
Abstract
There is a paucity of data on the outcomes and revascularization strategies for critical limb ischemia (CLI) among patients with chronic kidney disease (CKD). Hence, we conducted a nationwide analysis to evaluate the trends and outcomes of hospitalizations for CLI with CKD. The National Inpatient Sample database (2002–2015) was queried for hospitalizations for CLI. The trends of hospitalizations for CLI with CKD were reported, and endovascular versus surgical revascularization strategies for CLI with CKD were compared. The main study outcome was in-hospital mortality. The analysis included 2,139,640 hospitalizations for CLI, of which 484,224 (22.6%) had CKD. There was an increase in hospitalizations for CLI with CKD (Ptrend = 0.01), but a reduction in hospitalizations for CLI without CKD (Ptrend = 0.01). Patients with CLI and CKD were less likely to undergo revascularization compared with patients without CKD. CLI with CKD had higher rates of in-hospital mortality (4.8% vs 2.5%, adjusted odds ratio (OR) 2.01; 95% CI 1.93–2.11) and major amputation compared with no CKD. Revascularization for CLI with CKD was associated with lower rates of mortality (3.7% vs 5.3%, adjusted-OR 0.78; 95% CI 0.72–0.84) and major amputation compared with no revascularization. Compared with endovascular revascularization, surgical revascularization for CLI with CKD was associated with higher rates of in-hospital mortality (4.7% vs 2.7%, adjusted-OR 1.67; 95% CI 1.43–1.94). In conclusion, this contemporary observational analysis showed an increase in hospitalizations for CLI among patients with CKD. CLI with CKD was associated with higher in-hospital mortality compared with no CKD. Compared with endovascular therapy, surgical revascularization for CLI with CKD was associated with higher in-hospital mortality.
Keywords
Introduction
Critical limb ischemia (CLI) represents the advanced form of the peripheral artery disease (PAD) spectrum, with presentations ranging from rest pain to extensive gangrene in the affected limb.1,2 CLI is considered a grave diagnosis with associated morbidity and mortality exceeding other forms of occlusive atherosclerotic cardiovascular diseases.3,4 The prevalence of chronic kidney disease (CKD) is increasing in the overall population and is considered a fast-growing global health burden. 5 CKD is a major risk factor for PAD and is associated with a more extensive and progressive disease pattern of PAD. 6 That noted, data on the temporal trends and outcomes of CKD among patients with CLI remain scarce. In recent years, endovascular interventions for CLI are more commonly performed; yet the comparative outcomes of endovascular versus surgical revascularization among patients with CKD are not well understood. To address these knowledge gaps, we conducted a large nationwide analysis to evaluate the temporal trends and outcomes of hospitalization for CLI among patients with CKD.
Methods
Data source
The source for this study was the National Inpatient Sample (NIS) database. The NIS is part of the Healthcare Cost and Utilization Project (HCUP), and is considered the largest inpatient database in the US. It comprises clinical data obtained from discharge abstracts by hospitals to statewide data organizations across the US. Unweighted, the NIS contains > 7 million annual hospitalizations, and by using weighted samples it can provide national estimates of hospital admissions across the US. 7 Data from the NIS have been used to describe national estimates of health care utilization, access, charges, quality, and outcomes.8–10 The NIS reports data using the International Classification of Diseases, Ninth Edition (ICD-9) until September 2015; afterwards data are reported using the ICD-10 coding system. Data from the NIS are publicly available and de-identified; thus, this study was exempt from the institutional review board.
Study population and outcome measures
We queried the NIS database years 2002–2015 for patients’ hospitalizations with primary ICD-9 diagnostic codes for CLI (online Supplemental Table 1). 9 These ICD-9 codes identify patients with PAD who were admitted primarily for lower extremity ulceration, resting pain, or gangrene. Patients with CKD were identified using ICD-9 Clinical Modification (CM) codes 585.1 (CKD stage 1), 585.2 (CKD stage 2), 585.3 (CKD stage 3), 585.4 (CKD stage 4), 585.5 (CKD stage 5), and 585.9 (unspecified CKD stage). CKD stages are based on glomerular filtration rate (GFR) and are defined as: stage 1 (GFR ⩾ 90 mL/min/1.73 m2); stage 2 (GFR 60–90 mL/min/1.73 m2); stage 3 (GFR 30–60 mL/min/1.73 m2); stage 4 (GFR 15–30 mL/min/1.73 m2); and stage 5 (GFR < 15 mL/min/1.73 m2). The ICD-9 CM codes for CKD have been previously demonstrated to have a sensitivity of 81.9% and specificity of 98.6%, positive predictive value of 77.1%, and negative predictive value of 99.2%. 11 We excluded cases with end-stage renal disease (ICD-9 CM 585.6) or those on chronic dialysis (online Supplemental Table 1) as well as cases with missing data on the status of CKD or study outcomes. We identified patients undergoing revascularization using ICD-9 procedure codes for endovascular revascularization (peripheral balloon angioplasty, atherectomy or stent placement), surgical revascularization and combined endovascular/surgical (i.e., hybrid) revascularization (online Supplemental Table 1). 12 We analyzed the data for 2015 by quarter, and discontinuity in the frequency of available study variables was identified across ICD-9 and ICD-10 coding systems. Therefore, only ICD-9 codes were utilized and data beyond September 2015 were not included. 13 Per HCUP recommendations, we have conducted trend analysis for the year 2015 by dividing the observed frequencies in the first three quarters by 0.75 to yield annual estimates. 13
We reported the temporal trends in hospitalizations, in-hospital mortality, and revascularization modalities among those with CKD versus those without CKD. We also evaluated the outcomes for hospitalizations with CLI and CKD versus no CKD, and the outcomes of endovascular-only versus surgical-only revascularization approaches in CKD. The main study outcome was all-cause in-hospital mortality. The secondary outcomes included major amputation, minor amputation, postoperative infection, postoperative hemorrhage, acute stroke, acute myocardial infarction (MI), acute kidney injury (AKI), discharge to skilled nursing facility, and length of hospital stay. Procedures, clinical characteristics, and inpatient outcomes were abstracted and reported using ICD-9, Clinical Classifications Software (CCS) codes and Elixhauser comorbidities as reported by HCUP (online Supplemental Table 1).
