
Abstract
The postexercise ankle–brachial index (ABI) is recommended in patients with normal resting ABI when peripheral artery disease (PAD) is suspected. The aims of this study were to determine the comparative diagnostic accuracy of the resting and postexercise ABI for detecting PAD, and, the effect of the presence of diabetes on these. Three methods of interpretation currently in use were also investigated: a reduction in postexercise ABI by >20% compared to resting ABI, an ABI value of ≤0.90 postexercise, or a reduction in systolic ankle pressure of >30 mmHg postexercise. This retrospective study used colour duplex ultrasound (CDU) as the reference standard. In 278 limbs (whole group), the resting ABI had an overall area under the curve (AUC) of 0.71, with the postexercise ABI yielding a similar diagnostic accuracy of AUC 0.72. In the non-diabetes group (n=171), the resting ABI had an overall AUC of 0.74 and the postexercise ABI had a similar AUC of 0.76. In the diabetes group (n=107), overall accuracy was reduced compared to the non-diabetes group, with the resting ABI having an overall AUC of 0.65 and the postexercise ABI yielding a similar accuracy with an AUC of 0.64. The overall diagnostic accuracy of the postexercise ABI for diagnosing PAD was not greatly improved compared to resting ABI. Given the lower overall diagnostic accuracy in the diabetes group, both the resting and the postexercise ABI results in diabetes populations should be interpreted with caution. There is a risk of undiagnosed disease if relying on these results alone to determine lower limb vascular status.
Keywords
Introduction
The postexercise ankle–brachial index (ABI) is frequently used alongside the resting ABI for diagnosis and monitoring of peripheral artery disease (PAD). It is also used as an indicator of functional capacity of the lower limb vasculature, 1 and, has been used as a predictor of cardiovascular morbidity and all-cause mortality.2,3 Postexercise ABI is currently recommended in populations with suspected PAD, particularly in those exhibiting symptoms with normal resting ABI.4–9 The normal protocol for performing postexercise ABI includes baseline rested ankle and brachial pressures, followed by a period of exercise either on a treadmill or by active pedal plantarflexion, then immediate repetition of ankle and brachial pressure measurements. 10 While central blood pressure will increase with exercise, a mild decrease in peripheral pressure should be seen in healthy patients in response to vasodilation of vessels to skeletal muscle. 10 In patients with PAD, a more marked drop in peripheral pressure is proposed to occur due to the vessels not responding to the increased demands of muscle tissue. 5 The interpretation of postexercise ABI varies in the literature. The American College of Cardiology/American Heart Association (ACA/AHA) guidelines recommend interpretation of pathology at a drop in postexercise ABI of >20% compared to resting ABI, or a drop in systolic ankle pressure of >30 mmHg,10,11 while some of the literature uses a postexercise ABI value of ≤0.9 as indicative of pathology.3,6
Despite regular use of postexercise ABI in vascular laboratories, there is limited evidence examining the diagnostic accuracy of this test, particularly in specific populations at risk of PAD, including those with diabetes. Diabetes populations are at higher risk of PAD, which can be difficult to detect with non-invasive vascular testing methods, 12 mostly attributed to medial arterial calcification and a predilection for distal anatomical distribution of PAD.13,14 To date, the diagnostic accuracy of the postexercise ABI for detecting PAD in people with diabetes has not be investigated.
The primary aim of this study was to determine the comparative diagnostic accuracy of the resting and postexercise ABI for PAD in people with suspected disease, with and without diabetes. In addition, the most diagnostically accurate method of interpretation of the postexercise ABI using current clinical guideline recommendations was investigated and the effect of anatomical location and severity of PAD on the sensitivity of the resting and postexercise ABI in people with and without diabetes was determined.
Methods
This retrospective diagnostic accuracy study was undertaken at Vascular Health Care, a private vascular clinic in Lake Macquarie, New South Wales, Australia. Ethical approval was obtained from the University of Newcastle Human Research Ethics Committee (H2010-1230).
Data were extracted during a clinical file audit from the consecutive records of patients referred to the clinic with suspected PAD who had undergone both resting and postexercise ABI measurements and colour duplex ultrasound (CDU). Extracted diagnostic data included CDU, resting ABI and postexercise ABI. These data, along with information on age, sex, cardiovascular risk factors, smoking status and history of foot complications were systematically extracted by two researchers (PT and AB).
Vascular testing methods
For the vascular assessments results extracted, a vascular ultrasonographer performed both index tests (resting and postexercise ABI) and the CDU reference test at the same appointment. Standard clinic protocol was followed where participants were rested in a supine position for 10 minutes prior to resting pressure measurements being undertaken in a temperature controlled room (23–25°C). 15 Participants were asked to avoid alcohol, smoking, exercise and caffeine 1 hour prior to the testing session to avoid influencing pressure measurement. Participants fasted for 12 hours prior to the testing session to limit abdominal gas to allow for visualisation of the distal aorta and iliac arteries. 16 Pressures were taken using the Parks Vascular Mini-Lab 1050-C (Parks Medical Electronics, Aloha, OR, USA), an 8.2 MHz continuous wave Doppler, a Parks standard 10 cm inflatable cuff, and an ERKA Switch blood pressure gauge (ERKA, Bad Toelz, Germany). The ankle systolic pressures of each limb were taken by placing the brachial pressure cuff around the lower leg, proximal to the medial and lateral malleoli. Both the anterior tibial and the posterior tibial artery pressures were recorded. The higher of the two was then divided by the highest brachial pressure to calculate the ABI for that limb.
