
Abstract
Exposure to uninterrupted prolonged sitting leads to macro- and microvascular complications, which can contribute to increased cardiovascular disease risk. This study investigated the macrovascular and microvascular responses to 3 h of sitting that was: (i) uninterrupted (CON); and (ii) interrupted every 20 min with 1 min light intensity half squats plus calf raises (EX). Twenty healthy participants (21 [SD: 2] years; 21.5 [SD: 1.6] kg/m2) were recruited to participate in this randomized cross-over trial. Macrovascular function was quantified using brachial–ankle pulse wave velocity (baPWV) and the lower- and upper-limb arterial stiffness index (ASI). Microvascular function was quantified as the medial gastrocnemius tissue oxygen saturation (StO2) area under the curve (AUC) during reactive hyperemia. The baPWV did not significantly change with time (p = 0.594) or by condition (p = 0.772). The arm ASI increased by 3.6 (95% CI: 0.7 to 6.6, effect size [ES] = 0.27) with a nonsignificant condition effect (p = 0.219). There was a significant interaction effect for leg ASI (p = < 0.001), with ASI increasing (impairment) by 18.7 (95% CI: 12.1 to 25.3, ES = 0.63) for CON and decreasing (improvement) by −11.9 (95% CI: −18.5 to −5.3, ES = 0.40) for EX compared to presitting. Similarly, the AUC decreased (detrimental) by 18% (Δ = −321, 95% CI: −543 to −100, ES = 0.32) for CON and increased by 32% (Δ = 588, 95% CI: 366 to 809, ES = 0.59) for EX. The leg ASI was inversely associated with StO2 AUC (interclass correlation coefficient: −0.66, 95% CI: −0.51 to −0.77). These preliminary findings suggest that regularly interrupting prolonged sitting with simple bodyweight exercises may help to preserve lower-limb vascular function.
Introduction
Simple strategies are needed to break-up prolonged sitting and mitigate the negative macrovascular and microvascular effects associated with increased cardiovascular disease risk.1–8 For example, four studies have measured the central arterial stiffness response to prolonged sitting,5–8 of which three incorporated a sitting interruption strategy.5,7,8 Standing every 30 min was reported to mitigate the increased arterial stiffness, 5 but calf-raise exercises while remaining seated (i.e., less work load) 7 and resistance exercises 8 were ineffective. However, it should be considered that the resistance exercise trial interrupted sitting every 30 min, and the exercises alternated between upper-body and lower-body. 8 Considering prolonged sitting has been reported to impair lower-limb but not upper-limb macrovascular function, 9 targeting the lower limbs once per hour may have presented an insufficient stimulus. Further research is warranted to test the efficacy of simple resistance-based exercises to regularly (i.e., greater than once per hour) interrupt prolonged sitting.
This study investigated the macrovascular and microvascular responses to 3 h of sitting that was (i) uninterrupted (CON) and (ii) interrupted every 20 min with 1 min light intensity exercise (half squats) (EX). These bodyweight resistance exercises require minimal expertise, engage major muscle groups, and can be performed without equipment in the home or office setting. We hypothesized that regularly targeting the lower extremities with the minimally disruptive EX would preserve macrovascular and microvascular function compared to CON.
Methods
This study is reported according to Consolidated Standards of Reporting Trials (CONSORT) guidelines 10 and ethical approval was obtained by the Mount Fuji Research Institute (ECMFRI-02-2017). All participants provided written informed consent prior to participating in the study.
Participants
We recruited healthy men and women between the ages of 18 and 30 years using a digital and paper flyer in the local community (Kawaguchiko town and Fuji-yoshida site, Yamanashi, Japan) and the adjacent university (Health Science University). Exclusion criteria included pregnancy, stationary bike use, current smoker, any known cardiometabolic disorders, or use of medications known to affect cardiovascular health, and regular engagement in moderate-to-vigorous physical activity (⩾ 120 min/week). We excluded highly active individuals to ensure findings are generalizable to the target populations (those that are inactive and sedentary). Women were studied within the first 1–7 days of the onset of their menstrual cycle. 11 Participants were stratified by sex and randomly assigned to the starting condition using a lottery.
Experimental design
This study was a randomized, controlled cross-over trial with two experimental conditions (Figure 1): 3 h sitting (i) uninterrupted (CON) and (ii) interrupted every 20 min with 1 min of light intensity exercise (half squats) (EX). Participants reported to the laboratory on three occasions, including one familiarization with all measurement techniques (i.e., blood pressure [BP] measurement both in supine and sitting positions, near infrared spectroscopy [NIRS] measurement including cuff occlusion in the prone position, and bodyweight exercise) and two experimental visits. For each visit, separated by 2–4 days, participants arrived between 0700 and 1100 having fasted for 12 h, abstaining from strenuous physical activity and alcohol for 24 h, and refraining from supplement intake that morning. After emptying their bladder, height and body mass were measured. Next, participants rested supine while being fitted with BP cuffs around each limb, and the legs were placed in commercial vacuum packs to prevent leg movement (Vacform, Muranaka Medical Instruments Co., Ltd, Osaka, Japan). The cuffs were attached to the ArterioVision MS-3000 (Osachi Co., Ltd, Yamanashi, Japan) for the measurement of macrovascular and standard hemodynamic outcomes. NIRS probes (BOM-L1TRW, Omegawave, Tokyo, Japan) were fitted over the left medial gastrocnemius to assess microvascular function in the prone position. 12 Baseline macrovascular, microvascular, BP, and heart rate (HR) measures were collected in the supine posture following 20 min quiet rest, and postcondition measures were collected 5 min after being returned to the supine posture. BP and HR were additionally measured during each condition at 10 min, 60 min, 120 min, and 180 min.