Statistical analysis
We used linear regression analysis to evaluate the temporal trends in hospitalizations for CLI. 14 We conducted a multivariable regression analysis to adjust for in-hospital outcomes of CLI in CKD versus without CKD. Other multivariable regression models were also performed to compare the outcomes of endovascular-only versus surgical-only revascularization, as well as any-revascularization versus no-revascularization approaches for patients with CLI and CKD. The models included the following patient and hospital variables: age, sex, race, hypertension, diabetes mellitus, obesity, history of heart failure, chronic lung disease, pulmonary circulation disorders, chronic liver disease, chronic anemia, coagulopathy, hypothyroidism, history of smoking, coronary artery disease, prior MI, history of implantable cardiac defibrillator, history of cardiac pacemaker, prior stroke, prior percutaneous coronary intervention (PCI), prior coronary artery bypass grafting (CABG), hospital bed-size, hospital region, and hospital teaching status. In the multivariable regression model for CLI with CKD versus without CKD, we also included undergoing revascularization in the model.
All analyses were conducted using complex sample analysis and appropriate weighting samples to account for hospital clustering, weights, and stratification in accordance with the regulations of HCUP. We compared categorical variables using the chi-squared test, while continuous variables were compared using the Student’s t-test or Mann–Whitney U-test depending on the distribution curve. We reported categorical valuables as frequencies and percentages, while continuous variables were reported as mean ± SD or median and IQR depending on the distribution curve. Associations were considered significant if the p-value was ⩽ 0.05. We used SPSS software, Version 24.0 (IBM Corp., Armonk, NY, USA) for all statistical analyses.
Results
Study cohort
The initial analysis yielded 2,400,778 hospitalizations with a primary admission diagnosis of CLI from 2002 to 2015. After excluding cases with end-stage renal disease or on chronic dialysis (n = 235,956), missing data on CKD status (n = 24,851) or study outcomes (n = 331), the final analysis included 2,139,640 hospitalizations: 484,224 (22.6%) with CKD and 1,655,416 (77.4%) without CKD (Figure 1). Overall, those with CKD were less likely to receive any revascularization during the index admission (30.8% vs 36.6%, p < 0.001). Compared to those without CKD, patients who had CKD were more likely to receive endovascular revascularization (18.2% vs 14.1%, p < 0.001), and less likely to receive surgical revascularization (8.8% vs 15.0%, p < 0.001).
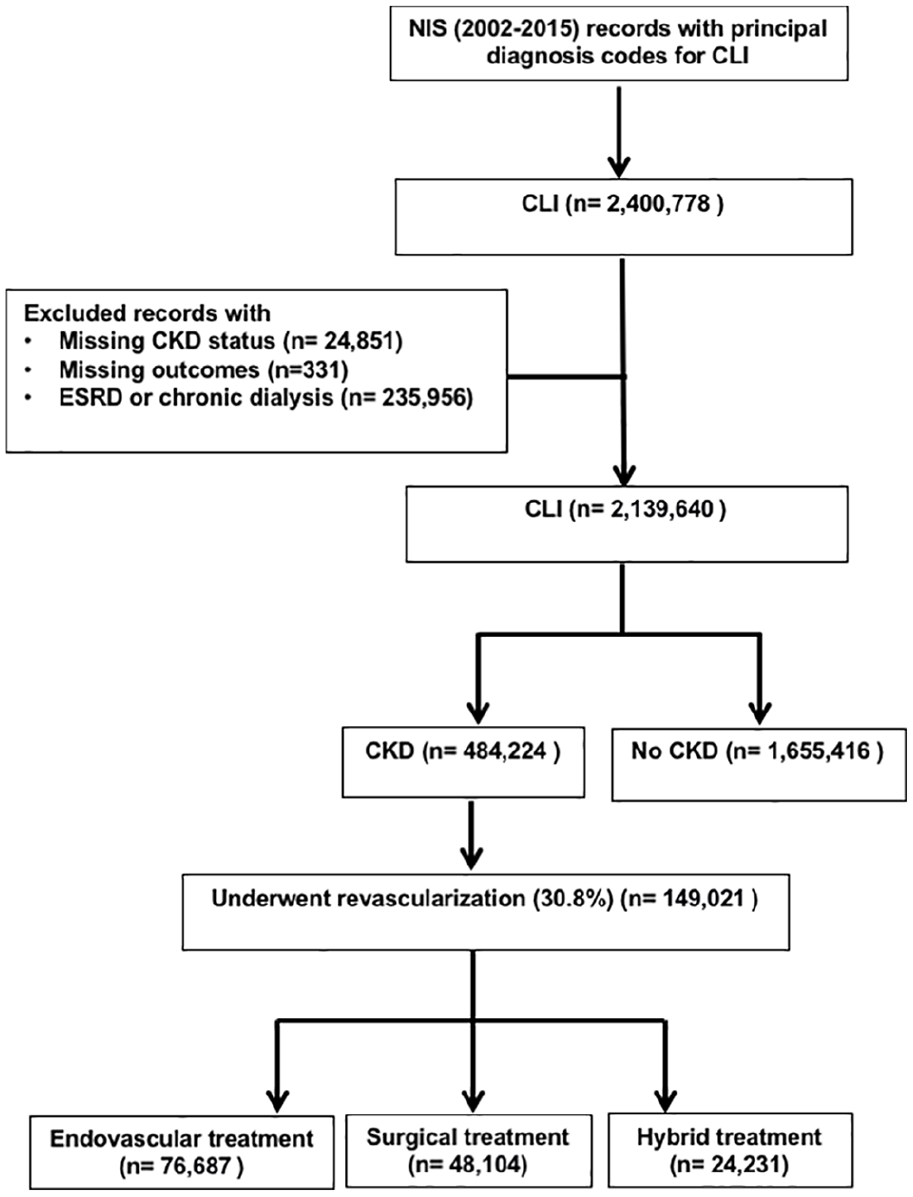
Study flow diagram.
The baseline characteristics for patients with CLI and CKD versus without are outlined in Table 1. Patients with CLI and CKD were slightly younger and less likely to be women compared with patients with no CKD. Patients with CLI and CKD were more likely to be black or Hispanic. Compared with no CKD, patients with CLI and CKD had a higher burden of comorbidities, including: coagulopathy, obesity, hypertension, hypothyroidism, diabetes, chronic liver disease, chronic anemia, heart failure, valvular heart disease, prior pacemaker, coronary artery disease, prior MI, prior PCI, prior CABG, prior stroke, and pulmonary circulation disorders.
Baseline characteristics for CLI patients with CKD and without CKD.