The exercise protocol for the vascular laboratory consists of participants walking on a treadmill at a maximum speed of 3 km/h for up to 5 minutes at a maximum incline of 10 degrees. If the participant experienced excessive lower extremity discomfort, angina, or dyspnea, exercise was ceased. The ankle and brachial pressures were then re-recorded immediately after cessation of exercise in a supine position as described previously. CDU was then performed on the limb(s) from the distal aorta to the foot, and for this study, this was used as the reference standard.17,18 CDU was performed with either a Phillips CX-50 (Philips, Massachusetts, USA) or GE LOGIQ i (GE Healthcare, Little Chalfont, UK). The reliability of ABI measurement and CDU at the vascular laboratory has previously been shown to be adequate. 12
Statistical analysis
For calculations relating to variables of diagnostic accuracy for this study, participant data were analysed as the whole participant group, and sub-analyses were conducted for those with diabetes, (diabetes group) and those without (non-diabetes group). To compare the participant groups with and without diabetes, independent samples t-tests were performed for age and resting and postexercise ABIs. Pearson’s chi was used to compare history of smoking, severity of PAD and sex. All comparative analyses were conducted using IBM SPSS Statistics 24.0 (IBM Corp., Armonk, NY, USA) and significance was set at <0.05.
Sensitivity, specificity, positive and negative likelihood ratios for the resting ABI, and two methods of interpreting the postexercise ABI, and a set reduction in ankle systolic pressure for detecting the presence of PAD were calculated in Microsoft Excel. For the purposes of performing calculations relating to diagnostic accuracy of the ABI for this study, PAD was defined as one or more arterial segments (from iliac arteries to the pedal arteries) with ≥50% luminal stenosis indicating the presence of significant PAD.19–21 Grading of stenosis was conducted in accordance with the following criteria: 50–75% stenosis – focal increase in velocities 250 cm/sec to 350 cm/sec and greater than threefold increase in velocities; 75–99% (>75%) stenosis – focal increase in velocities >350 cm/sec, fourfold increase in velocities; occlusion – vessel well visualised, no colour or Doppler flow seen. 22 Information on the presence and extent of stenosis and medial arterial calcification was collected during CDU imaging.9,19–21 For calculations relating to the resting ABI, the diagnostic threshold for an ABI indicating PAD of ≤0.90 was used, consistent with current guidelines.9,11 The two methods of interpreting postexercise ABI values were: a reduction in postexercise ABI measurement of >20% compared to resting ABI, consistent with the ACC/AHA recommendations; and interpreting a postexercise ABI ≤0.9 as pathological. 3 ,6 In addition, a reduction of systolic ankle pressure of >30 mmHg compared to resting as being diagnostic of PAD was also investigated. Comparison of the diagnostic accuracy of the resting and postexercise ABI for the whole group, the diabetes group, and the non-diabetes group was also undertaken using receiver operating characteristic (ROC) analysis. All ROC analysis was performed using IBM SPSS Statistics 24.0.
To investigate if the anatomical location of PAD influenced sensitivity of the resting and postexercise ABI, data for both the diabetes and non-diabetes groups were then divided into distal, proximal, or both proximal and distal disease. Distal disease was defined as disease distal to, and including, the proximal popliteal artery, and proximal disease was disease from the common iliac artery to the distal superficial femoral artery. Sensitivities of the resting and postexercise ABI were then determined. The effect of disease severity on sensitivities of the resting and postexercise ABI were also calculated. Severities used in the analysis were defined as disease >50% stenosis but <75%, >75% stenosis and occlusive disease.
Results
In this study, data for 278 limbs from 160 participants including 107 limbs of people with diabetes (diabetes group) and 171 limbs of people without diabetes (non-diabetes group) were extracted. Participant characteristics are included in Table 1. Statistical comparison of the two groups showed that there were no significant differences in sex, smoking history and prevalence of PAD, or the resting and postexercise ABI measurements. There was a significant age difference between the non-diabetes group and the diabetes group (p=0.006), with the non-diabetes group having an older mean age (74.47 years vs 71.15 years).
Participant characteristics.