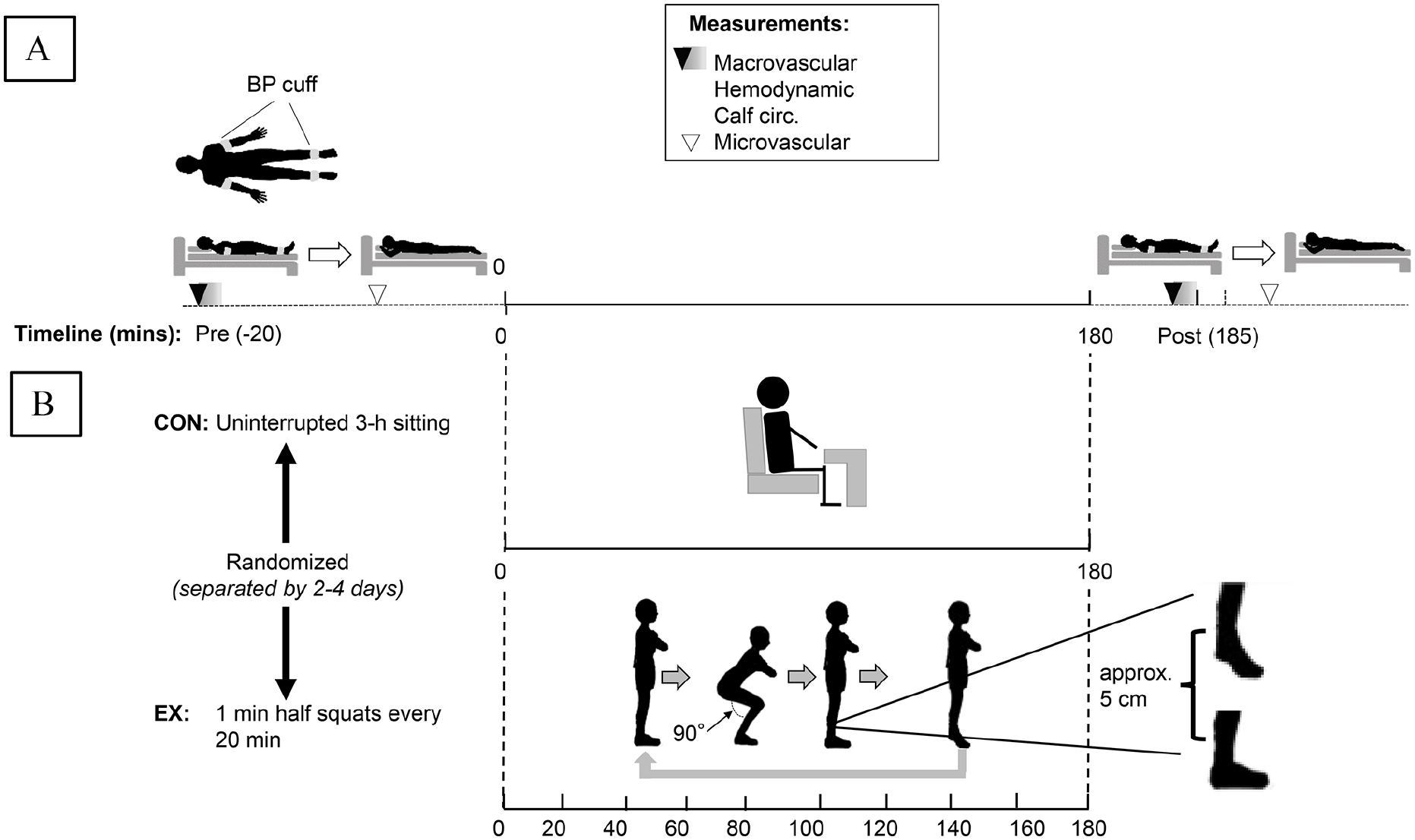
Overview of randomized, controlled cross-over trial with two 3 h experimental conditions: (i) uninterrupted sitting (CON) and (ii) interruptions with light intensity exercise (half squats) (EX).
Sitting condition
To minimize confounding due to movement/fidgeting during the 3 h sitting period, participants were asked to keep their arms and legs stationary, their feet were placed on a nonslip mat, and they were monitored throughout by study personnel. To maintain wakefulness, participants watched a nonstimulatory television program. This is because acute stress conditions affect sympathetic vasoconstrictor tone and BP 13 or positive emotional states (e.g., laughter) induce a beneficial impact on vascular function. 14
Light intensity exercise
For the EX condition, participants were asked to interrupt sitting with half squats every 20 min, performed for 1 min at 15 reps/min without pause between repetitions to avoid isometric muscle contractions. To perform a half squat, the participants did the following: (i) started in the standing position with arms crossed over their chest; (ii) bent their knees to 90 degrees; (iii) stood up again; (iv) immediately performed a calf raise (approximate 5 cm rise) without holding the contraction; and (v) repeated. With respect to the calf raise, during familiarization participants were asked to raise their heels from the ground to the limit of their own natural range of motion, which we measured as an approximate 5 cm rise across individuals.