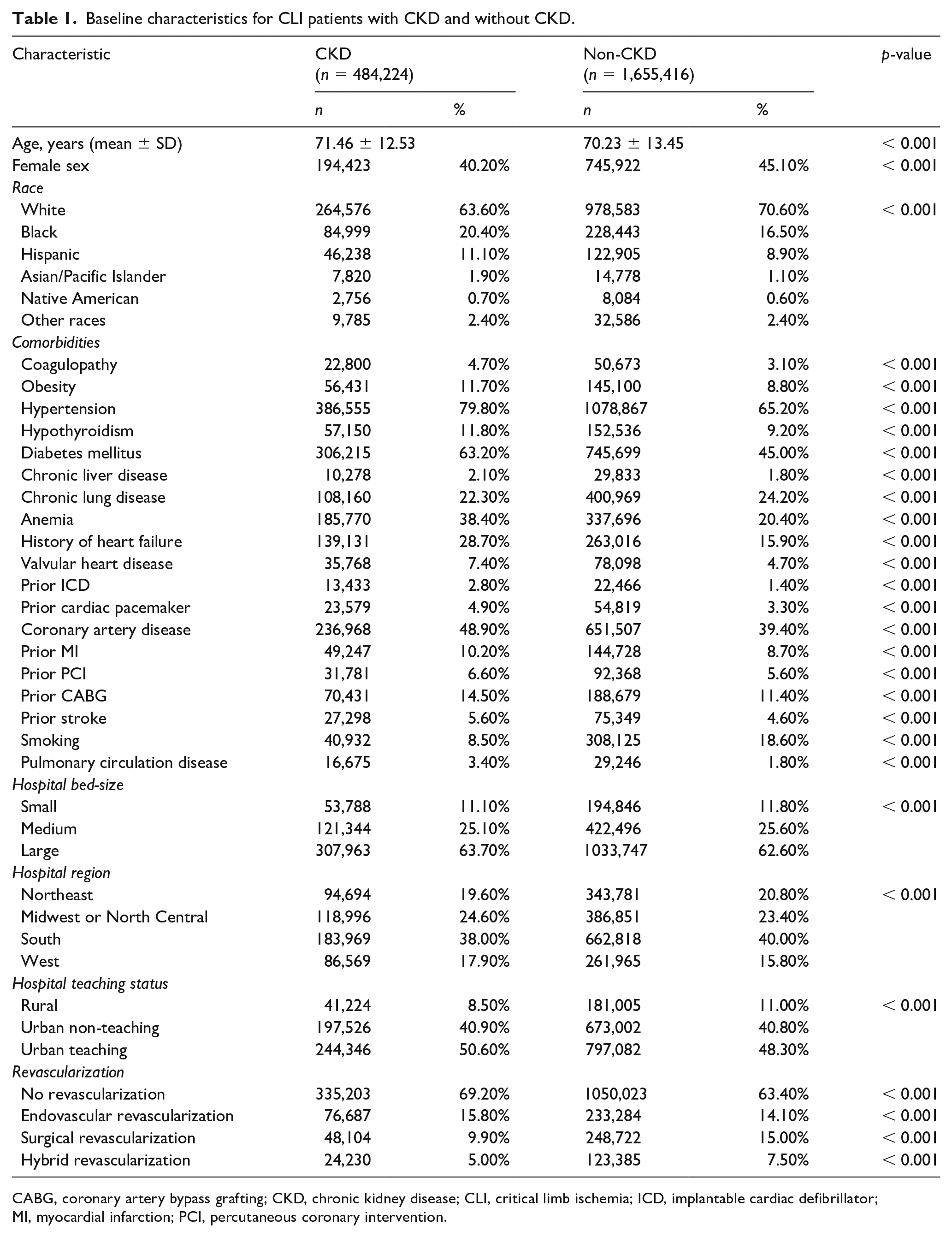
CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CLI, critical limb ischemia; ICD, implantable cardiac defibrillator; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Trends in hospitalizations for CLI among patients with CKD versus without CKD
The number of hospitalized patients with PAD and CKD increased from 151,140 hospitalizations in 2002 to 590,147 hospitalizations in 2015 (Ptrend < 0.001). During the study period, there was a temporal increase in the number of hospitalizations for CLI in those with CKD (33,081 in 2002 vs 44,313 hospitalizations in 2015, Ptrend = 0.01), while there was a decrease in the number of hospitalizations for CLI in those without CKD (132,858 in 2002 vs 116,206 hospitalizations in 2015, Ptrend = 0.01) (Figure 2). There was a rising trend for any revascularization modality among those with CLI and CKD (25.3% in 2002 vs 31.7% in 2015, Ptrend < 0.001) and CLI without CKD (30.2% in 2002 vs 39.8% in 2015, Ptrend < 0.001). There was also a reduction in the rates of in-hospital mortality among those with CKD (9.2% in 2002 vs 2.8% in 2015, Ptrend < 0.001), as well as among those without CKD (3.7% in 2002 vs 2.0% in 2015, Ptrend < 0.001) (Figure 2).