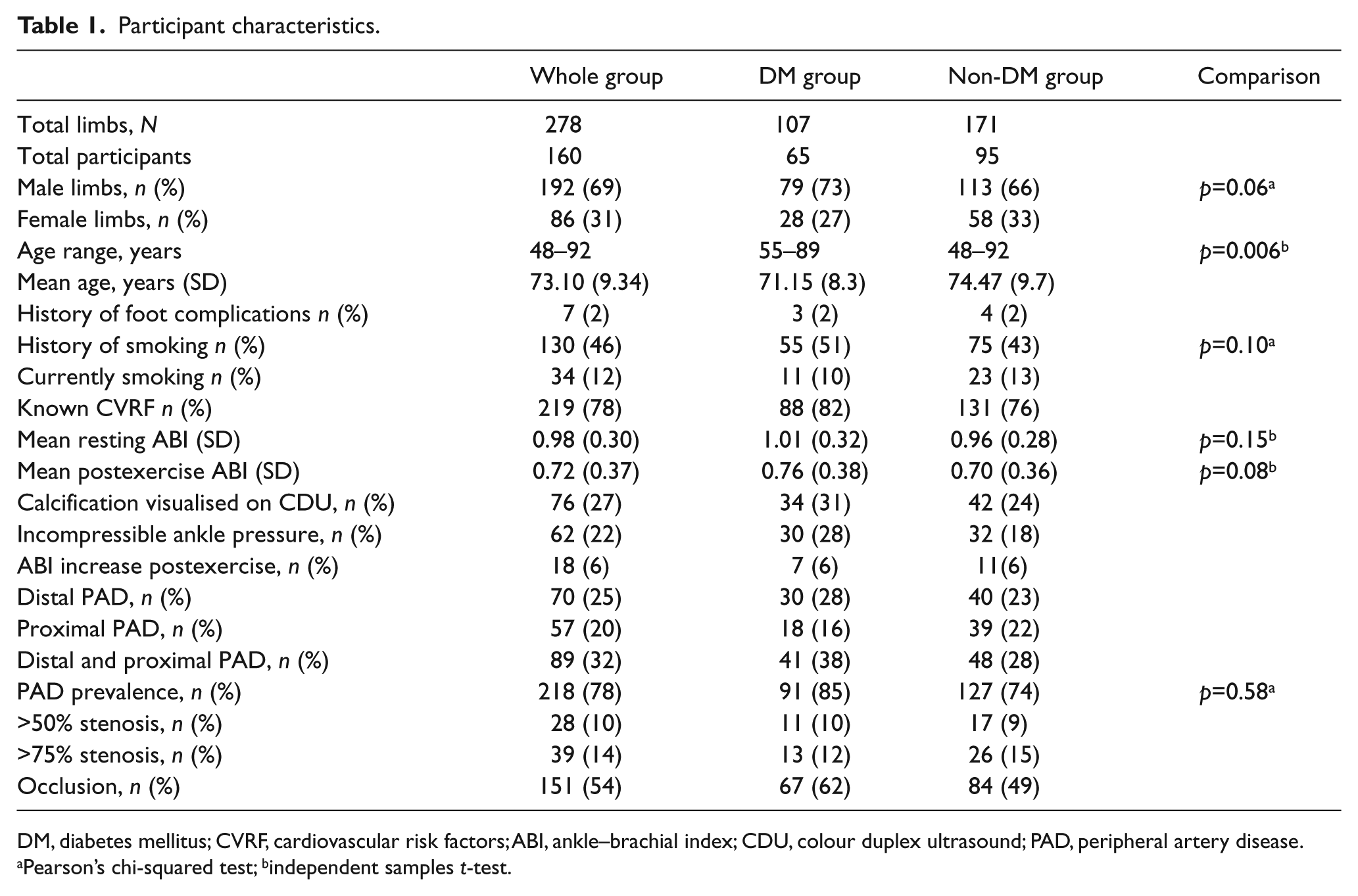
DM, diabetes mellitus; CVRF, cardiovascular risk factors; ABI, ankle–brachial index; CDU, colour duplex ultrasound; PAD, peripheral artery disease.
Pearson’s chi-squared test; bindependent samples t-test.
The mean (SD) resting ABI was 0.98 (0.30) in the whole group, 1.01 (0.32) in the diabetes group and 0.96 (0.28) in the non-diabetes group (Table 1). The postexercise ABI was 0.72 (0.37) in the whole group, 0.76 (0.38) in the diabetes group and 0.70 (0.36) in the non-diabetes group. In the whole group, 6% of participants demonstrated an increase in their postexercise ABI, 22% had incompressible ankle pressures and 27% had calcification visualised on CDU.
Sensitivity, specificity, and positive and negative likelihood ratios of the resting and postexercise ABI in the whole group and in the non-diabetes and diabetes groups are included in Table 2. The overall sensitivity for the resting ABI in detecting PAD in the whole group was 49.79% (95% CI: 43.25–56.33), with a specificity of 90.32% (95% CI: 74.25–97.96). Sub-analysis by diabetes status demonstrated the sensitivity and specificity of the resting ABI was relatively unaffected by the presence of diabetes (Table 2).
Validation table: all groups.
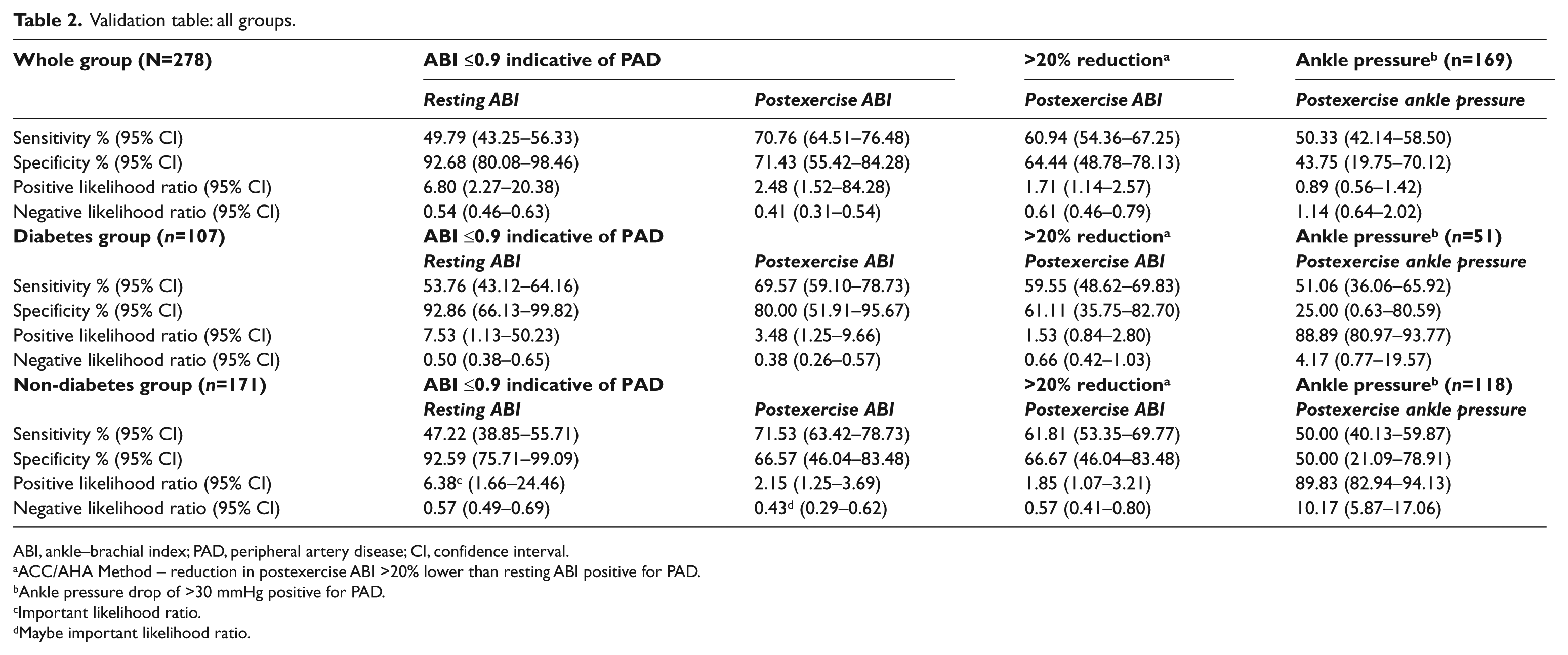
ABI, ankle–brachial index; PAD, peripheral artery disease; CI, confidence interval.
ACC/AHA Method – reduction in postexercise ABI >20% lower than resting ABI positive for PAD.
Ankle pressure drop of >30 mmHg positive for PAD.
Important likelihood ratio.
Maybe important likelihood ratio.
