective study was conducted with data from a single center, selection bias was inevitable. The potential effect of in-hospital treatment for PE on outcome was not considered. The lack of information on overall survival is another limitation.
In conclusion, in this cohort of PE patients without cancer, IPE was associated with a significantly lower risk of adverse outcomes compared to SPE.
Supplemental Material
sj-docx-2-vmj-10.1177_1358863X231171614 – Supplemental material for Incidental versus symptomatic pulmonary embolism in patients without cancer
Supplemental material, sj-docx-2-vmj-10.1177_1358863X231171614 for Incidental versus symptomatic pulmonary embolism in patients without cancer by Yong Hoon Lee, Seung-Ick Cha, Jongmin Park, Jae Kwang Lim, Won Kee Lee, Ji-Eun Park, Sun Ha Choi, Hyewon Seo, Seung-Soo Yoo, Shin-Yup Lee, Jaehee Lee, Chang-Ho Kim and Jae-Yong Park in Vascular Medicine
Supplemental Material
sj-tif-1-vmj-10.1177_1358863X231171614 – Supplemental material for Incidental versus symptomatic pulmonary embolism in patients without cancer
Supplemental material, sj-tif-1-vmj-10.1177_1358863X231171614 for Incidental versus symptomatic pulmonary embolism in patients without cancer by Yong Hoon Lee, Seung-Ick Cha, Jongmin Park, Jae Kwang Lim, Won Kee Lee, Ji-Eun Park, Sun Ha Choi, Hyewon Seo, Seung-Soo Yoo, Shin-Yup Lee, Jaehee Lee, Chang-Ho Kim and Jae-Yong Park in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.