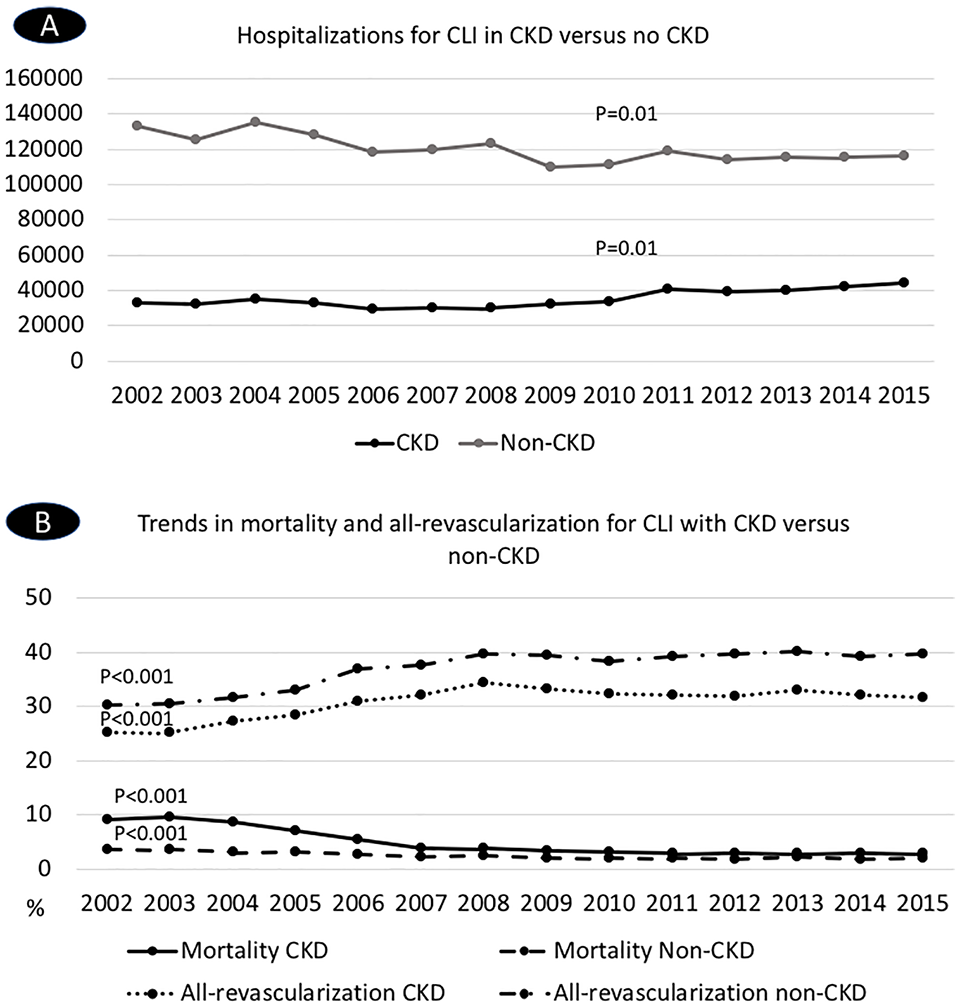
Temporal trends in (A) hospitalizations and (B) mortality and all-revascularization for CLI in patients with CKD versus without CKD.
From 2002 to 2015, there was an increase in endovascular and hybrid revascularization modalities corresponding to a decrease in surgical revascularization for CLI in those with CKD and without CKD. Among those patients with CKD, the use of endovascular revascularization increased from 6.0% in 2002 to 19.3% in 2015 (Ptrend < 0.001), surgical revascularization decreased from 16.9% in 2002 to 6.3% in 2015 (Ptrend < 0.001), while hybrid revascularization increased from 2.3% in 2002 to 6.1% in 2015 (Ptrend = 0.01). Among those without CKD, the use of endovascular revascularization also increased from 5.0% in 2002 to 17.8% in 2015 (Ptrend < 0.001), surgical revascularization decreased from 22.9% in 2002 to 10.6% in 2015 (Ptrend < 0.001), and hybrid treatment increased from 2.4% in 2002 to 11.3% in 2015 (Ptrend < 0.001) (Figure 3).
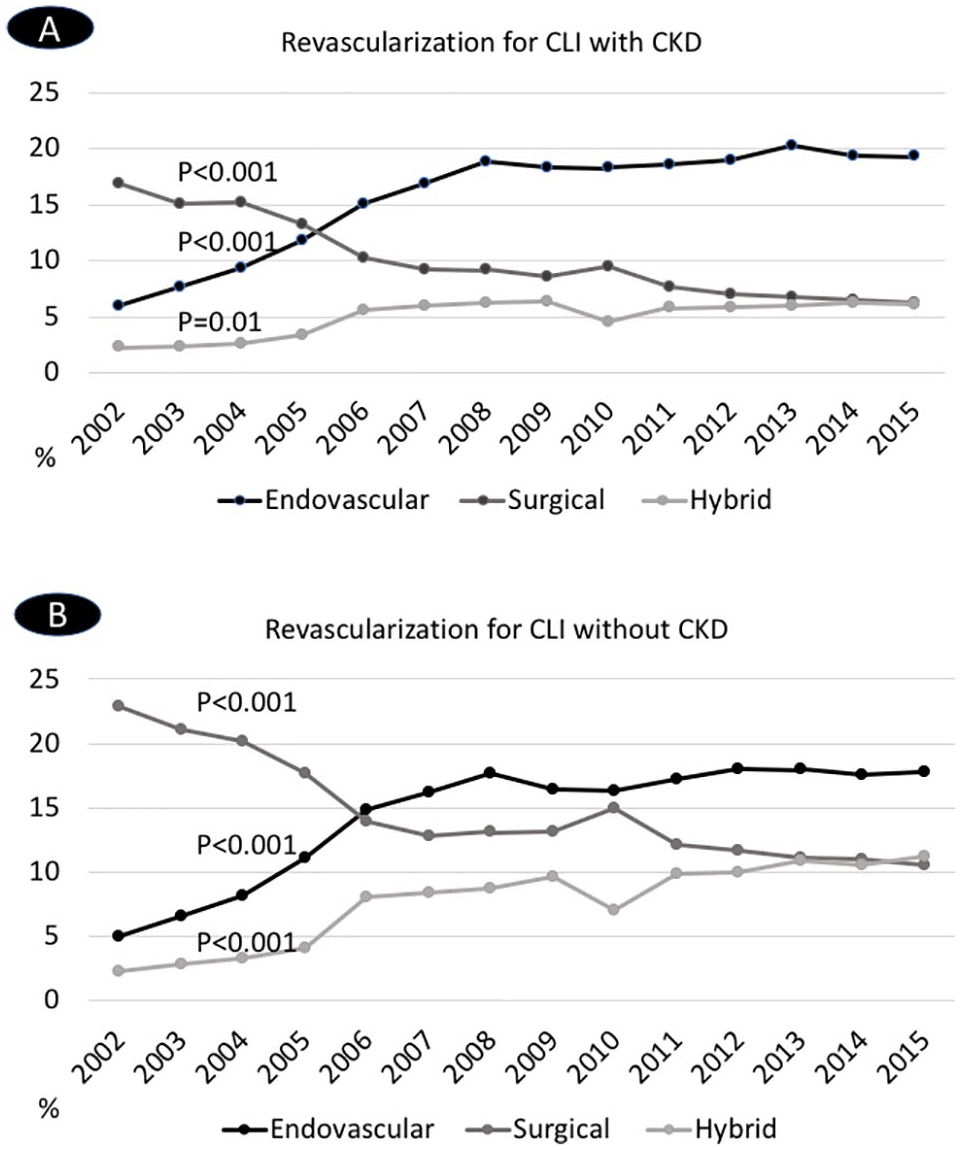
Temporal trends in revascularization modalities for CLI in patients (A) with CKD and (B) without CKD.