Macrovascular function measurement
The ArterioVision device (OSACHI Co., Ltd) simultaneously measured brachial–ankle pulse wave velocity (baPWV; units: m/s) on each side of the body, and arterial stiffness index (ASI; units: arbitrary) in each limb, and BP and HR in each limb. 15 Measurements were made in duplicate, separated by 1 min. If the second BP value was > 5 mmHg to the first measurement, a third measure was collected, and the closest two measures were averaged. The baPWV was calculated by dividing arterial path length (D) by the pulse transit time (PTT) between the brachial and ankle arterial segment. The D was calculated by measuring the linear distance from the suprasternal notch to the mid-point of the ankle cuff and then subtracting the distance from the suprasternal notch to the mid-point of the brachial cuff. The PTT (as the time between the foot of the proximal pressure waveform to the foot of the distal pressure waveform) with the waveforms were recorded at a subdiastolic pressure (~50 mmHg). To measure ASI, a pressure sensor attached to the BP cuff was used to generate an oscillometrc curve by repeatedly measuring the arterial pulse amplitude as the cuff pressure was gradually reduced. As illustrated in Figure 2, the pressures at 100% and 80% of the peak arterial pulse amplitude were identified. Subsequently, ASI was calculated as the difference between these pressures multiplied by 10. Healthy, elastic arteries generate sharply peaked oscillometric curves (Figure 2A), and stiff arteries generate flat or multinotched peaks (Figure 2B).
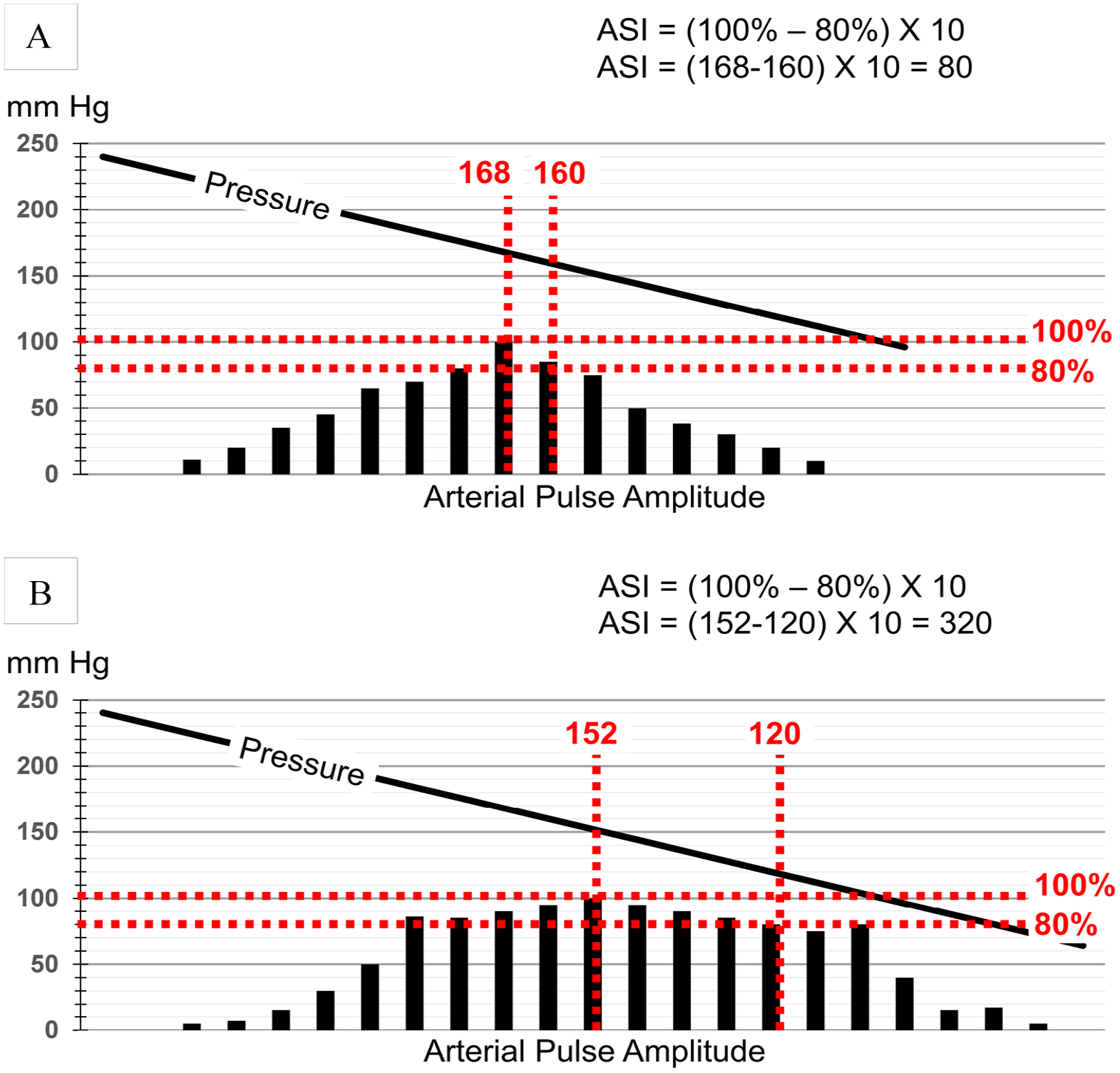
Illustration of arterial stiffness index (ASI) calculation (units: arbitrary). The diagonal line indicates cuff pressure. The pressures at 100% and 80% of the peak arterial pulse amplitude (i.e., the oscillometric curve over time [s]) are identified as vertical dashed lines. Subsequently, ASI is calculated as the difference between these pressures (100% – 80%) multiplied by 10. Healthy, elastic arteries generate oscillometric curves with sharp peaks.
