
Abstract

Endovascular therapy has been increasingly utilized for the treatment of lower extremity peripheral artery disease (PAD) given its shorter recovery time, overall safety, and non-inferiority compared to surgical repair. 1 After endovascular interventions, antiplatelet therapy (anti-PLT) is frequently prescribed. The proximate goal of anti-PLT is to reduce the risk of acute limb ischemia caused by thrombosis and to potentially reduce the risk of major adverse cardiovascular events (MACE) due to atherosclerosis progression. 2 Anti-PLT monotherapy has been shown to reduce MACE rates in patients with symptomatic PAD, although the absolute event rate reduction with monotherapy may be small. 3 Thus, according to the TASC (TransAtlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease) recommendations, single anti-PLT should be started before any endovascular procedure and should be continued lifelong. 4 However, data regarding the additive benefit of dual antiplatelet therapy (DAPT) and the optimal duration of anti-PLT are sparse, with only a few studies guiding decision-making.3,5 The American College of Cardiology and the American Heart Association (ACC/AHA) recommend at least 1 month of combined therapy with aspirin and clopidogrel after infrainguinal endovascular procedures; however, the level of evidence for this recommendation is low (grade 2B). 5 Moreover, in several trials investigating peripheral intervention devices, treatment with DAPT (i.e. aspirin and clopidogrel) was mandated for a time period ranging from 1 to 3 months, but this recommendation was again based primarily on expert consensus. 6 Detailed anti-PLT guidelines for PAD are presented in Table 1.
Current guidelines for antiplatelet therapy in PAD.
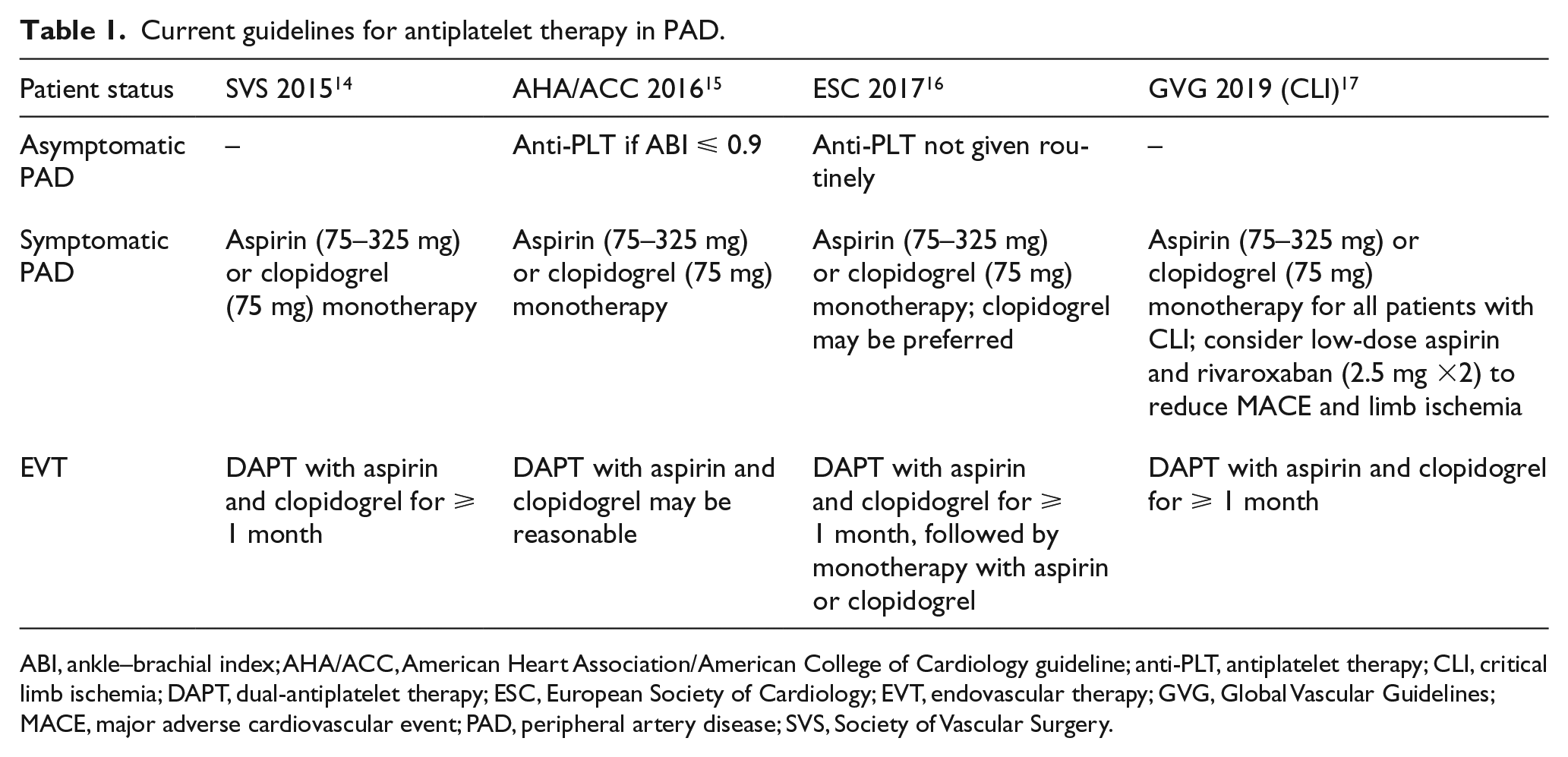
ABI, ankle–brachial index; AHA/ACC, American Heart Association/American College of Cardiology guideline; anti-PLT, antiplatelet therapy; CLI, critical limb ischemia; DAPT, dual-antiplatelet therapy; ESC, European Society of Cardiology; EVT, endovascular therapy; GVG, Global Vascular Guidelines; MACE, major adverse cardiovascular event; PAD, peripheral artery disease; SVS, Society of Vascular Surgery.
In the current study by Kim and colleagues, 7 the authors conducted a retrospective analysis to describe the practice patterns of DAPT prescription following endovascular procedures for the treatment of lower extremity lesions and to determine which factors might predict discontinuation of anti-PLT therapy in real-world practice. In total, the current study included 23,420 patients and approximately 58% of the patients were discharged with DAPT. 7 The study demonstrated that patients prescribed DAPT after endovascular intervention