
Abstract
The left ventricular outflow tract (LVOT) velocity time integral (VTI) is an easily measured echocardiographic stroke volume index analog. Low values predict adverse outcomes in left ventricular failure. We postulate the left ventricular VTI may be a signal of right ventricular dysfunction in acute pulmonary embolism, and therefore a predictor of poor outcomes. We retrospectively reviewed echocardiograms on all Pulmonary Embolism Response Team activations at our institution at the time of pulmonary embolism diagnosis. Low LVOT VTI was defined as ⩽ 15 cm. We examined two composite outcomes: (1) in-hospital death or cardiac arrest; and (2) shock or need for primary reperfusion therapies. Sixty-one of 188 patients (32%) had a LVOT VTI of ⩽ 15 cm. Low VTI was associated with in-hospital death or cardiac arrest (odds ratio (OR) 6, 95% CI 2, 17.9; p = 0.0014) and shock or need for reperfusion (OR 23.3, 95% CI 6.6, 82.1; p < 0.0001). In a multivariable model, LVOT VTI ⩽ 15 remained significant for death or cardiac arrest (OR 3.48, 95% CI 1.02, 11.9; p = 0.047) and for shock or need for reperfusion (OR 8.12, 95% CI 1.62, 40.66; p = 0.011). Among intermediate–high-risk patients, low VTI was the only variable associated with the composite outcome of death, cardiac arrest, shock, or need for reperfusion (OR 14, 95% CI 1.7, 118.4; p = 0.015). LVOT VTI is associated with adverse short-term outcomes in acute pulmonary embolism. The VTI may help risk stratify patients with intermediate–high-risk pulmonary embolism.
Introduction
Outcomes in acute pulmonary embolism (PE) vary widely, with early mortality ranging from < 1% among low-risk patients to over 50% among high-risk subsets.1–4 A number of tools are available to identify low-risk PE, but accurate identification and further risk stratification of patients with intermediate–high-risk PE, patients with both imaging and biochemical evidence of right ventricular (RV) dysfunction, remains difficult. 5 Studies have demonstrated association between RV dysfunction and mortality among initially hemodynamically stable patients with acute PE.4,6–12 However, the positive predictive value is low, and specific echocardiographic indicators of RV dysfunction differ between studies producing conflicting results.1,12 The risk of hemodynamic deterioration or death among patients with intermediate–high-risk PE may not be apparent; current imaging strategies and clinical models do not fully capture this risk. 5 How best to identify such patients remains a key question in PE research.
The left ventricular outflow tract (LVOT) velocity time integral (VTI), the sum of instantaneous velocities measured at the LVOT by pulse wave (PW) Doppler, is a stroke volume index analog.13–16 The LVOT VTI provides a reliable estimate of cardiac function and is commonly followed in the management of shock.17–19 This measure correlates well with indices of perfusion, and outperforms ejection fraction in predicting outcomes in patients with heart failure.14,15,20 The Doppler tracing is part of the standard echocardiographic protocol, and is feasible across multiple levels of training in the emergency setting with good intra-, and inter-observer repeatability.21–23
As acute cor pulmonale leads to left ventricular filling impairment and therefore stroke volume reduction, low VTI may identify patients with PE at risk for impending clinical deterioration, and therefore those who may benefit most from intensive monitoring or primary reperfusion. 24 To our knowledge, no published studies have evaluated VTI in risk stratification or outcome assessment of acute PE. We carried out a retrospective, single-center study of all Pulmonary Embolism Response Team (PERT) activations between October 1, 2016 and October 1, 2018 to determine the association between LVOT VTI and in-hospital mortality or cardiac arrest, and shock or need for primary reperfusion therapies.
Materials and methods
This was a single-center, retrospective study approved by the NYU Langone Health Institutional Review Board (ID s18-01125). The PERT is a multidisciplinary group engaged at the discretion of the consulting team following the diagnosis of acute PE. We reviewed clinical and echocardiographic data of PERT activations at our institution between October 1, 2016 and October 1, 2018.