Outcomes of CLI for CKD versus no CKD
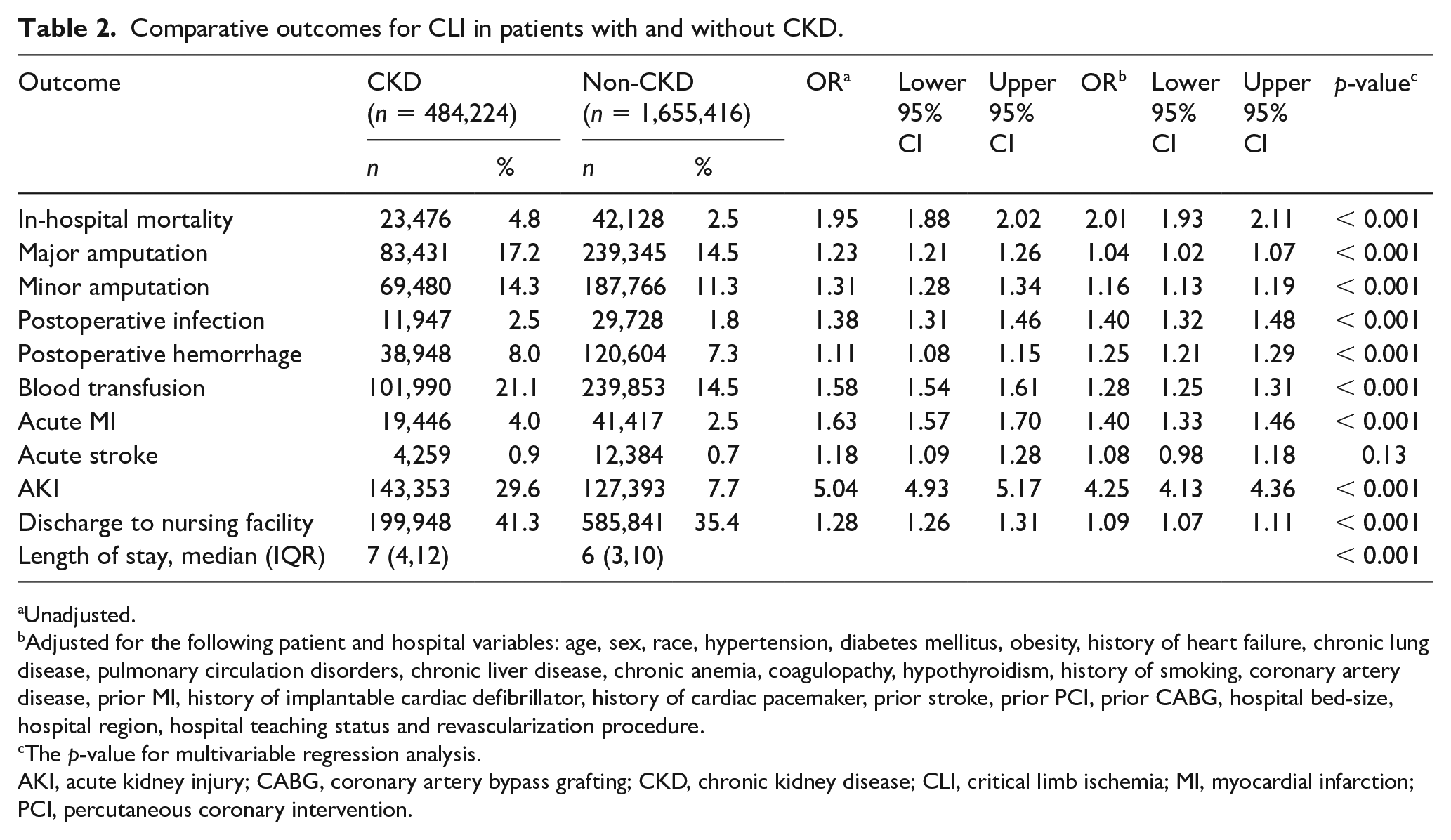
On multivariable analysis, CLI in patients with CKD was associated with higher rates of in-hospital mortality (4.8% vs 2.5%, adjusted odds ratio (OR) 2.01; 95% CI 1.93–2.11, p < 0.001). Compared with no CKD, CLI with CKD was associated with higher rates of major amputation (adjusted-OR 1.04; 95% CI 1.02–1.07, p < 0.001), minor amputations, postoperative infection, postoperative hemorrhage, blood transfusion, acute MI, acute stroke, AKI, discharges to nursing facility, and longer median length of hospital stay (Table 2). Among those with CKD, multivariable analysis showed higher rates of in-hospital mortality with worsening stages of CKD. Using CKD stage 1 as a reference, the rate of in-hospital mortality was higher in those with stage 2 CKD (2.2% vs 1.1%, adjusted-OR 1.77; 95% CI 1.36–2.30), stage 3 CKD (2.5% vs 1.1%, adjusted-OR 2.73; 95% CI 2.12–3.51), stage 4 CKD (4.2% vs 1.1%, adjusted-OR 2.81; 95% CI 1.98–3.98), and stage 5 CKD (5.6% vs 1.1%, adjusted-OR 4.88; 95% CI 1.89–12.62).
Comparative outcomes for CLI in patients with and without CKD.
Unadjusted.
Adjusted for the following patient and hospital variables: age, sex, race, hypertension, diabetes mellitus, obesity, history of heart failure, chronic lung disease, pulmonary circulation disorders, chronic liver disease, chronic anemia, coagulopathy, hypothyroidism, history of smoking, coronary artery disease, prior MI, history of implantable cardiac defibrillator, history of cardiac pacemaker, prior stroke, prior PCI, prior CABG, hospital bed-size, hospital region, hospital teaching status and revascularization procedure.
The p-value for multivariable regression analysis.