In regard to the two interpretation methods of postexercise ABI, a reduction in postexercise ABI measurement of >20% compared to resting ABI had a sensitivity of 60.69% and a specificity of 64.44%, with results of the subgroup analysis by diabetes status showing both sensitivity and specificity dropped slightly in the diabetes group (diabetes group: sensitivity 59.55%, specificity 61.11%; non-diabetes group: sensitivity 61.81%, specificity 66.67%). Using a postexercise ABI ≤0.9 to indicate pathology had the highest sensitivity and specificity of the two interpretation methods (70.76% and 71.43%, respectively) and generally performed better in sub-analysis by diabetes status (Table 2). Reduction of the systolic ankle pressure of >30 mmHg compared to resting was also investigated in a subset of participants and yielded an overall sensitivity of 50.33% (95% CI: 42.14–58.50) and specificity of 43.75% (95% CI: 19.75–70.12).
Analysis of resting and postexercise ABI sensitivity for PAD by anatomical location of disease showed in the whole group both the resting and the postexercise ABI ≤0.9 method had the highest sensitivity for proximal disease (resting: 76.47%, postexercise: 94.12%) (Table 3). These results were also found in the sub-analysis for the diabetes group. In the non-diabetes group, the postexercise ABI ≤0.9 method demonstrated the highest sensitivity in the proximal disease group (85.71%); however, the resting ABI was most sensitive in the distal disease group (59.09%). The >20% reduction in the postexercise ABI method had lower sensitivity than the postexercise ABI ≤0.9 method for all categories of anatomical distribution of disease but better sensitivity than the resting ABI.
Sensitivity of resting and postexercise ABI for detecting PAD in people with and without diabetes by anatomical location of PAD and PAD severity.
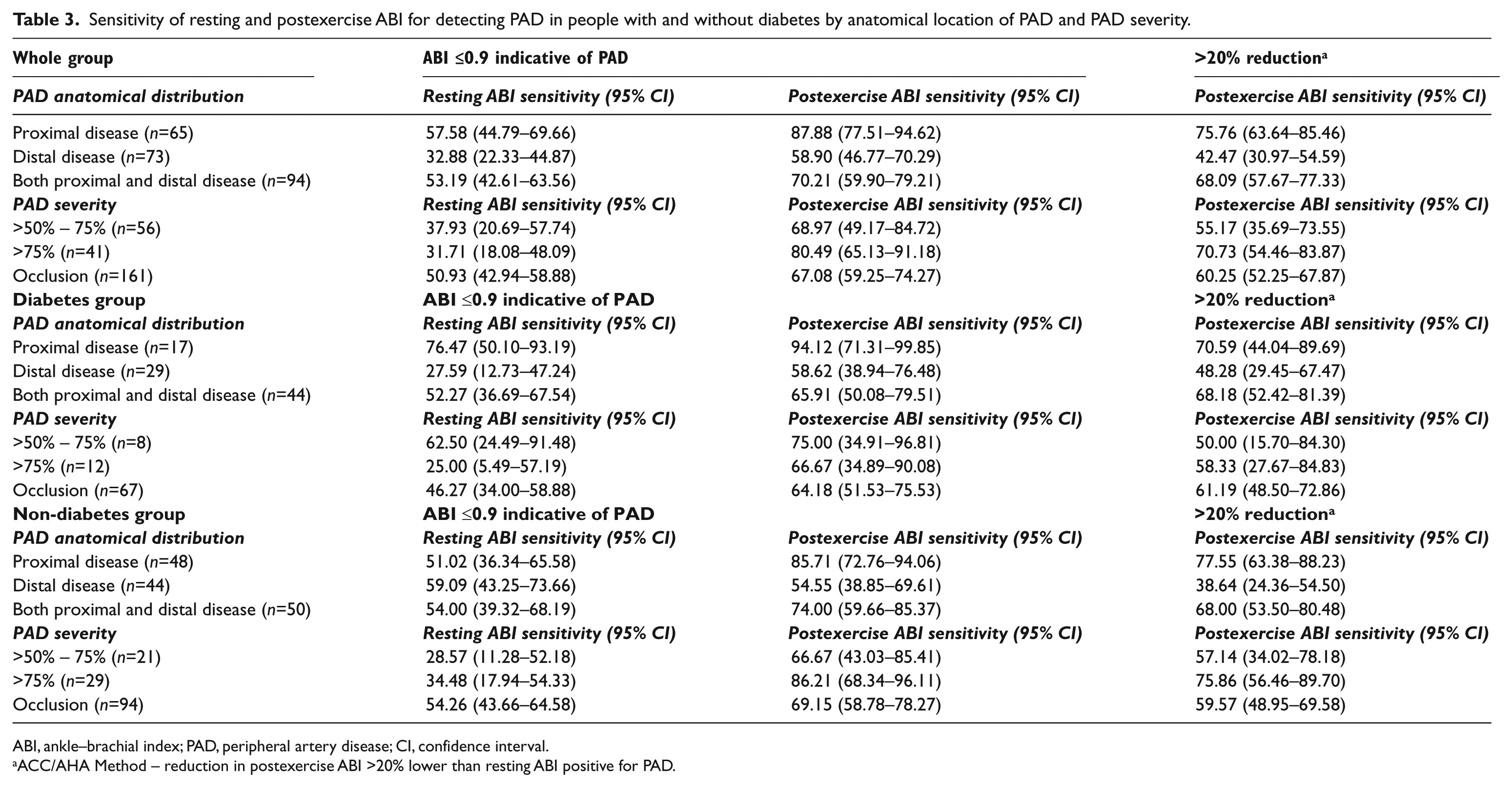
ABI, ankle–brachial index; PAD, peripheral artery disease; CI, confidence interval.