Clinical definitions
Electronic medical records (Epic©; Epic Systems Corporation, Verona, WI, USA) were reviewed for clinical and outcomes data. The highest heart rate, and lowest systolic and diastolic blood pressures prior to the diagnosis of PE were reported. RV strain by computerized tomography (CT) or transthoracic echocardiogram (TTE) was defined as radiologist or echocardiographer reported evidence of RV dilation or dysfunction. Brain natriuretic peptide (BNP) > 100 pg/mL, N-terminal pro-brain natriuretic peptide (NT-proBNP) > 300 pg/mL, and troponin I (TnI) > 0.04 ng/mL were classified as elevated. Simplified Pulmonary Embolism Severity Index (sPESI) and Bova scores were calculated as previously described.25,26
Echocardiographic measures
VTI was obtained by PW Doppler at the LVOT in either the apical three-chamber, or in the anteriorly angulated apical four-chamber view (‘apical five-chamber view’) (Figure 1A–C). We excluded studies that did not have LVOT VTI tracings, had LVOT VTI of insufficient quality to trace, and patients with left ventricular outflow tract obstruction (LVOTO) (Figure 1D). Spectral Doppler envelopes were traced retrospectively by a board-certified echocardiographer in syngo® Dynamics Workplace software (version VA20E_20.0.0.2645_HF02 Build 2645) at end-expiration. In case of irregular rhythms, five consecutive tracings were averaged. An LVOT VTI ⩽ 15 cm is commonly accepted as low and was the cut-off selected in our study. 14 Tricuspid annular plane systolic excursion (TAPSE) < 1.6 cm, and tissue Doppler imaging myocardial systolic excursion velocity (TDI S’) < 10 cm/s were considered abnormal as previously defined. 27
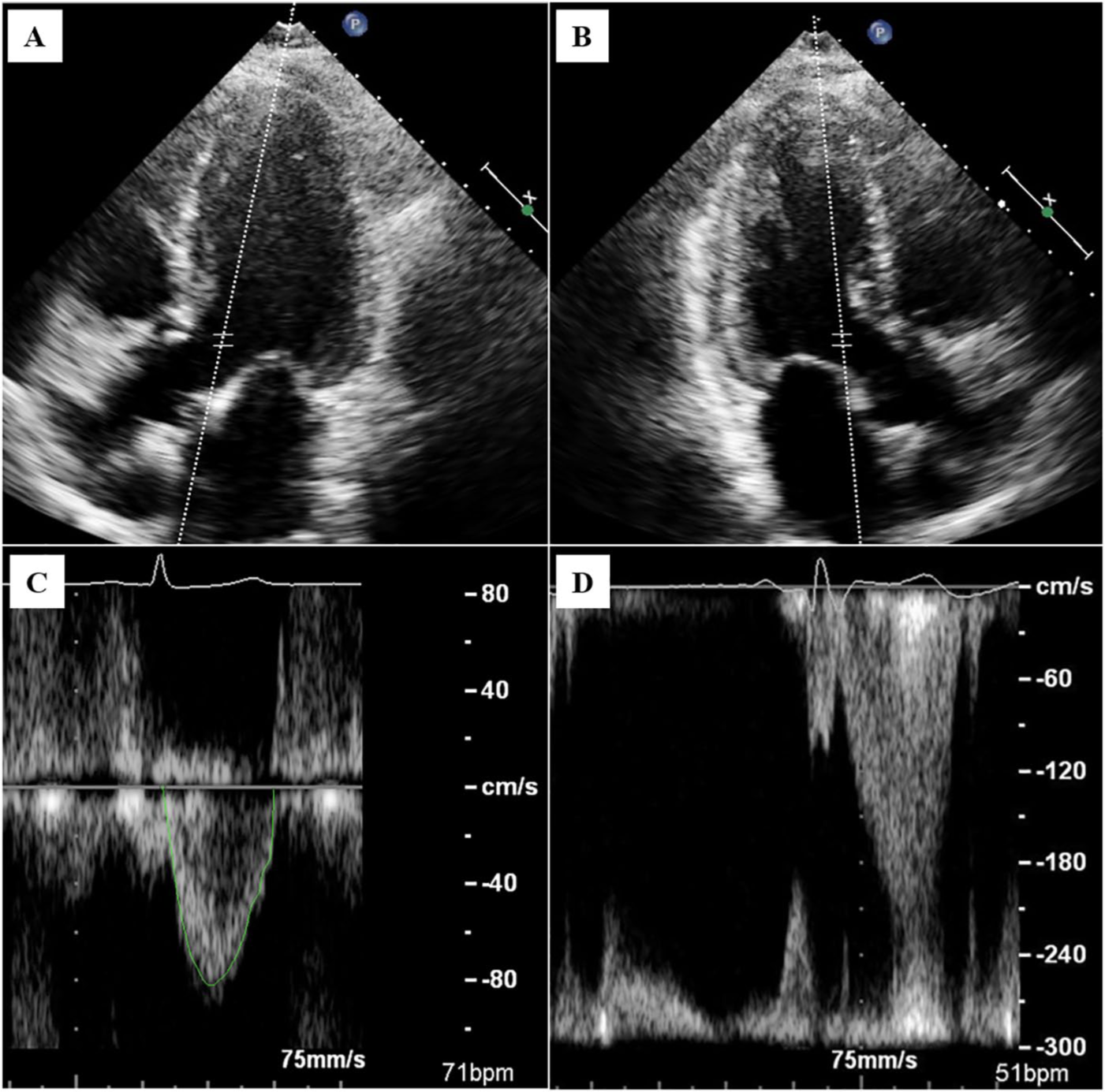
LVOT VTI image acquisition. (A) An anteriorly angulated apical four-chamber view (‘apical five-chamber’) of the LVOT (image modified to include the PW Doppler sample); (B) an apical three-chamber view of the LVOT (image modified to include the PW Doppler sample); (C) normal LVOT VTI spectral Doppler envelope tracing; (D) VTI with dynamic LVOT obstruction appearing as a high velocity, dagger-shaped flow signal with aliasing.
Outcomes and statistical analysis
We examined two composite outcomes in our study: (1) in-hospital mortality or cardiac arrest and (2) shock or need for primary reperfusion therapies. Cardiac arrest was defined as need for cardiopulmonary resuscitation documented in the chart, and shock as documented shock and administration of vasopressors or inotropes. Reperfusion therapies included systemic tissue plasminogen activator (tPA), catheter-directed therapies, and surgical embolectomy. The intermediate–high-risk subgroup was defined by an sPESI of ⩾ 1, RV dysfunction by imaging, and elevated biomarkers (either BNP, NT-proBNP, or TnI) as per European Society of Cardiology guidelines. 1
Unpaired t-tests were used to compare the means of continuous variables and chi-squared tests for categorical variables between the patients with LVOT VTI ⩽ 15 cm and those with LVOT VTI > 15 cm. We performed univariate analyses for the primary and secondary outcomes. Odds ratios (OR) and 95% CI were reported. Risk factors with p < 0.1 were selected as candidate covariates in the multivariable models. The final models for multivariable logistic regression analyses were constructed using backward variable selection including covariates with p < 0.05 in the final models. Statistical analyses were carried out in R (Version 3.5.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Of 216 PERT activations, 198 (92%) had a TTE performed at our institution. Six studies did not have VTI recorded and four patients had significant LVOTO, leaving 188 patients for the final analysis (Figure 2). TAPSE was available on 166 of 188 studies and TDI S’ on 167. TnI values were available on 179 patients and BNP or NT-proBNP on 155. Table 1 displays baseline characteristics of the total study population stratified by low VTI (⩽ 15 cm) and by VTI > 15 cm. The average patient in our study population was 57 ± 17.6 years old, 51% were female, with roughly a quarter of the patients having a history of cardiopulmonary disease or cancer. The majority of patients (n = 109, 58%) were categorized as having intermediate-risk PE based on imaging evidence of RV dysfunction or elevated biomarkers.