AKI, acute kidney injury; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CLI, critical limb ischemia; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Revascularization for patients with CLI and CKD
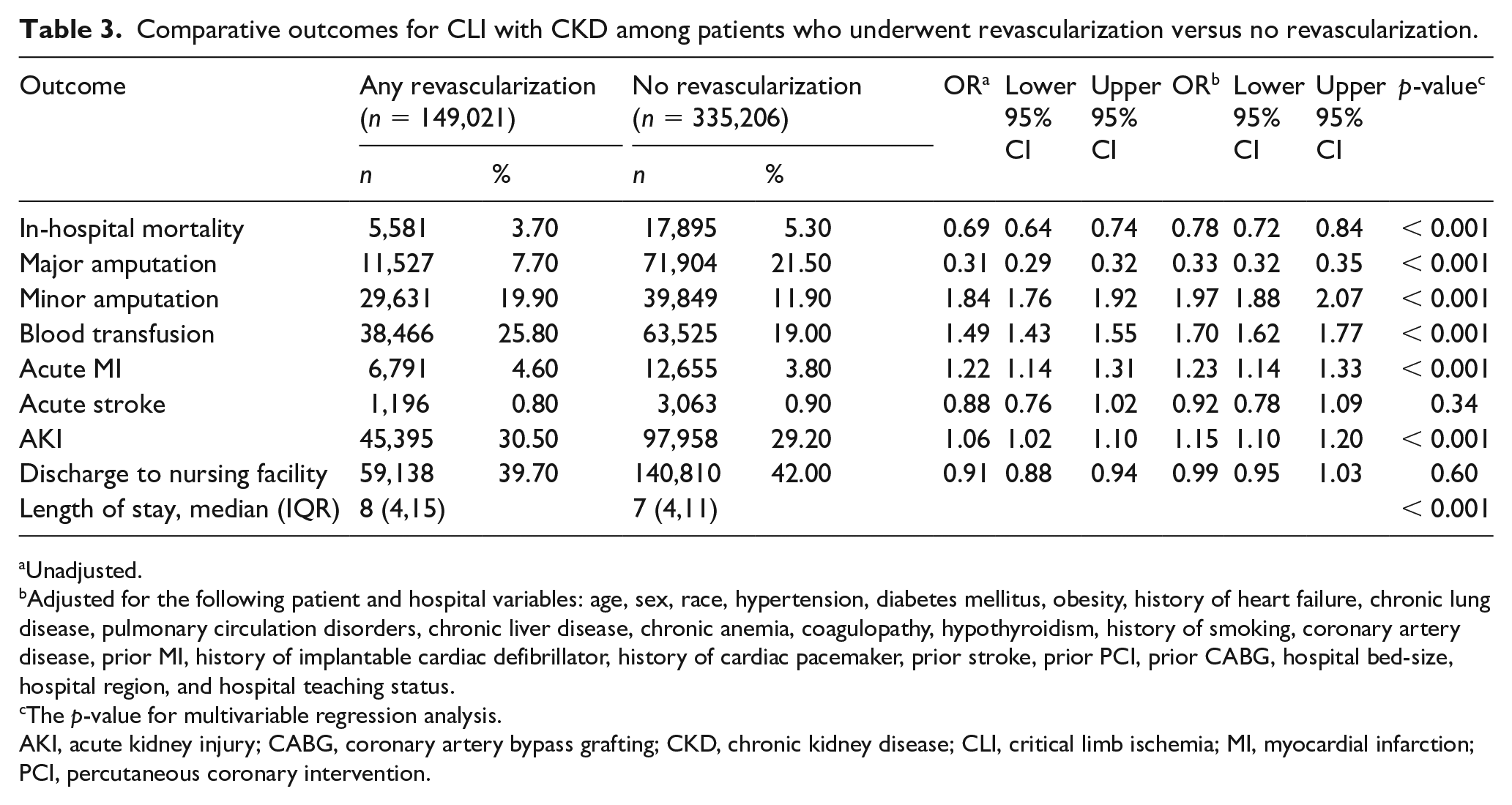
Compared with no revascularization, revascularization was associated with lower rates of in-hospital mortality (3.7% vs 5.3%, adjusted-OR 0.78; 95% CI 0.72–0.84, p < 0.001) and lower major amputation (adjusted-OR 0.33; 95% CI 0.32–0.35, p < 0.001) among patients with CLI and CKD. Revascularization was associated with slightly higher rates of AKI, acute MI, and longer length of hospital stay compared with those who did not undergo revascularization (Table 3).
Comparative outcomes for CLI with CKD among patients who underwent revascularization versus no revascularization.
Unadjusted.
Adjusted for the following patient and hospital variables: age, sex, race, hypertension, diabetes mellitus, obesity, history of heart failure, chronic lung disease, pulmonary circulation disorders, chronic liver disease, chronic anemia, coagulopathy, hypothyroidism, history of smoking, coronary artery disease, prior MI, history of implantable cardiac defibrillator, history of cardiac pacemaker, prior stroke, prior PCI, prior CABG, hospital bed-size, hospital region, and hospital teaching status.
The p-value for multivariable regression analysis.
AKI, acute kidney injury; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CLI, critical limb ischemia; MI, myocardial infarction; PCI, percutaneous coronary intervention.