ACC/AHA Method – reduction in postexercise ABI >20% lower than resting ABI positive for PAD.
Sensitivity for detecting PAD based on severity of disease (Table 3) demonstrated the postexercise ABI ≤0.9 method had the highest sensitivity (80.49%, 95% CI: 65.13–91.18) for detecting PAD in the whole group with moderate disease (>75% stenosis). In the diabetes group, the postexercise ABI ≤0.9 method had the highest sensitivity in the mild disease group (75.00%, 95% CI: 34.91–96.81) and had higher sensitivity compared to resting ABI in all three disease severity groups overall. In the non-diabetes group, the postexercise ABI ≤0.9 method yielded the highest sensitivity in the moderate disease group (86.21%, 95%CI 68.34–96.11). Again the >20% reduction in the ABI method of interpretation generally had higher sensitivity than the resting ABI but lower sensitivity than the postexercise ABI ≤0.9 method.
ROC analyses showed that in the whole group the resting ABI (AUC: 0.71) demonstrated similar accuracy to the postexercise ABI (AUC: 0.72) (Figure 1). In the non-diabetes group (Figure 2), the resting ABI (AUC: 0.74) demonstrated similar accuracy to the postexercise ABI (AUC: 0.76). Similarly, in the diabetes group (Figure 3), the resting ABI had similar accuracy (AUC: 0.65) to postexercise ABI (AUC: 0.64). Overall the diabetes group had lower AUC values for both resting and postexercise ABI compared to the non-diabetes group. Using the ROC, output diagnostic thresholds for resting and postexercise ABI were evaluated. The resting ABI diagnostic threshold in the whole group was 1.07, in the diabetes group 1.07 and in the non-diabetes group 1.05. The postexercise ABI diagnostic threshold in the whole group was 0.88, the diabetes group 0.99 and the non-diabetes group 0.88.