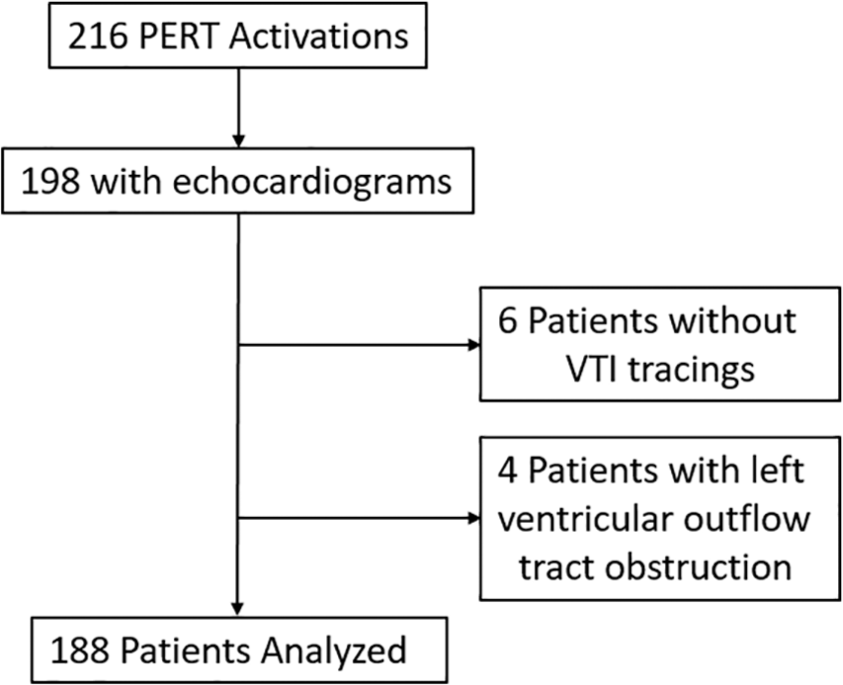
Study flow diagram.
Baseline patient characteristics.
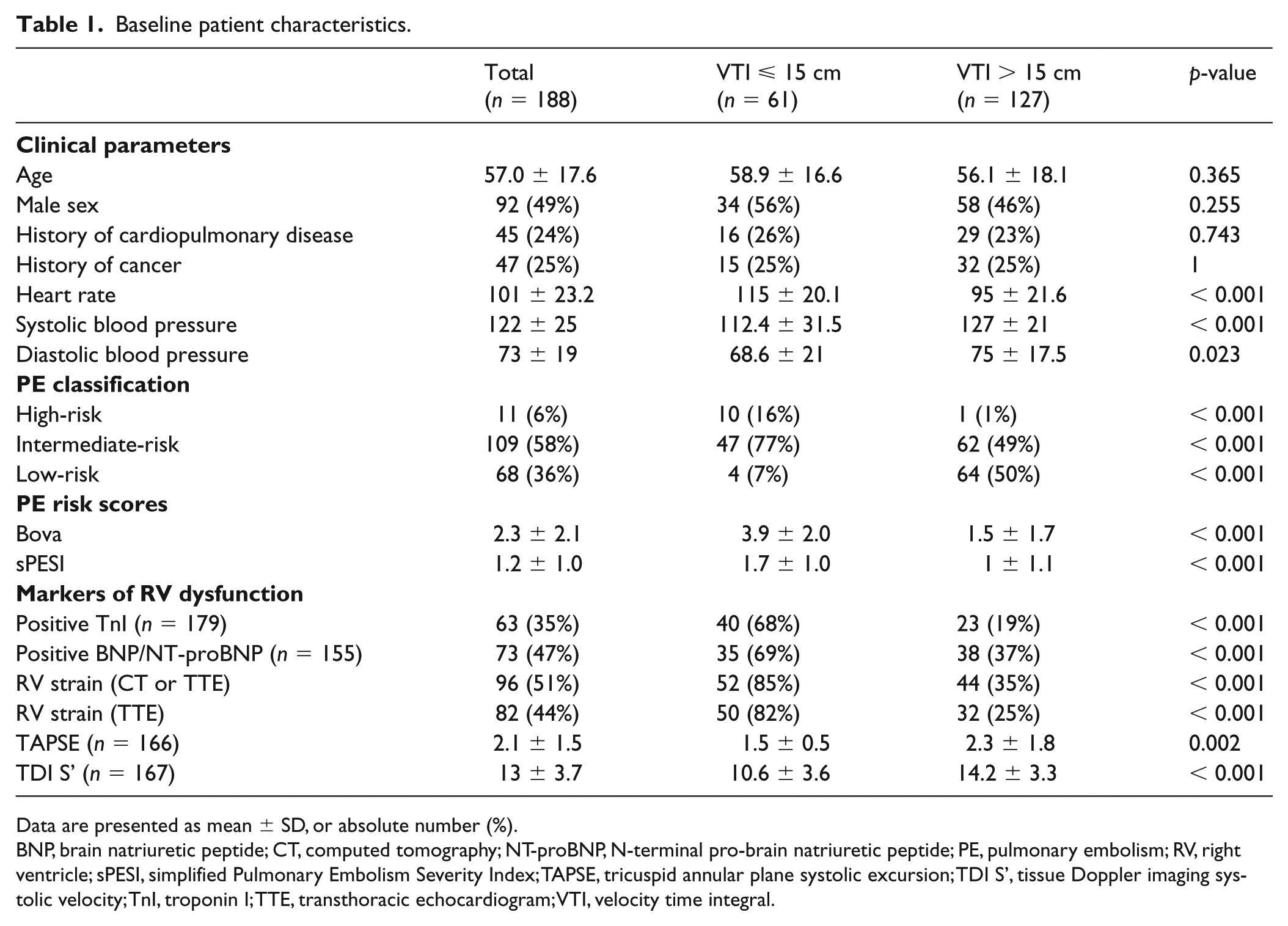
Data are presented as mean ± SD, or absolute number (%).