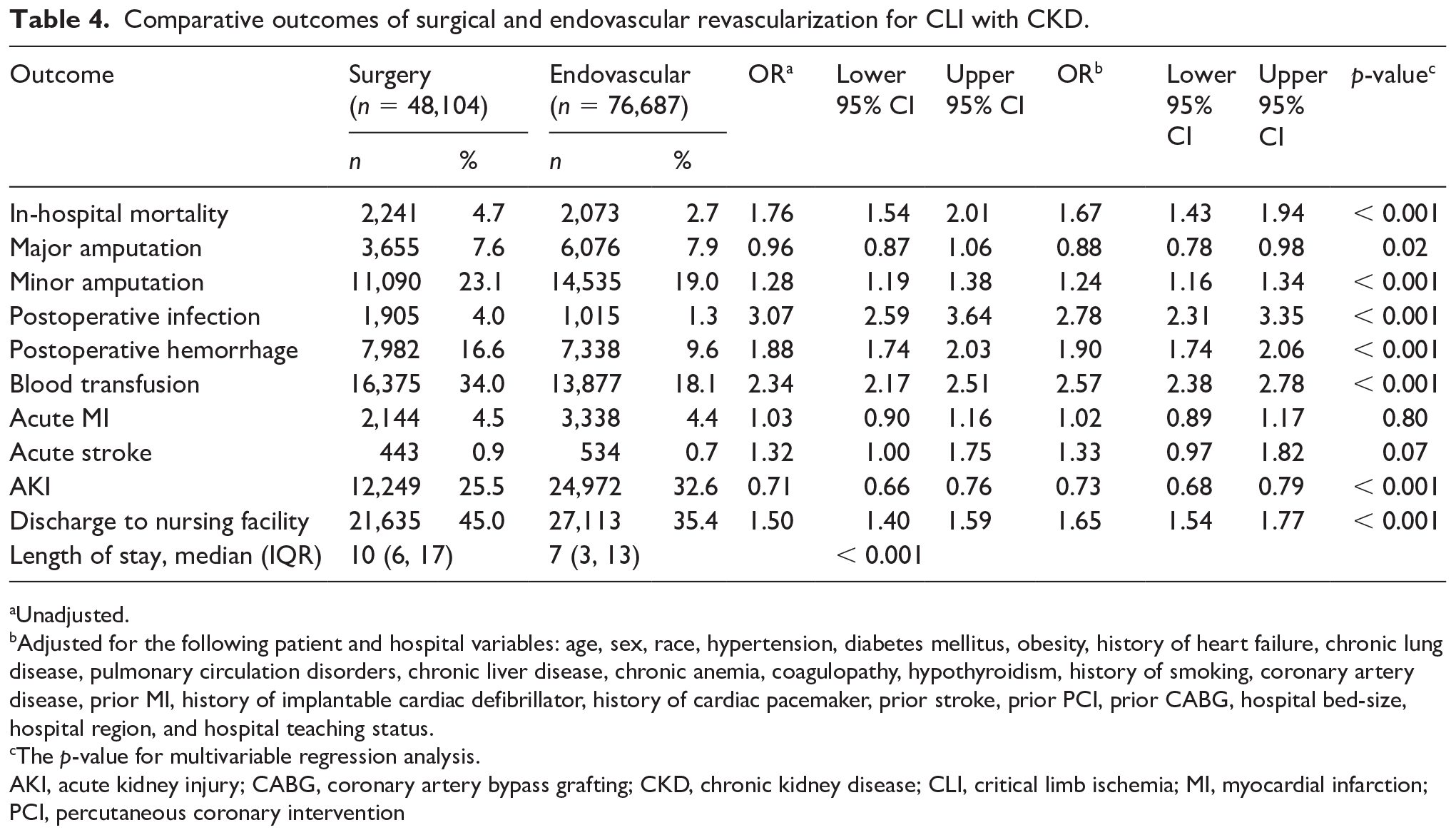
Compared with endovascular revascularization, surgical revascularization was associated with higher rates of in-hospital mortality (4.7% vs 2.7%, adjusted-OR 1.67; 95% CI 1.43–1.94, p < 0.001), minor amputations, postoperative infection, postoperative hemorrhage, blood transfusion, discharge to nursing facility, and longer length of hospital stay. Additionally, surgical revascularization was associated with lower rates of major amputation (adjusted-OR 0.88; 95% CI 0.78–0.98, p = 0.02) and AKI. There was no difference between surgical and endovascular revascularization in the rates of acute MI or acute stroke (Table 4).
Comparative outcomes of surgical and endovascular revascularization for CLI with CKD.
Unadjusted.
Adjusted for the following patient and hospital variables: age, sex, race, hypertension, diabetes mellitus, obesity, history of heart failure, chronic lung disease, pulmonary circulation disorders, chronic liver disease, chronic anemia, coagulopathy, hypothyroidism, history of smoking, coronary artery disease, prior MI, history of implantable cardiac defibrillator, history of cardiac pacemaker, prior stroke, prior PCI, prior CABG, hospital bed-size, hospital region, and hospital teaching status.
The p-value for multivariable regression analysis.
AKI, acute kidney injury; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CLI, critical limb ischemia; MI, myocardial infarction; PCI, percutaneous coronary intervention
Discussion
In this observational analysis including > 2.1 million hospitalizations with CLI, we sought to evaluate the trends and outcomes of CLI in patients with CKD. The principal findings of this analysis were: (1) there was an increase in hospitalizations for CLI in patients with CKD from 2002 to 2015; (2) patients with CLI and CKD were less likely to receive any revascularization compared with those without CKD; (3) CLI among those with CKD was associated with higher in-hospital mortality compared with those without CKD; (4) patients with CLI and CKD who underwent any revascularization procedure had lower in-hospital mortality compared with those who were not revascularized; and (5) compared with endovascular revascularization, surgical revascularization for CLI was associated with higher in-hospital mortality, but lower rates of AKI among those with CKD.
Trends in hospitalizations and outcomes for CLI and CKD
In this analysis, there was a rising trend in hospitalizations for CLI among those with CKD, in contrast to those without CKD. This rise is an important finding despite advances in recognition of important secondary prevention measures, including the administration of antiplatelet and statin therapies. We also observed that patients with CLI and CKD had a significantly higher burden of comorbidities compared to those without CKD, consistent with previous reports correlating greater prevalence of risk factors among patients with CLI and CKD. 6 Patients with CKD were more commonly treated with endovascular revascularization compared to those without CKD, which might reflect the burden of comorbidities, lack of autogenous vein conduit, or poor distal targets for bypass associated with PAD patterns in CKD. 15 Importantly, patients with CKD and CLI were less likely to undergo any revascularization compared to those with CLI but no CKD. This finding is concerning given the observed reduction in mortality and major amputation among those with CLI and CKD who underwent revascularization. The lower likelihood for revascularization among patients with CKD suggest that physicians are reluctant to offer revascularization therapies to patients with CKD despite mounting evidence that revascularization improves outcomes among patients with CLI.3,16,17 This could be related to perceived higher risk with revascularization, due to higher prevalence of comorbid conditions as well as reduced kidney function and concern for contrast-related renal complications.