Microvascular function measurement
Microvascular function was quantified as reperfusion rate (upslope; units: %∙s–1) and area under the curve (AUC; units: %∙s) of the medial gastrocnemius tissue oxygen saturation (StO2).12,16,17 The upslope was quantified during the first 10 s following cuff release and the AUC during the hyperemic phase. 12 Reactive hyperemia was induced by inflating a custom-built tourniquet reformed by a commercial device (Oscar 2 Ambulatory Blood Pressure Monitor; SunTech Medical, Inc., NC, USA) wrapped around the thigh to 220 mmHg for 5 min. 18 Measurements were made in duplicate, separated by 10 min, and the mean value was calculated. We confirmed that the resting baseline (preocclusion) value was apparent prior to initiation of the subsequent trial. 12
Sample size calculation
Sample size calculation was based on the baPWV arterial stiffness measure, for which we had the most comparable data for effect size estimation.6,7 We conservatively set the minimum within-subject detectable difference in baPWV at 0.30 m/s with an SD of 0.50 m/s. To detect a beneficial (or detrimental) effect at 80% statistical power with the maximum chances of a type-I error controlled at 5%, 19 participants were required.
Statistical analyses
Statistical analyses were performed using the R programming language (RKWard, version 0.7.2). Only participants who had complete data for the primary outcomes were included in the analyses. Raw data are presented as mean (SD) and mixed model data are presented as mean (95% CI). The corresponding author had full access to the data in the study and was responsible for the integrity of the data set and the data analyses. The α level was set a priori for main effects at 0.05, and for interaction effects at 0.10. Model assumptions were tested using Q-Q plots to diagnose normal distribution, and by plotting residual against fitted values to inspect bias.
The effects of time (pre vs post) and condition (CON vs EX) were analyzed using linear mixed models, with subject (intercept) specified as a random effect and time (slope), and condition specified as fixed effects. To limit within-subject variance, the models were adjusted for baseline values as specified by Kenward and Roger. 19 Effect size (ES) was calculated as Cohen’s d by the dividing β by the SD. An ES was defined as trivial (< 0.2), small (0.2), moderate (0.5), or large (0.8). 20
A series of linear mixed models was used to estimate the strength of association between leg microvascular and macrovascular function outcomes. The mixed-model approach maximizes statistical power while accounting for the correlated error variances. To calculate the overall measurement agreement, microvascular function was regressed against macrovascular function, with subject (intercept) specified as a random effect. Subsequently, the overall intraclass correlation coefficient (ICC) was calculated using the random variance components. To calculate repeated measures agreement (RM ICC) (i.e., the strength of the association for change in one measure versus change in the other measure), we used the rmcorr (repeated measures correlation) package for R. 21 The rmcorr statistical technique determines the overall within-individual relationship among paired measures assessed on two or more occasions. 21 Although there is no universal criterion for adjudicating the strength of a correlation, estimates were defined as negligible (< 0.2), weak (0.2), moderate (0.4), strong (0.7), or very strong (0.9). 22
Results
All 20 participants (50% women), aged 21 (SD: 2) years with a body mass index of 21.5 (SD: 1.6) kg/m2, completed both trials and there were no missing data. Data reported below are for measurements made in the supine position, except NIRS measurements in the prone position. The onlne supplementary material (Table S1) reports seated BP and HR data.
Hemodynamic data
With prolonged sitting HR increased 6.6% (Δ = 4.0 beats per min, 95% CI: 2.9 to 5.0, ES = 0.86), with a nonsignificant condition effect (p = 0.170) (Table 1). Mean arterial blood pressure (MAP) did not significantly change with time (p = 0.577) or by condition (p = 0.807), but pulse pressure decreased by 4.9% (Δ = −2.5 mmHg, 95% CI: −3.8 to −1.1, ES = 0.41) in the arms and 4.3% in the legs (Δ = −2.7 mmHg, 95% CI: −5.1 to −0.3, ES = 0.24), with nonsignificant condition effects. For calf circumference, there was a significant interaction effect (p < 0.001), with a 2.3% increase for CON (Δ = 0.82 cm, 95% CI: 0.71 to 0.94, ES = 1.60) and a 0.4% decrease for EX (Δ = −0.15 cm, 95% CI: −0.26 to −0.03, ES = 0.28).
Supine hemodynamic responses to two prolonged sitting (3 h) conditions.