BNP, brain natriuretic peptide; CT, computed tomography; NT-proBNP, N-terminal pro-brain natriuretic peptide; PE, pulmonary embolism; RV, right ventricle; sPESI, simplified Pulmonary Embolism Severity Index; TAPSE, tricuspid annular plane systolic excursion; TDI S’, tissue Doppler imaging systolic velocity; TnI, troponin I; TTE, transthoracic echocardiogram; VTI, velocity time integral.
Sixty-one patients (32%) had a VTI ⩽ 15 cm and, compared to the 127 patients (68%) with VTI > 15 cm, were more likely to have RV dysfunction (85% vs 35%, p < 0.001), elevated TnI (68% vs 19%, p < 0.001), and BNP/NT-proBNP (69% vs 37%, p < 0.001). Those with low VTI represented a higher-risk cohort with higher Bova (3.9 ± 2 vs 1.5 ± 1.7, p < 0.001) and sPESI scores (1.7 ± 1 vs 1 ± 1.1, p < 0.001). Of the patients with high-risk PE (n =11, 5.9%), 10 had a low VTI while of the patients with low-risk PE (n = 68, 36.2%), only four had a low VTI.
Outcomes
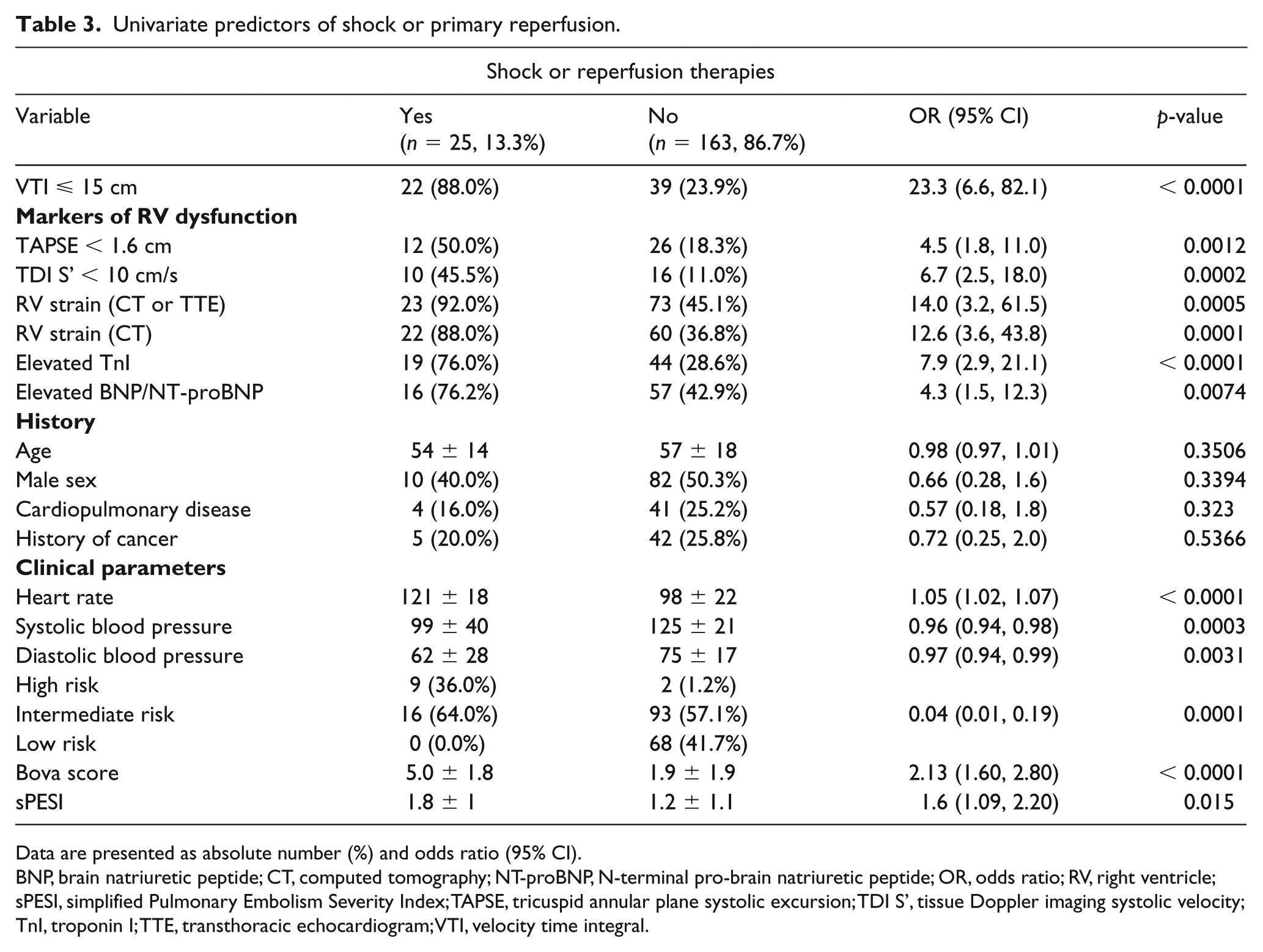
Table 2 displays clinical and echocardiographic univariate predictors of in-hospital mortality or cardiac arrest, and Table 3 of shock or need for reperfusion. A VTI ⩽ 15 cm carried an OR of 6 (95% CI 2, 17.9; p = 0.001) for the composite outcome of death or cardiac arrest, with a mean VTI of 13.4 ± 3.9 cm compared to 18.3 ± 5 cm among outcome-negative patients (p = 0.0003). Binary TAPSE (< 1.6 cm) and TDI S’ (< 10 cm/s) were not significantly associated with death or cardiac arrest. A VTI ⩽ 15 cm carried an OR of 23.3 (95% CI 6.6, 82.1; p < 0.0001) for the composite of developing shock or need for reperfusion, with a mean VTI of 12.8 ± 3.2 cm compared to a VTI of 18.6 ± 4.8 cm among outcome-negative patients (p < 0.0001).
Univariate predictors of in-hospital mortality or cardiac arrest.
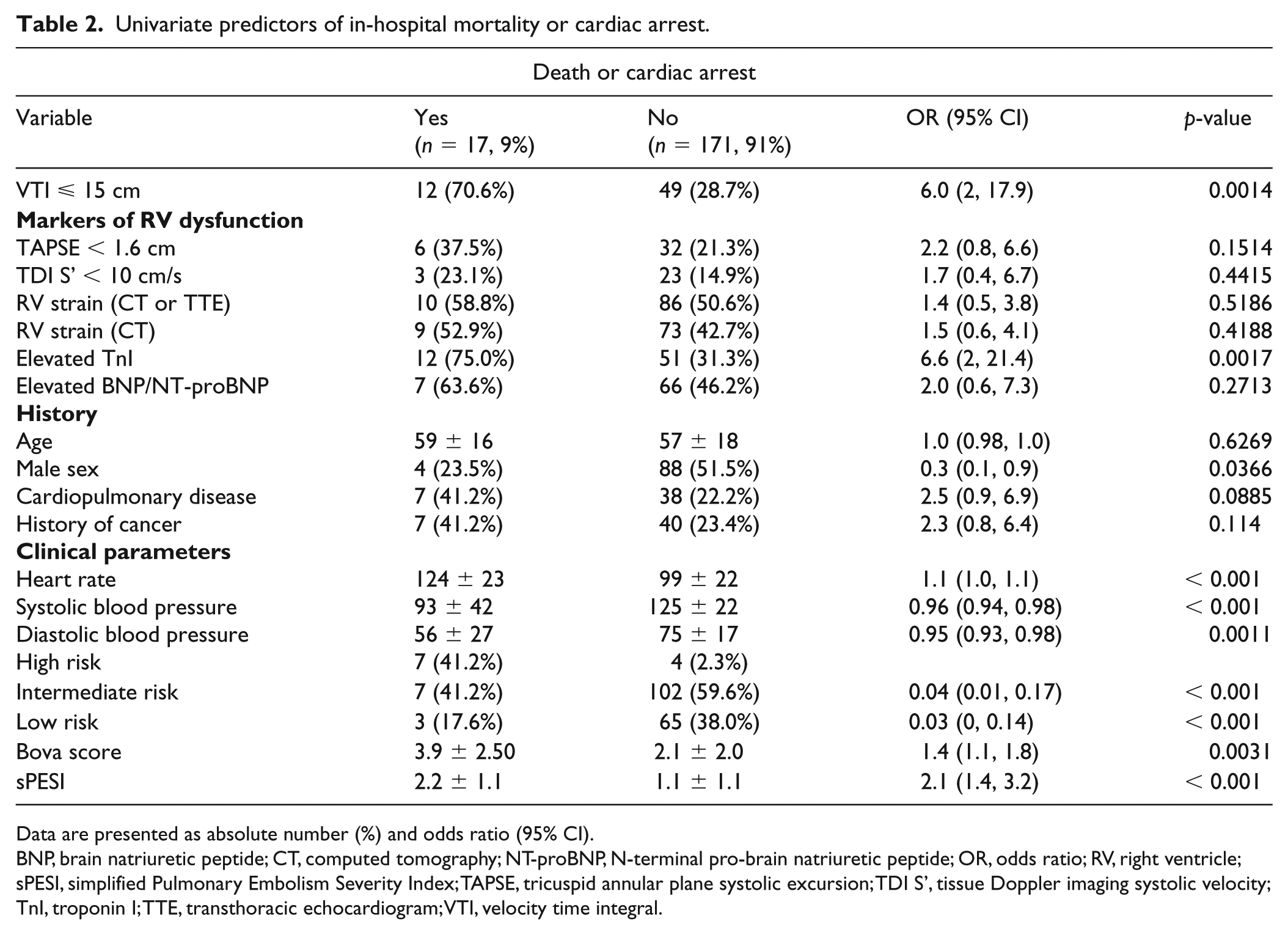
Data are presented as absolute number (%) and odds ratio (95% CI).