had higher odds of coronary artery disease (CAD), history of percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG), and history of previous lower extremity vascular intervention. Subjects prescribed DAPT were also more likely to be prescribed statins, indicating overlap in optimal medical therapy. Thus, this study suggested that patients with cardiovascular risk factors and/or comorbidities were more likely to be prescribed DAPT at the time of hospital discharge after endovascular intervention. Interestingly, at 3, 12, and 24 months of follow-up, 70.47%, 56.49%, and 49.63% of these patients remained on DAPT, respectively.
The high variation in actual DAPT duration demonstrated by this study may be driven by the lack of class I evidence supporting DAPT use, differences in revascularization strategies, and several patient comorbidities (i.e. cardiovascular factors). 8 Consistent with this, prior studies have suggested that the presence of recognized CAD and/or diabetes drives most decision making among medical therapy of patients with PAD, rather than the recognition that PAD is associated with a high risk of MACE. 9 Some studies regarding DAPT use among patients with symptomatic PAD (i.e. claudication, CLI) have shown reduced rates of MACE and mortality compared to aspirin monotherapy. 10 The mechanism of this late benefit of DAPT is likely that it protects the patients from both limb adverse events and overall cardiovascular mortality. 3 However, the benefits of DAPT must be balanced by the potential higher risk for bleeding complications, and, as such, in several individualized cases DAPT should be prescribed with caution (Table 2). Additionally, the clinical decision making for anti-PLT and antithrombotic therapy after endovascular intervention is becoming more complicated with the addition of direct-acting oral anticoagulants, such as rivaroxaban. The recent Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS; ClinicalTrials.gov Identifier: NCT01776424) trial, comparing combined therapy with rivaroxaban and aspirin to monotherapy with either aspirin or rivaroxaban, demonstrated the lower risk of MACE in the combined group.11,12 However, the safety and efficacy of this antithrombotic approach in patients with symptomatic PAD requiring revascularization remains unclear. The Vascular Outcomes study of Aspirin along with rivaroxaban in endovascular or surgical limb revascularization for peripheral artery disease (VOYAGER PAD; ClinicalTrials.gov Identifier: NCT02504216) trial will evaluate the outcomes of rivaroxaban added to anti-PLT in patients undergoing revascularization for peripheral arterial lesions. 13
Factors associated with longer or shorter DAPT in clinical practice.