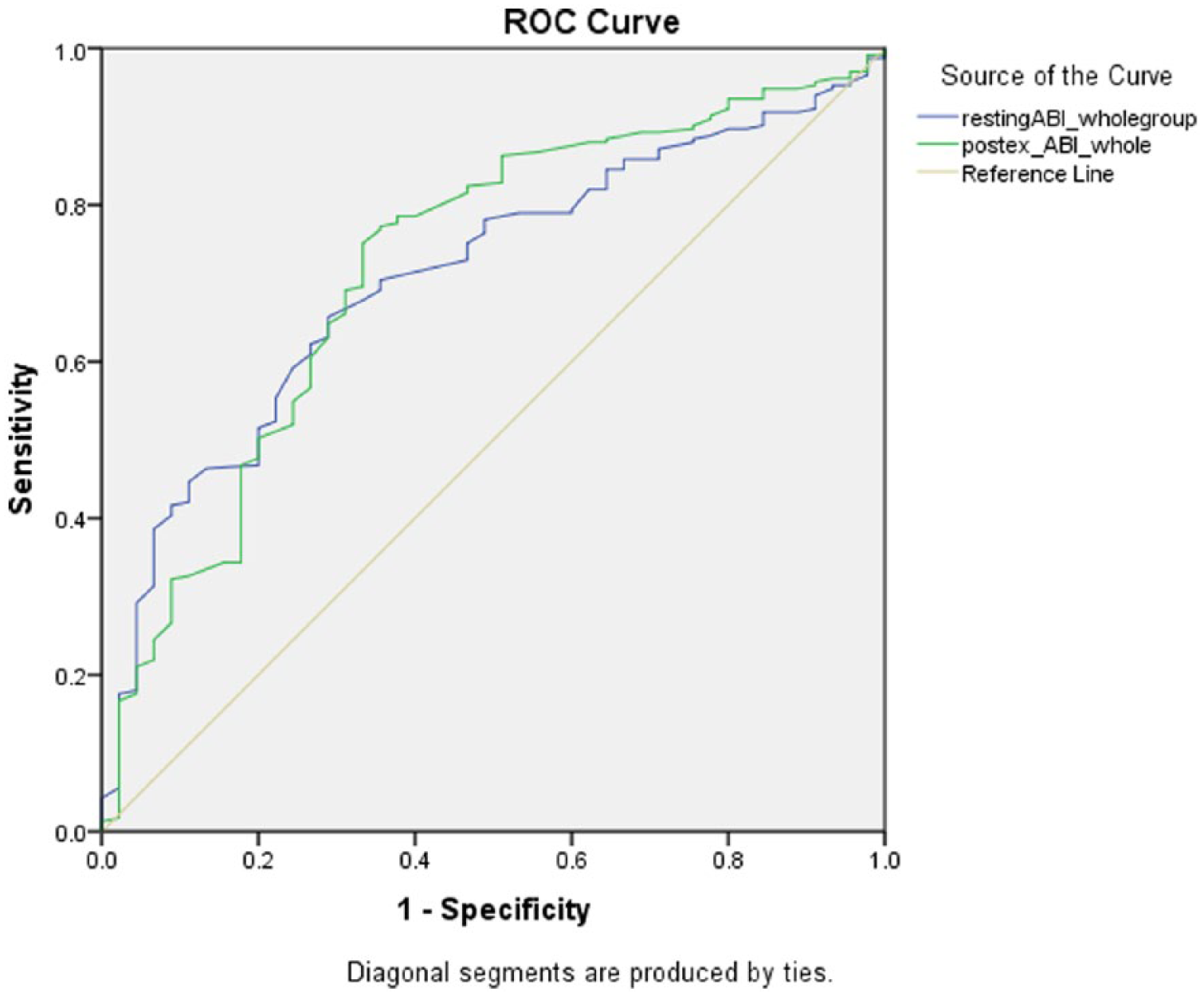
ROC analysis of resting ABI and postexercise ABI for detecting PAD in the whole group (N=278).
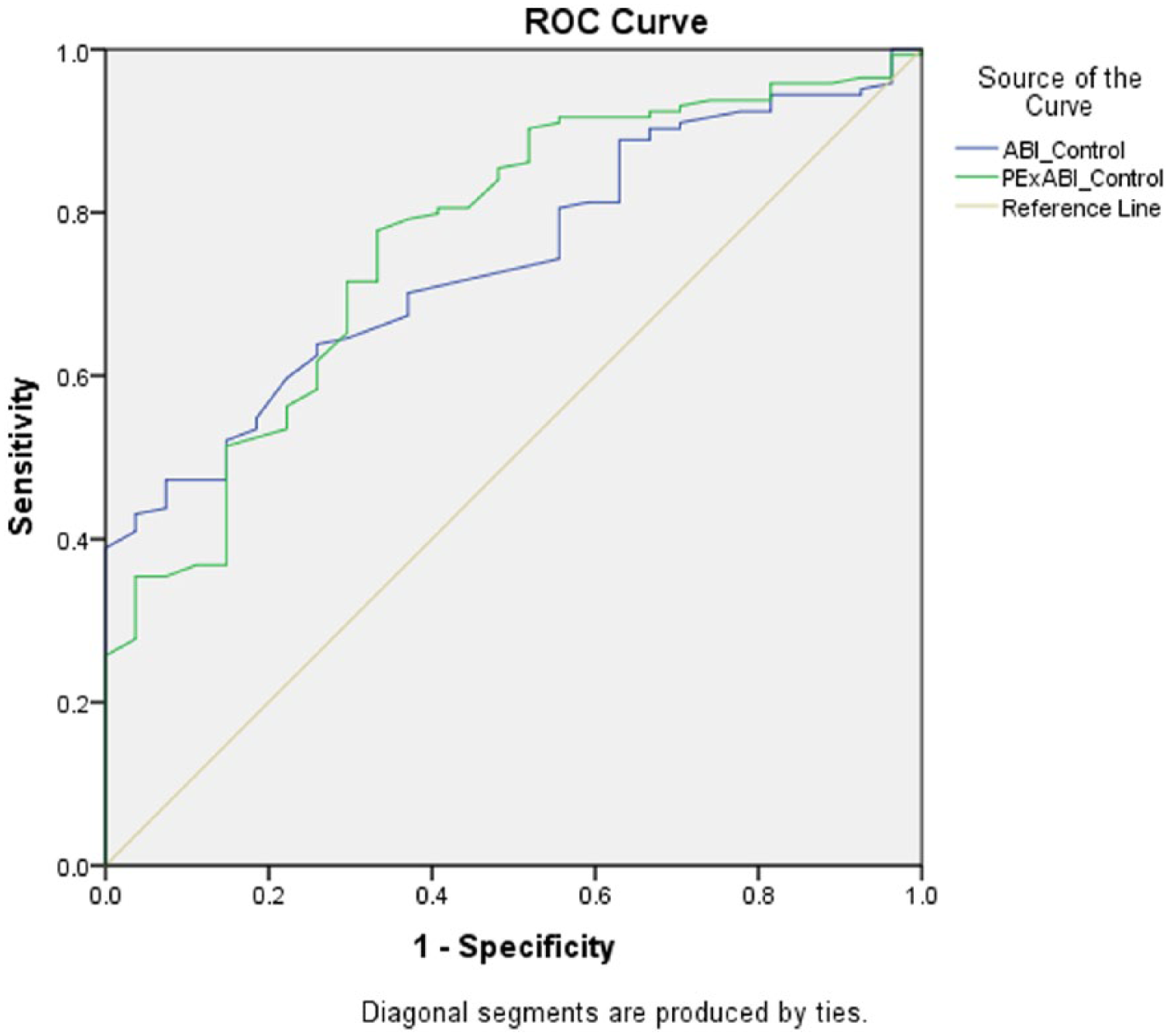
ROC analysis of resting ABI and postexercise ABI for detecting PAD in the non-diabetes subgroup (n=171).