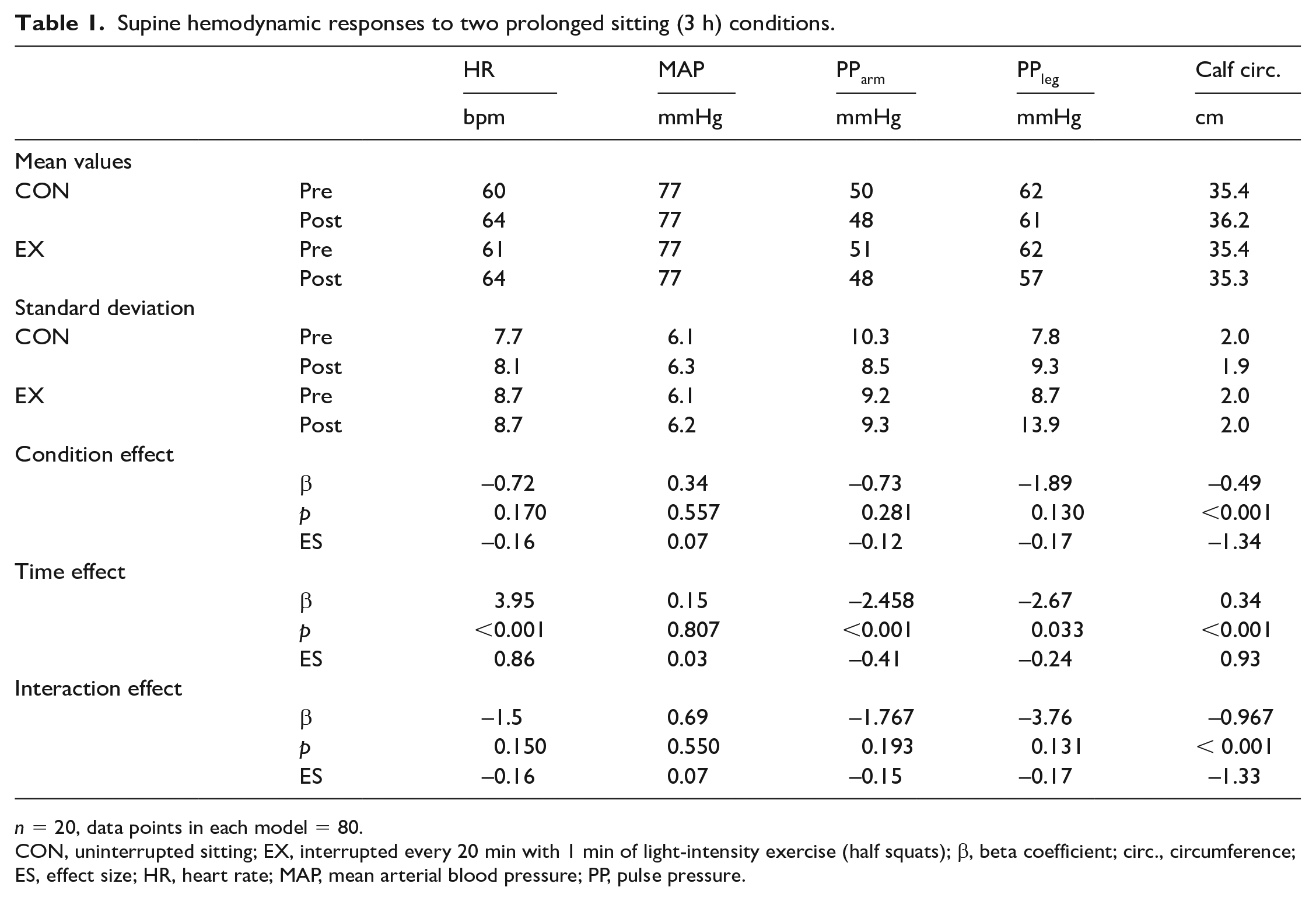
n = 20, data points in each model = 80.
CON, uninterrupted sitting; EX, interrupted every 20 min with 1 min of light-intensity exercise (half squats); β, beta coefficient; circ., circumference; ES, effect size; HR, heart rate; MAP, mean arterial blood pressure; PP, pulse pressure.
Macrovascular function
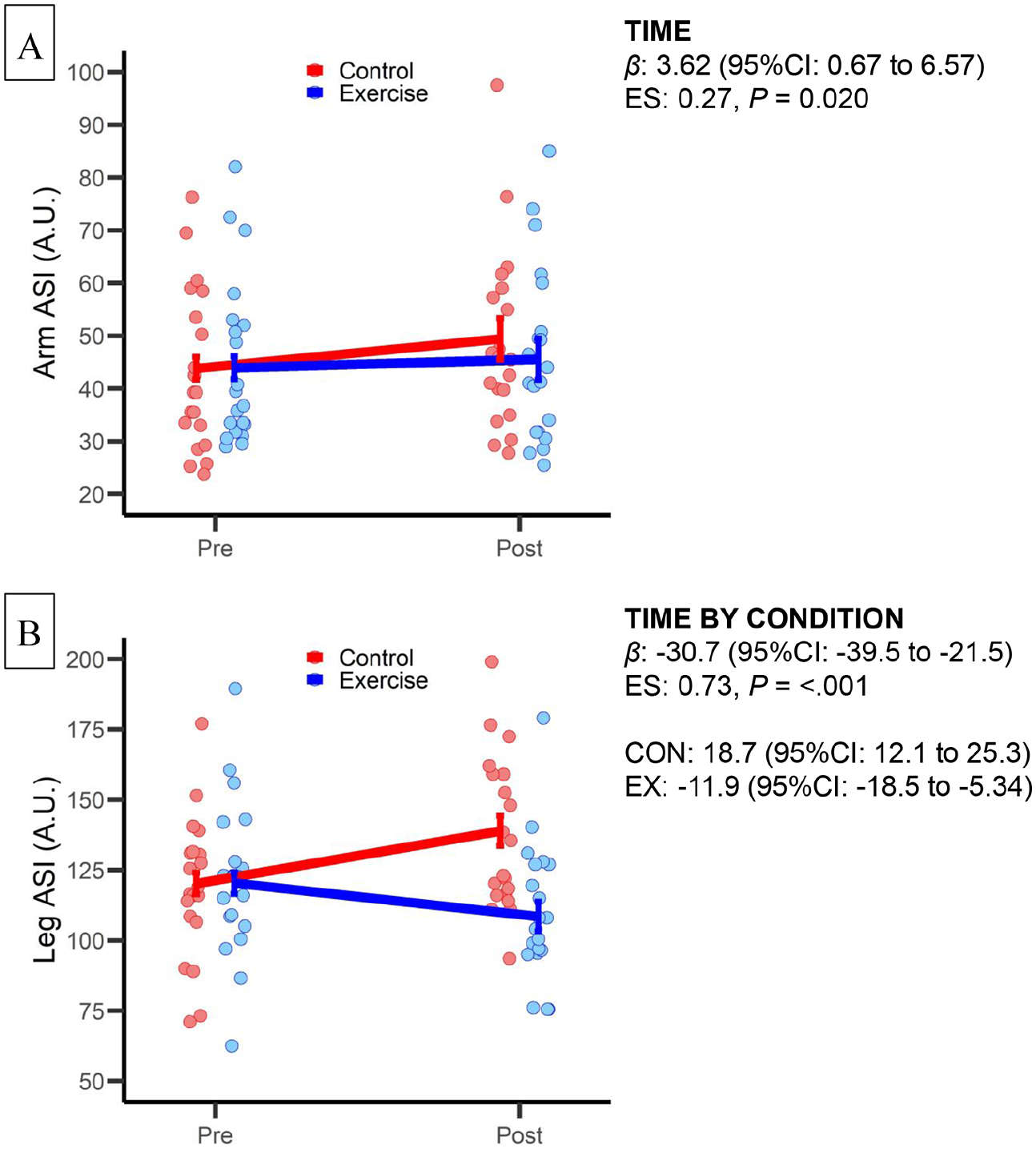
The baPWV did not significantly change with time (p = 0.594) or by condition (p = 0.772) (Table 2). The arm ASI increased by 8.2% (Δ = 3.6, 95% CI: 0.7 to 6.6, ES = 0.27; Figure 3A) with a nonsignificant