BNP, brain natriuretic peptide; CT, computed tomography; NT-proBNP, N-terminal pro-brain natriuretic peptide; OR, odds ratio; RV, right ventricle; sPESI, simplified Pulmonary Embolism Severity Index; TAPSE, tricuspid annular plane systolic excursion; TDI S’, tissue Doppler imaging systolic velocity; TnI, troponin I; TTE, transthoracic echocardiogram; VTI, velocity time integral.
Univariate predictors of shock or primary reperfusion.
Data are presented as absolute number (%) and odds ratio (95% CI).
BNP, brain natriuretic peptide; CT, computed tomography; NT-proBNP, N-terminal pro-brain natriuretic peptide; OR, odds ratio; RV, right ventricle; sPESI, simplified Pulmonary Embolism Severity Index; TAPSE, tricuspid annular plane systolic excursion; TDI S’, tissue Doppler imaging systolic velocity; TnI, troponin I; TTE, transthoracic echocardiogram; VTI, velocity time integral.
Multivariable analyses
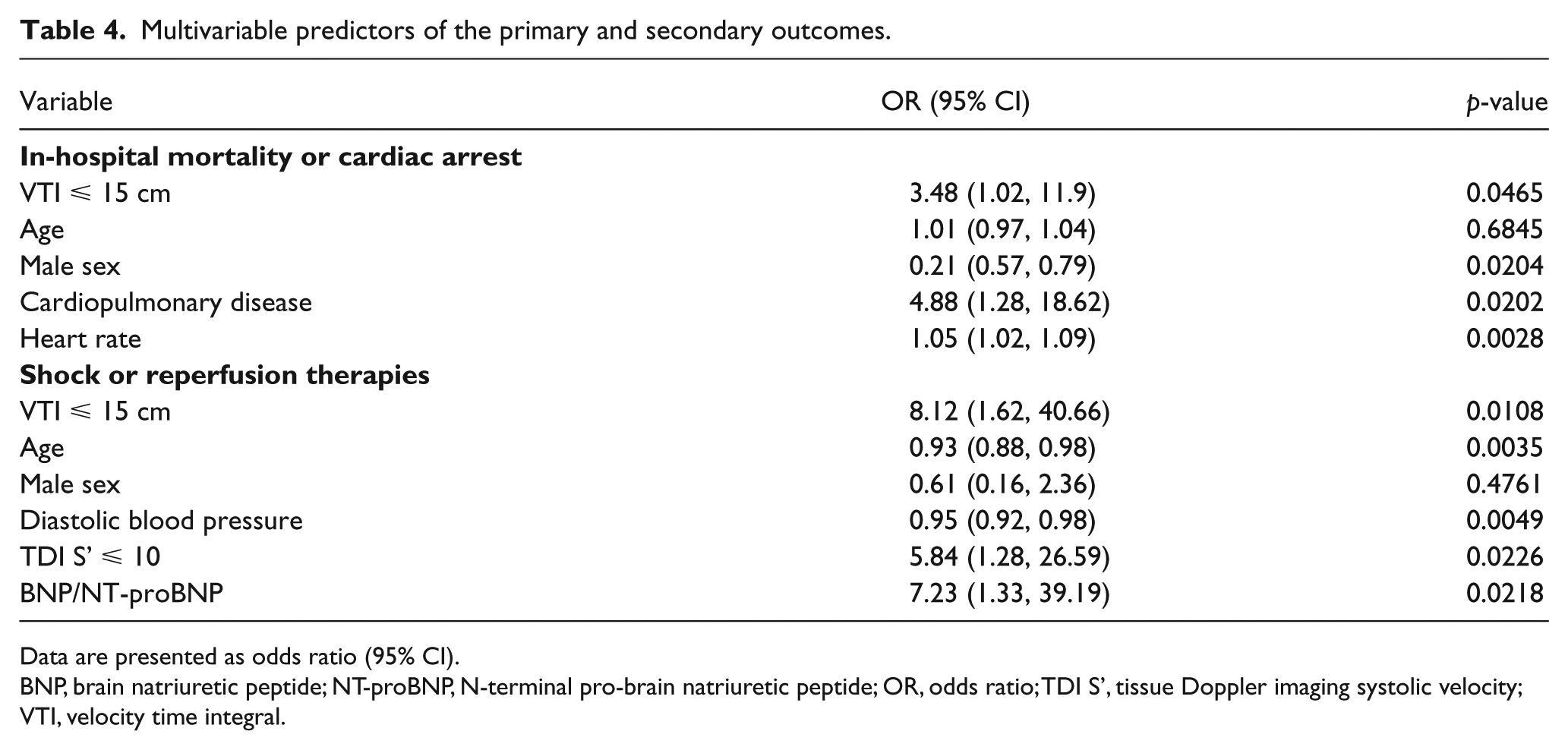
In our multivariable analysis, variables with a p-value < 0.1 from the univariate analysis were selected, and backward stepwise selection was performed. Univariates that were strongly associated with VTI were excluded. Table 4 displays the final multivariable models for the two composite outcomes. Low LVOT VTI remained significantly associated with in-hospital death or arrest (OR 3.48, 95% CI 1.02, 11.9; p = 0.047), and with shock or need for reperfusion (OR 8.12, 95% CI 1.62, 40.66; p = 0.011). In this multivariable model, low VTI was the strongest predictor of shock or need for reperfusion.