This analysis identified a significant improvement in outcomes related to CLI admissions over the course of the study period, as evidenced by longitudinal reductions in in-hospital mortality rates in both CKD and non-CKD groups. This finding corresponds to a concomitant increase in rates of revascularization for patients hospitalized with CLI. As was identified in this study population, other published data have demonstrated a rise in the utilization of endovascular revascularization and a reduction in the utilization of surgical revascularization for the treatment of patients with CLI.16,18,19 Our results signal a possible correlation between the temporal improvement in outcomes of hospitalizations with CLI and the wider adoption of any revascularization modality. At the same time, however, advances in guideline-directed medical therapy, public awareness regarding recognition and treatment of PAD, access to timely wound care, and secondary prevention measures may also significantly contribute to improved outcomes in CLI.3,20,21
Outcomes of CLI among CKD versus no CKD
This analysis showed worse in-hospital outcomes for CLI and CKD versus no CKD, including higher mortality and major amputation rates. These results are consistent with previous studies showing that CKD is associated with higher mortality among all-comers with PAD.6,22,23 In one study by Lüders et al., the authors evaluated 41,888 patients hospitalized for PAD-related complications. 6 They reported that the co-existence of CKD was associated with significantly higher in-hospital as well as long-term mortality among patients with PAD. 6 Lüders et al. also reported an approximately twofold higher risk of amputation among patients with CKD. 6 Similarly, Pasqualini et al. reported a 2.2-fold increase in long-term mortality with CKD among patients with PAD. 22 Liew et al. also reported higher 6-year mortality with CKD among patients with PAD. 23 Our analysis showed that CLI among patients with CKD was associated with higher in-hospital complications, including postoperative infection, bleeding, blood transfusion, acute MI, acute stroke, AKI, and longer length of hospital stay. Adverse outcomes were also described in studies evaluating the impact of CKD on all-comers with PAD.6,24
The association between CKD and worse outcomes with CLI in our study is likely multifactorial. Patients with CKD tend to have more extensive and severe arterial disease compared to patients without CKD. 6 Additionally, those with CKD have a higher burden of comorbidities, as was demonstrated in our study, compared to those without CKD. In addition, the presence of renal insufficiency might influence the consideration of more extensive endovascular or surgical revascularization procedures, in light of concerns that such procedures might worsen kidney function. These factors collectively might contribute to the higher rates of in-hospital adverse events and mortality observed in patients with CKD admitted with CLI.
Revascularization approaches for patients with CLI and CKD
Studies have consistently demonstrated the benefit of revascularization for all-comers with CLI in improving survival and limb salvage.3,16,17 That notwithstanding, individuals with CKD are perceived to have a higher risk for endovascular or surgical revascularization procedures. Our study identifies a correlation between revascularization for CLI in patients with CKD and improved survival and limb salvage, consistent with previous studies of all-comers with CLI. Our analysis is the first to-date to compare the outcomes of endovascular versus surgical revascularization in a large population of patients with CKD. We found that surgical revascularization was associated with significantly higher in-hospital mortality compared with endovascular revascularization. These results are in discordance with studies evaluating all-comers with CLI, where evidence suggests comparable outcomes for endovascular versus surgical revascularization.25,26 Such discordance might be attributable to the higher surgical risk among patients with CKD, who are more prone to peri-procedural complications compared to those in the general population. 27 Given the observational nature of this analysis, however, there is a possibility that selection bias may influence the observed differences in outcomes between those treated with surgical versus endovascular revascularization. In the absence of randomized data, our study results are hypothesis-generating regarding the outcomes of revascularization modalities for CLI among patients with CKD. The BEST CLI (Best Endovascular versus Best Surgical Therapy in patients with CLI) is an ongoing large multicenter, open label randomized trial comparing the outcomes of endovascular and surgical revascularization approaches for patients with CLI eligible to both modalities. 28 The BEST-CLI trial is expected to add greater insight into the optimal revascularization strategies for patients with CLI; however; the trial is not powered to evaluate the outcomes of revascularization among the subgroup of patients enrolled with CKD. Given the unique nature and outcomes of CLI in patients with CKD, further prospective studies are warranted to evaluate the optimal revascularization approach for patients in this important population.
Limitations
The strength of the current analysis stems from its large sample size and national representation. There are certain limitations to this type of analysis, however. Since it is an administrative database, the NIS is susceptible to documentation and coding errors. Nevertheless, the NIS has been extensively validated internally and externally.29,30 The NIS only provides data on in-hospital outcomes with no long-term outcomes data. Patients with ESRD on hemodialysis who present with CLI represent a distinct high-risk group of patients, who have been demonstrated to carry a significantly higher propensity for tissue loss, amputations, and mortality.31,32 On the other hand, there is a paucity of data on the outcomes of non-dialysis patients with CKD who present with CLI; hence, in our analysis, we excluded patients with ESRD on chronic dialysis. Many useful data were irretrievable for our analysis, including details on revascularization procedures such as timing of the procedure, laterality, and technical details regarding bypass grafts and endovascular devices used. Also, data on imaging, laboratory results, and medications were not available for assessment. Importantly, there were no data on the extent of PAD, and the reasons for undergoing a certain revascularization strategy. Revascularization procedures for pre-CLI PAD in patients with CKD are mostly in outpatient settings and would not be captured by the NIS. Despite our extensive multivariable analysis, there remains the potential for influence by unmeasured or inadequately corrected confounding variables. There is a potential for survivor bias in this analysis, since patients who received medical therapy only might have been too sick to receive any procedure (amputation or revascularization). Finally, this analysis was limited until September 2015 using the ICD-9 coding system, and it is possible that the results might have varied in the ensuing years. Overall, however, the study addresses an important knowledge gap regarding outcomes of CLI in patients with CKD.
Conclusion
This observational analysis from a large national database identified a significant longitudinal increase in hospitalizations for CLI among patients with CKD between 2002 and 2015. Patients with CLI and CKD were less likely to receive any revascularization procedure compared with those without CKD. Patients with CLI and CKD who underwent revascularization were associated with lower mortality and major amputation compared with those who did not undergo revascularization. Compared with endovascular therapy for CLI and CKD, surgical revascularization was associated with higher in-hospital mortality. Given the observational nature of this analysis, our findings are mainly hypothesis-generating and need to be confirmed in future prospective studies. The observed disparity in revascularization for those with CLI and CKD compared with those without CKD requires immediate attention.
Supplemental Material
Supp_table_1_IE – Supplemental material for Temporal trends and outcomes of critical limb ischemia among patients with chronic kidney disease
Supplemental material, Supp_table_1_IE for Temporal trends and outcomes of critical limb ischemia among patients with chronic kidney disease by Ayman Elbadawi, Islam Y Elgendy, Michael Megaly, Mohammed Elzeneini, Amgad Mentias, Mohamed Omer, Gbolahan Ogunbayo, Devesh Rai, Douglas E Drachman and Mehdi H Shishehbor in Vascular Medicine
Footnotes
Declaration of conflicting interests
Mehdi H Shishehbor serves as an advisory board member and consultant for Abbott Vascular, Medtronics, Boston Scientific, Philips, and Terumo and as a National or Site Principal Investigator for LimFlow, Terumo R2P, and Abbott LIFE-BTK. Douglas E Drachman serves as a consultant to Abbott Vascular, Boston Scientific, Broadview Ventures, and Cardiovascular Systems Inc. All other authors have no conflict of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.