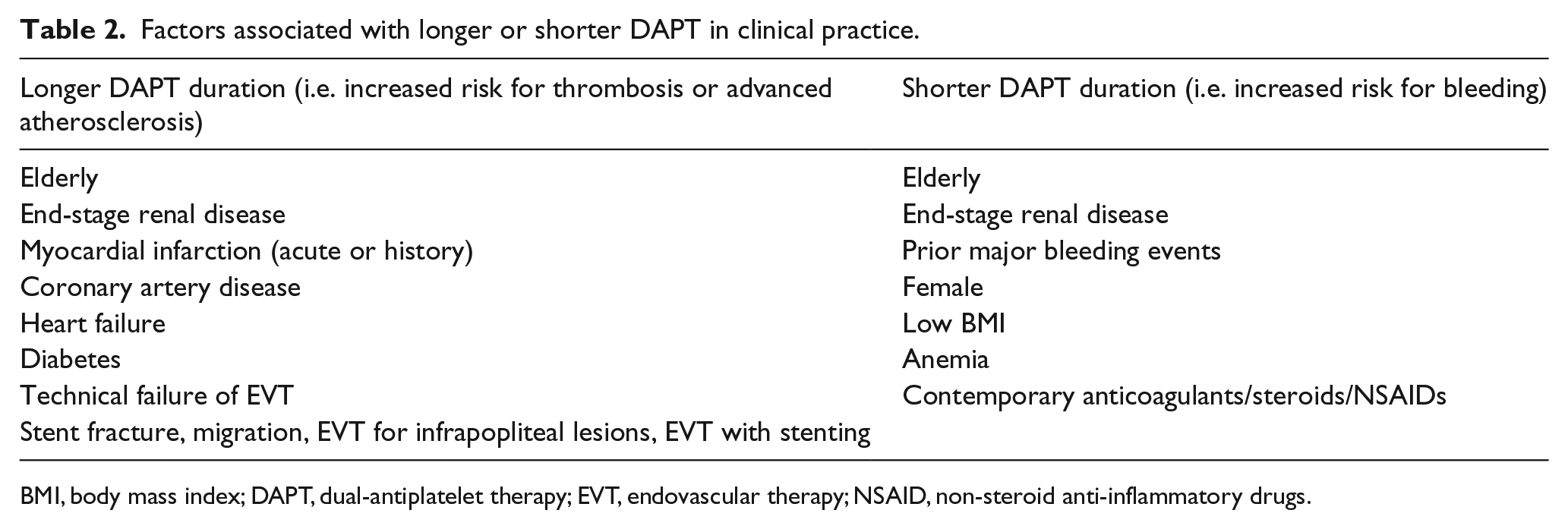
BMI, body mass index; DAPT, dual antiplatelet therapy; EVT, endovascular therapy; NSAID, non-steroid anti-inflammatory drugs.
In the current study by Kim et al, the practice patterns of DAPT prescription following endovascular procedures were highly variable, reflecting the lack of data regarding optimal DAPT treatment. 7 Understanding the role of lesion location, device type, and degree of PAD severity on clinical outcomes of DAPT/antithrombotic therapy after endovascular interventions for lower extremity lesions is needed in order to identify the optimal DAPT/antithrombotic regimen. Thus, further prospective real-world studies are necessary to determine the efficacy of DAPT/antithrombotic therapy after different revascularization techniques in specific high-risk populations (e.g. elderly patients, patients with cardiovascular comorbidities, etc.). Finally, considering the promising results of either DAPT (i.e. aspirin and clopidogrel) or combined antithrombotic therapy (i.e. aspirin and rivaroxaban), we could be carefully optimistic that wide application of continuous DAPT/antithrombotic therapy has the potential to improve the efficacy and long-term durability of endovascular interventions while also minimizing cardiovascular mortality.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Armstrong is a consultant to Abbott Vascular, Boston Scientific, Cardiovascular Systems Incorporated (CSI), Intact Vascular, Medtronic, Philips, and PQ Bypass. Dr Giannopoulos has no relationships to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.