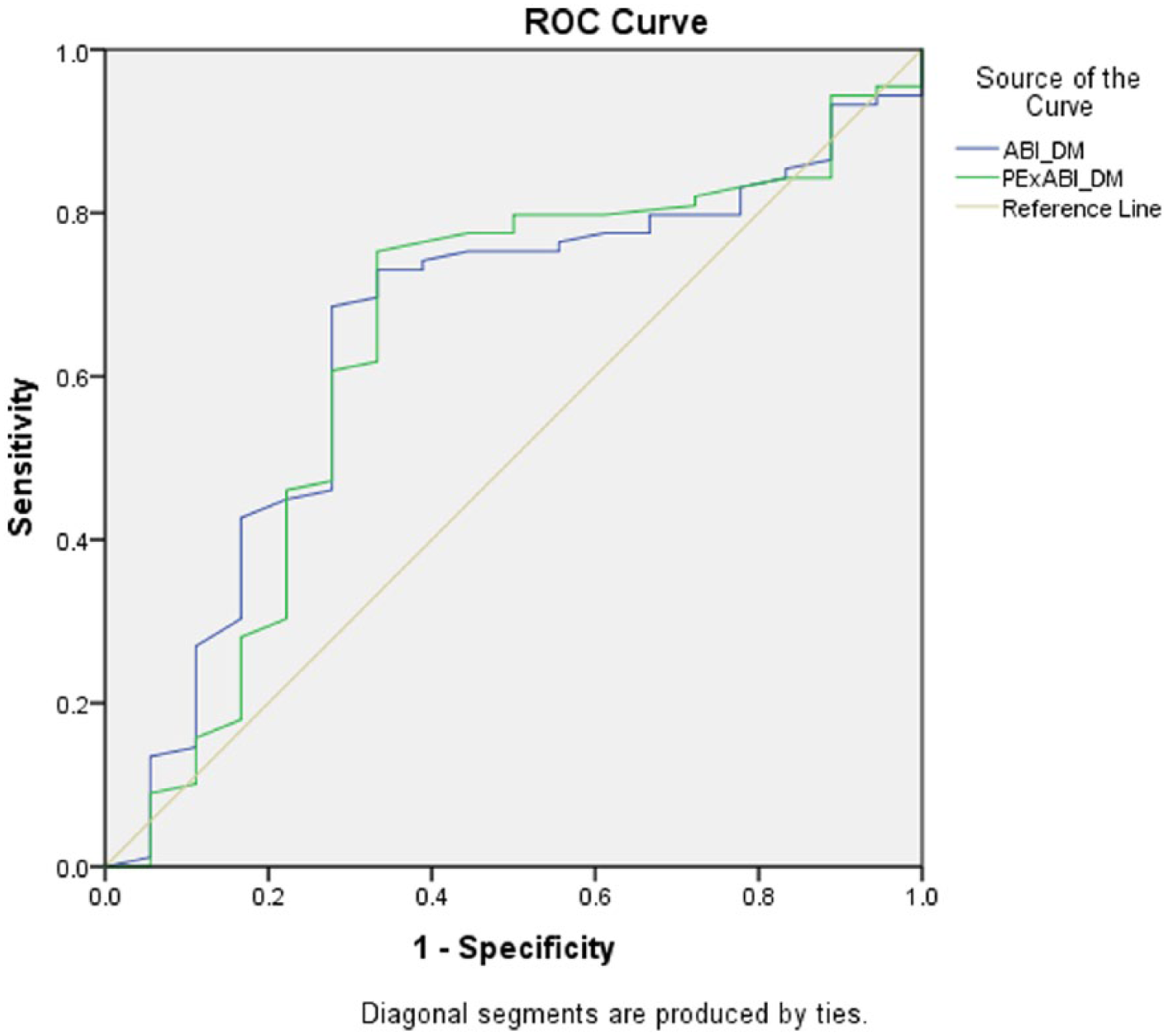
ROC analysis of resting ABI and postexercise ABI for detecting PAD in the diabetes (DM) subgroup (n=107).