Multivariable predictors of the primary and secondary outcomes.
Data are presented as odds ratio (95% CI).
BNP, brain natriuretic peptide; NT-proBNP, N-terminal pro-brain natriuretic peptide; OR, odds ratio; TDI S’, tissue Doppler imaging systolic velocity; VTI, velocity time integral.
Intermediate–high-risk patients
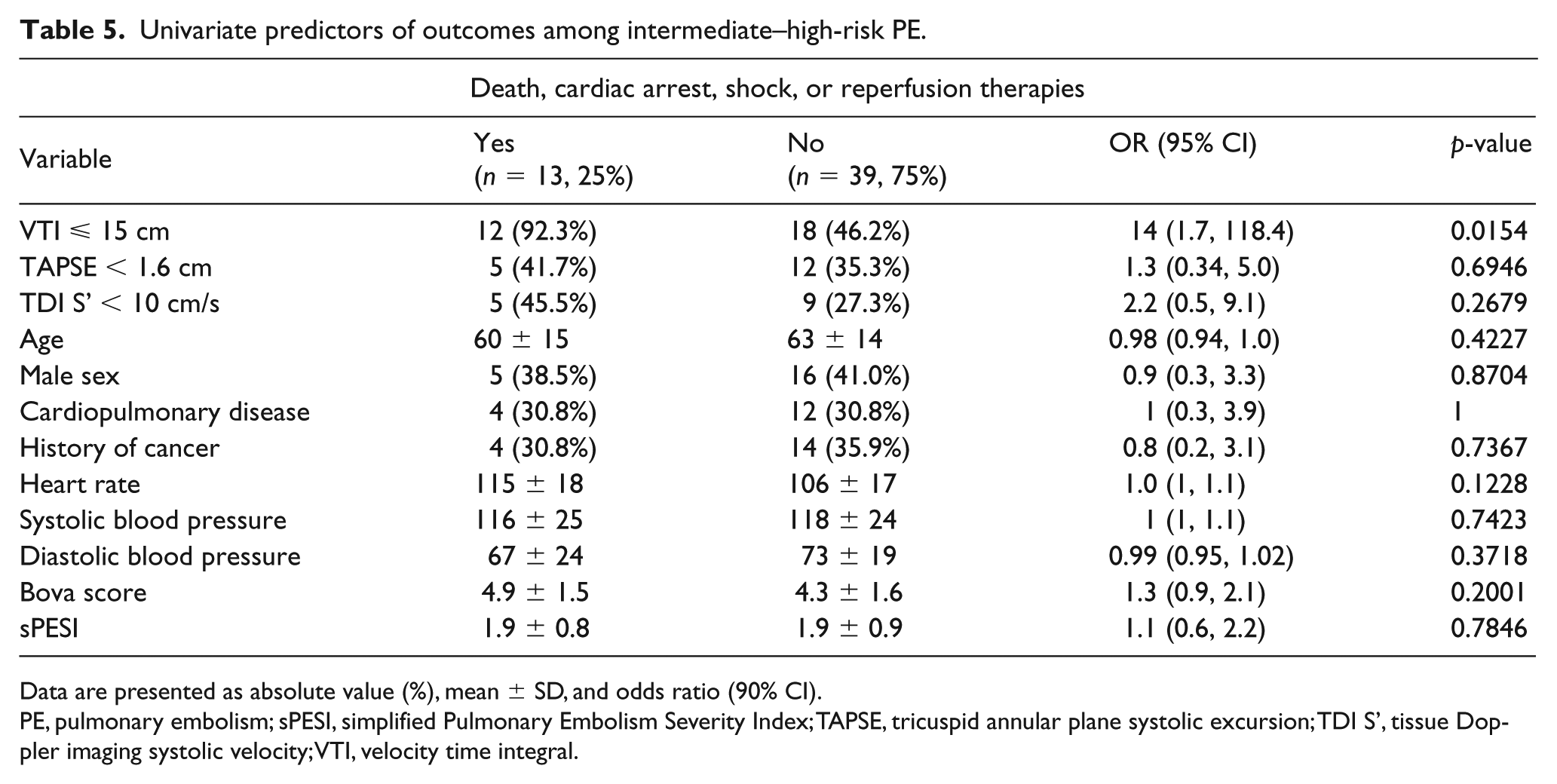
Fifty-two patients (28%) of the 188 analyzed were classified as having intermediate–high-risk PE (Table 5). Compared to those with VTI > 15 cm, those with VTI ⩽ 15 cm had similar heart rates (115 ± 18 vs 106 ± 17 beats per minute, p = 0.12), systolic blood pressures (116 ± 25 vs 118 ± 24 mmHg, p = 0.74), Bova (4.9 ± 1.5 vs 4.3 ± 1.6, p = 0.2), and sPESI scores (1.9 ± 0.8 vs 1.9 ± 0.9, p = 0.78). A VTI ⩽ 15 cm was the only predictor of the composite outcome of death, cardiac arrest, shock, or need for reperfusion in this group. Twelve of 13 patients (92.3%) reaching the composite outcome had a VTI ⩽ 15 cm while 46.2% of outcome-negative patients had a VTI ⩽ 15 cm. The average VTI among those meeting the composite outcome was 13.4 ± 1.6 cm, compared to 16.3 ± 4.5 cm among outcome-negative patients (p = 0.035). In this group, three patients died, three had cardiac arrest, and three were in shock; all these patients had a VTI ⩽ 15 cm. Twelve of the 30 patients with a VTI ⩽ 15 cm required either systemic tPA or catheter-directed therapies.