condition effect (p = 0.219). There was a significant interaction effect for leg ASI (p < 0.001; Figure 3B), with ASI increasing by 15.6% (Δ = 18.7, 95% CI: 12.1 to 25.3, ES = 0.63) for CON and decreasing by 9.9% (Δ = −11.9, 95% CI: −18.5 to −5.3, ES = 0.40) for EX.
Supine macrovascular and microvascular responses to two prolonged sitting (3 h) conditions.
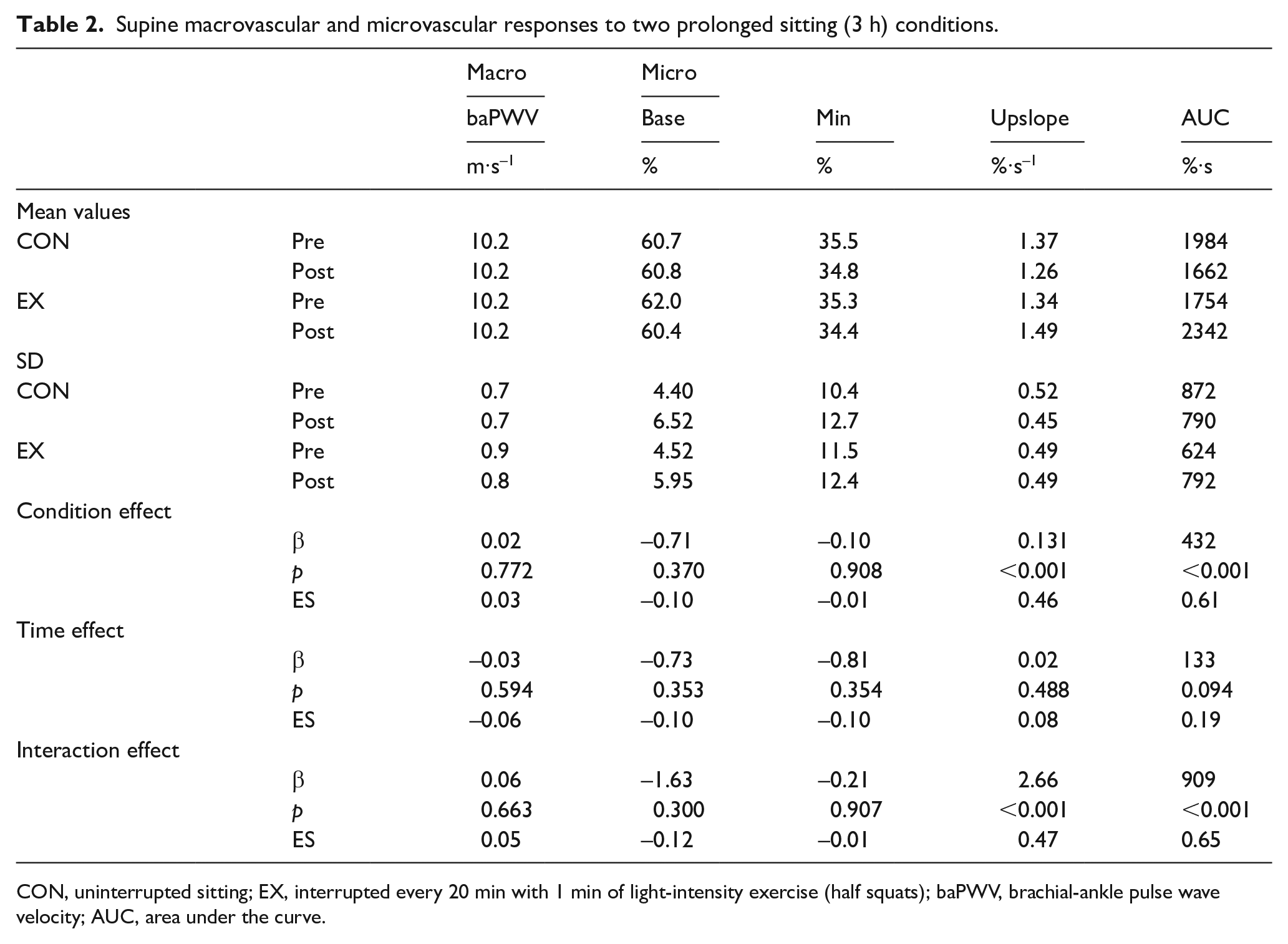
CON, uninterrupted sitting; EX, interrupted every 20 min with 1 min of light-intensity exercise (half squats); baPWV, brachial-ankle pulse wave velocity; AUC, area under the curve.