Univariate predictors of outcomes among intermediate–high-risk PE.
Data are presented as absolute value (%), mean ± SD, and odds ratio (90% CI).
PE, pulmonary embolism; sPESI, simplified Pulmonary Embolism Severity Index; TAPSE, tricuspid annular plane systolic excursion; TDI S’, tissue Doppler imaging systolic velocity; VTI, velocity time integral.
Discussion
LVOT VTI serves as a noninvasive surrogate of stroke volume; low values could identify patients with PE at increased risk for poor clinical outcomes. We demonstrated that low LVOT VTI is significantly associated with in-hospital mortality or cardiac arrest (OR 6, 95% CI 2, 17.9; p = 0.0014) and shock or need for reperfusion (OR 23.3, 95% CI 6.6, 82.1; p < 0.0001). Low VTI remained significantly associated with both composite outcomes in our multivariable model. To our knowledge, this is the first study to correlate LVOT VTI with short-term outcomes among patients with acute PE.
Among normotensive patients with acute PE, the risk of progressive hemodynamic impairment and increased risk of death may not be clinically apparent. Risk stratification scores such as sPESI and Bova can reliably identify patients with low-risk PE; however, a method to accurately identify patients at high risk for decompensation remains elusive.25,26 While echocardiographic assessment of the RV plays an important role in the evaluation of the PE patient, RV dysfunction carries only a modestly increased risk for mortality among initially hemodynamically stable patients.8,10 Consistent with some prior studies, RV strain by imaging was not associated with death or cardiac arrest in our cohort. Similarly, we did not find quantitative measures of RV dysfunction (low TAPSE and TDI S’) to be associated with death or cardiac arrest in our study.3,7,28
In our population, 85% of patients with low VTI had RV dysfunction. Likely impaired RV systolic function was contributory to low stroke volume among those patients. Similarly, 86% of patients with clinical shock had RV dysfunction; 93% of those with shock had low VTI. We postulate that patients without RV dysfunction reaching the outcome of death or cardiac arrest (41.2%) may have had a multifactorial cause of their clinical deterioration. PE in those instances may have been only partially contributory to circulatory failure resulting in low VTI. In our study, low VTI was more predictive of shock than death or arrest.
Patients with intermediate–high-risk PE present an area of management uncertainty; these patients represented 28% of our total population.1,29,30 Fifty-eight percent of intermediate–high-risk patients had low VTI. By contrast, only 5.8% of low-risk patients had low VTI. Low VTI was the only significant predictor of the composite outcome of death, cardiac arrest, shock, and need for reperfusion in this subset. The composite outcome was largely driven by need for systemic tPA or catheter-directed therapies (nine of 13 patients reaching the composite outcome). Our findings suggest that despite being normotensive, many intermediate–high-risk patients have a reduced stroke volume index and may be in subclinical shock.
The decision to perform primary reperfusion on patients with intermediate–high-risk PE requires a multidisciplinary approach. The overall clinical sense of illness, rather than any single data point, often drives the decision. We found that patients with low LVOT VTI are more likely to require reperfusion therapies. A potential explanation is those thought to be clinically most high risk, and therefore deemed appropriate for reperfusion, also are more likely to have low stroke volume. However, using reperfusion as an endpoint to our study presents a significant limitation as this is a clinical determination of the PERT. The decision to administer reperfusion therapies is one with bias and confounding; it is difficult to know if those deemed most appropriate for reperfusion were in fact the most high-risk individuals for the hard endpoints such as death or cardiac arrest. As the number of events is small in our study, eliminating this endpoint would limit our power.
LVOT VTI has several advantages over other echocardiographic risk markers in acute PE. A VTI tracing can be obtained even on technically difficult studies with poor two-dimensional imaging and is part of the standard TTE protocol. Poor-quality imaging would otherwise limit interpretation of RV function. As LVOT VTI is often part of the point-of-care ultrasound protocol in the evaluation of shock, critical care and emergency providers may have familiarity with its utility. 18
Our study was designed as a novel proof-of-concept study. However, as this was a retrospective and non-randomized analysis, a larger prospective study would be required to confirm our findings. Additionally, use of the LVOT VTI has several limitations. Dynamic LVOT obstruction in cases of hypovolemia, sepsis, or hypertrophic cardiomyopathy creates a late-peaking velocity curve rendering stroke volume calculations inaccurate (Figure 1D).19,20 Significant aortic valve insufficiency overestimates forward stroke volume as a result of increased LVOT flow; low VTI in the setting of severe aortic insufficiency is indicative of particularly low stroke volume. Irregular rhythms will produce variability in VTI and 5–10 measures should be averaged in such circumstances.
Conclusions
Low LVOT VTI is associated with adverse outcomes among patients with acute PE and may ultimately provide a noninvasive approach to identifying higher-risk individuals. VTI may also have prognostic value among patients with intermediate–high-risk PE, a subgroup in need of further risk stratification to guide management. A large proportion of these patients have a reduced stroke volume index despite being normotensive. A larger-scale prospective validation study may better define the prognostic role of LVOT VTI among this population and help guide management strategies.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Akhilesh Sista has a grant from Penumbra, which is administered through NYU School of Medicine. The other authors declared no potential conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.