Supine arm
Microvascular function
There was a significant interaction effect for the StO2 AUC (p < 0.001), with the AUC decreasing 18% (Δ = −321, 95% CI: −543 to −100, ES = 0.32) for CON and increasing 32% (Δ = 588, 95% CI: 366 to 809, ES = 0.59) for EX. Similarly, there was a significant interaction effect for the StO2 upslope (p < 0.001), with the upslope decreasing 8.2% (Δ = −0.11, 95% CI: −0.20 to −0.02, ES = 0.28) for CON and increasing 114% (Δ = 0.16, 95% CI: 0.07 to 0.24, ES = 0.36) for EX (Table 2).
Relationship between macrovascular and microvascular function
The overall association between the two measures was moderate (ICC: −0.66, 95% CI: −0.77 to −0.51), and the repeated measure association was weak (RM ICC: −0.21, 95% CI: −0.44 to −0.04) (Figure 4A). The strength of the ICC and RM ICC associations were likely influenced by the direction of change for leg ASI and StO2 AUC differing by condition. When stratified by CON (Figure 4B) and EX (Figure 4C) the strength of the overall association increased for CON, and the repeated measures associations increased for both conditions.
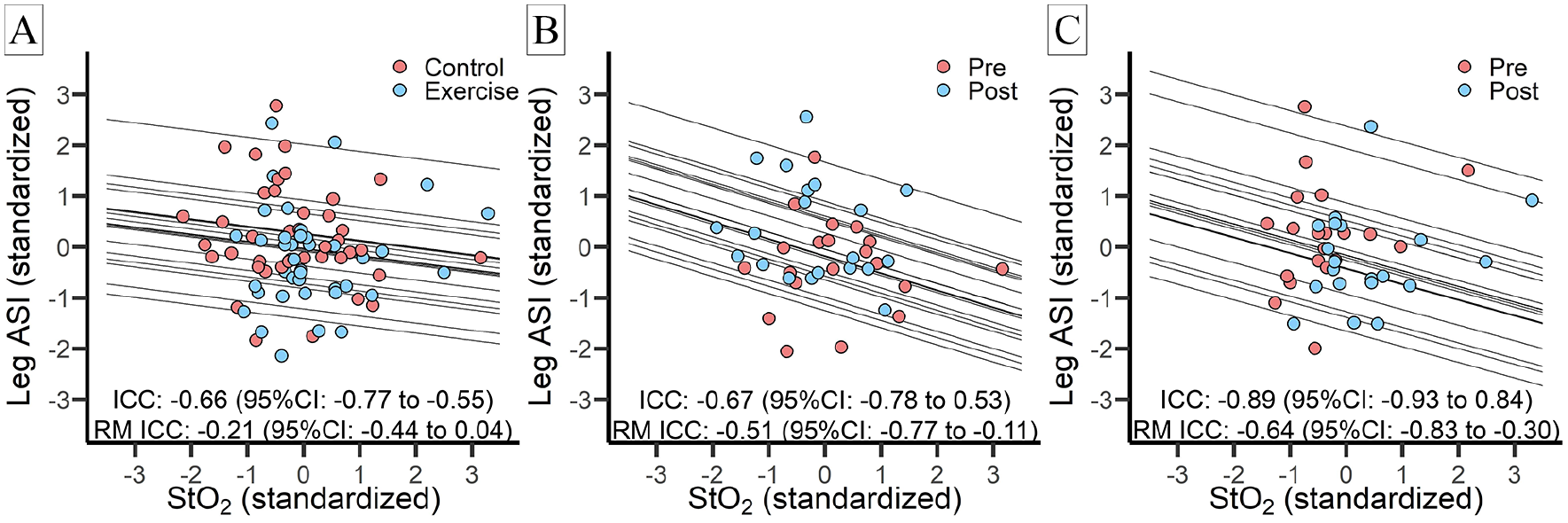
Associations between StO2 AUC and ASI.
Discussion
This study investigated if interrupting prolonged (3 h) sitting with light intensity exercise (half squats) mitigates declines in vascular function. The major findings are: (i) the interruption strategy prevented declines in leg macrovascular and microvascular function; (ii) there was a small effect size increase in arm macrovascular function (ASI) across conditions; and (iii) our index of global macrovascular function (baPWV) did not change with either condition. Collectively, our findings accord with previous reports of uninterrupted prolonged sitting preferentially and adversely targeting the lower-limb vasculature, and suggest that a simple interruption strategy with half squats may mitigate these adverse responses.
Comparison to the literature
Leg vascular function
The major finding of the current study is that our simple interruption strategy prevented declines in leg macrovascular (ASI) and microvascular (StO2 AUC and StO2 upslope) function. Specifically, for the uninterrupted condition there was a small–moderate effect size worsening of both indices, whereas for the interrupted condition there were small–moderate improvements. Additionally, we found a moderate association between change in microvascular and macrovascular function. Although associations between StO2 AUC and StO2 upslope with arterial stiffness have been reported, 12 the mechanisms responsible for the changes in microvascular and macrovascular function with prolonged sitting are not fully understood. It is likely that mechanisms responsible for the changes in mirco- and macrovascular function are multifactorial, including autonomic, hormonal, metabolic, and hemodynamic pathways. The hemodynamic pathway may play a particularly prominent role.
Hemodynamic changes may be led by blood pooling and, in the lower limbs, with subsequent decreased venous return. 18 The decreased venous return may lead to decreased cardiac output and contribute to the reported decrease in femoral artery blood flow-induced shear stress. 23 Shear stress is the key stimulus regulating endothelial function, and decreased shear stress through the leg arteries has been associated with a corresponding acute reduction in leg endothelial function. 24 The decrease in endothelial function would increase arterial stiffness, which depends on both the structural (e.g., vessel wall) 25 and functional (e.g., central autonomic and peripheral endothelial function)26,27 characteristics of the artery. The interruption strategy with half squats employed in the current study would activate the muscle pump, which is the major mechanism regulating venous return. Indeed, our results showed that increases in calf circumference (a measure of blood pooling)11,18 was reduced for EX compared with CON (Table 1). One caveat is that the blood pooling may have confounded our measurement of microvascular function, as venous congestion may have impeded the reactive hyperemic response. We did adjust our models for calf circumference, as a surrogate for venous pooling, but calf circumference was not a significant covariate and did not influence the findings.
Arm vascular function
Previous studies have reported prolonged sitting to impair lower-extremity but not upper-extremity vascular function.9,28 Although the effect size was small, our findings differ from these previous reports in that arm macrovascular function (ASI) was decreased across conditions. We speculate that our discrepant findings are attributable to differences in study design. Previous studies have not controlled the use of the arms,9,28 whereas the participants in the present study were strictly instructed not to move their upper arms while sitting. It is plausible that small arm movements maintain blood flow-induced shear stress, and therefore endothelial function. 9 To put the current findings into perspective, it is possible that permitting use of the arms is more ecologically valid, as many individuals may continue to use their arms while sitting, especially at work. Nonetheless, given the discordant findings, further investigation is warranted.
Global vascular function
Our index of global macrovascular function (baPWV) did not significantly change with either condition. Previous studies have reported decreased carotid-femoral (cf) PWV with prolonged sitting. However, although cfPWV and baPWV have previously been associated (r = 0.73 to 0.75),29,30 they do represent different latent constructs. The cfPWV is thought to primarily reflect the stiffness of the aorta, whereas the baPWV includes part of the brachial artery as well as the subclavian and leg arteries. As such, it is possible that whereas the aorta stiffened for participants in the current study, the differing responses in the brachial and femoral arteries (especially for EX) negated a detectable change. Further study is warranted to explore the effects of prolonged sitting on the stiffness of both lower- and upper-limb arteries and identify the importance of the interactions between these arterial segments to the myocardium and other end-organs.
Study strengths and limitations
The major strengths of this study include an internally robust design and our comprehensive assessment of vascular function. There are several limitations that should be considered to contextualize the findings. First, we purposely elected to recruit a small, homogeneous group of adults; therefore, whether the findings are generalizable across sex, different age groups, and cardiometabolic disease status may be limited. Our reasoning was that this recruitment would minimize the potential confounding of age and cardiometabolic diseases. Second, although we did exclude highly active individuals, we did not record sedentary behavior levels. We acknowledge that levels of daily sedentary behavior engagement may have differed between individuals, and future studies should consider the relative importance to habitual physical activity and sedentary behavior. Third, we did not measure sex hormones to enable more direct evaluation of the menstrual cycle, nor were we adequately powered to examine sex differences. Considering the positive outcomes of this study, further investigation is warranted to ascertain whether the findings are generalizable across sex, different age groups, and cardiometabolic disease status. Last, although our study protocol included 3 h of sitting, the average adult engages in closer to 8 h of sitting per day. 31 Further study is warranted to determine the effects of longer periods of uninterrupted sitting.
Conclusions
Prior to the current study it had been reported that uninterrupted prolonged sitting negatively affects vascular function, preferentially in the lower limbs.2–8 Repeated exposure to these acute insults likely leads to longer-term structural changes and increased cardiovascular disease risk. 1 Although national and international agencies now recognize the important health benefits of breaking-up sedentary behavior, no specific guidelines are provided.32,33 The current findings help to fill this gap in knowledge by reporting that a simple strategy to interrupt prolonged sitting, using half squats, prevents declines in lower-extremity vascular function.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X211053381 – Supplemental material for Macrovascular and microvascular responses to prolonged sitting with and without bodyweight exercise interruptions: A randomized cross-over trial
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X211053381 for Macrovascular and microvascular responses to prolonged sitting with and without bodyweight exercise interruptions: A randomized cross-over trial by Masahiro Horiuchi and Lee Stoner in Vascular Medicine
Footnotes
Acknowledgements
The authors would like to thank the participants for their time. We also thank Yasuyuki Yaguchi (OSACHI Co., Ltd, Nagano, Japan) and Daiki Shimura (SANYOSEIKO Co., Ltd, Yamanashi, Japan) for technical assistance with evaluating the arterial stiffness index, and Misato Watanabe (Mount Fuji Research Institute, Fuji-yoshida City, Yamanashi, Japan) for technical assistance with performing the experiment.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported in part by the Japan Society for the Promotion of Science (JSPS, KAKENHI, grant no. JP18K11012 to Dr Horiuchi).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.