Discussion
The results of this current study confirm previous research demonstrating postexercise ABI is beneficial in diagnosing PAD in patients exhibiting symptoms with a normal resting ABI.6 However, despite the postexercise ABI having higher sensitivity than the resting ABI, the overall sensitivity for the postexercise ABI to detect PAD was moderate. Notably, we have also shown that the postexercise ABI has higher sensitivity for diagnosing PAD compared to resting ABI in a population with suspected PAD, with and without diabetes. In addition, to our knowledge, this is the first study investigating different methods of interpretation of the postexercise ABI. We have demonstrated that the interpretation of the postexercise ABI relative to a threshold of ≤0.9 (sensitivity: 70.76%) was more sensitive than using a >20% reduction in ABI (sensitivity: 60.94%) as indicative of disease. Given the low mean resting ABI value in the whole group (0.98), a >20% reduction would require a significant change in brachial and/or ankle systolic blood pressure to generate a reduction of that magnitude, which may explain these results and also the generally poor sensitivity and specificity of a >30 mmHg reduction in systolic ankle pressure for PAD.
The moderate sensitivity of the postexercise ABI found in this present study is lower than a previous study examining the diagnostic accuracy of postexercise ABI;5 however, the current study used different diagnostic thresholds, a different reference standard and different populations. Of note, we found that when using the postexercise ABI <0.9 method, the test performed similarly in the diabetes and non-diabetes groups, particularly in regard to sensitivity. However, the AUC for the diabetes group was lower (AUC: 0.64) than for the non-diabetes group (AUC: 0.76), suggesting reduced utility of the test in this population. Owing to the high proportion of people with diabetes in this study, the overall performance of the ABI in the whole group would have been reduced. It is possible that the reduction in diagnostic accuracy for the postexercise ABI in people with diabetes may be associated with differences in distribution of lesions between the two groups. The diabetes group has a slightly lower prevalence of proximal disease only and higher rates of distal only disease compared to the non-diabetes group. As the ABI generally relies on a cumulative decrease in blood pressure, it is less affected by distal lesions. While this did not appear to affect the AUC for the resting ABI, which was similar to the non-diabetes group, it may be that the addition of exercise in the presence of distal lesions only (below the level of the tibial trifurcation) resulted in a lesser reduction in the ankle pressure used in the ABI calculation. This would be particularly the case if one lower leg artery was relatively unaffected by disease as this pressure would be higher and be used in the postexercise ABI calculation. In addition, it is possible that other diabetes-related complications including autonomic neuropathy and associated exercise intolerance altering vascular response to exercise also impacted the postexercise ABI sensitivity. 23 Overall, these findings suggest caution should be used when interpreting postexercise ABI values, particularly in a diabetes population, and potentially both a threshold of ≤0.9 along with the percentage change in ABI compared to resting ABI should be considered when interpreting results.
In the diabetes group and the whole group, the specificity of both methods of interpreting the postexercise ABI was lower than the resting ABI. While lower specificity increases the likelihood of a false positive diagnosis, it is more likely that the higher sensitivity will detect true disease when present. Overall, the positive and negative likelihood ratios demonstrated moderate increases in probability of the presence or absence of disease in the cases of a positive or negative test, respectively. This indicates that the postexercise ABI should be considered in the context of additional vascular assessment results rather than as a standalone assessment.
Resting ABI yielded low sensitivity in the whole group (49.79%, 95% CI: 43.25–56.33), and similarly in the diabetes (53.76%, 95% CI: 43.12–64.16) and non-diabetes (47.22%, 95% CI: 38.85–55.71) subgroups. These results are similar to previous studies in diabetes and elderly populations, where reported sensitivity varies between 20% and 70%.12,24–26 Given our population had suspected PAD, and had mostly occlusive disease severity, the low sensitivity of resting ABI is noteworthy as approximately half of these participants would have had a normal ABI result. As a significant proportion of patients with PAD present with symptoms which are atypical, or asymptomatic, 27 it is highly likely that many remain undiagnosed when using resting ABI as a primary indicator of presence of PAD.
Overall specificity of resting ABI for detecting PAD was 92.68% (95% CI: 80.08–98.46), with similar specificity in the non-diabetes group (92.59%, 95% CI: 75.71–99.09) and the diabetes group (92.86%, 95% CI: 66.13–99.82). This finding in the whole group was higher than previous studies in general cohorts 26 (83%); and similar to previous studies in diabetes cohorts which have reported sensitivity ranging from 83% to 99%. 26 These relatively high levels of specificity overall indicate that it is unlikely that resting ABI will falsely diagnose PAD, meaning a low resting ABI value will likely accurately indicate PAD.
The diagnostic threshold estimated by the ROC analysis indicated a cut-off of <1.07 in the whole group for resting ABI was ideal, which is much higher than the currently suggested ≤0.9. The postexercise ABI cut-off was much lower compared to resting at <0.88 as the indicative threshold for PAD diagnosis, which is less than a 20% reduction compared to resting and may explain why a cut-off of 0.9 was more effective in this instance.
The anatomical location of PAD influenced the sensitivity of both resting and postexercise ABI. Overall, the proximal disease group yielded the highest sensitivity for resting (57.58%) and the postexercise ABI ≤0.9 method (87.88%). The results were the same in the diabetes subgroup (94% sensitive) (Table 3). This is consistent with previous studies which have demonstrated lower diagnostic accuracy for resting ABI in detecting more distal disease in older populations. 28 Proximal vessels tend to be less affected by medial arterial calcinosis, 29 which is known to reduce the accuracy of the ABI, and may explain the higher sensitivity compared to distal disease distribution. Similar results were found in the non-diabetes group, with the postexercise ABI ≤0.9 method also yielding higher sensitivity in the proximal disease group (85%). However, due to low participant numbers in each of these subgroups, these results should be interpreted with caution.
The current study also investigated the influence of the severity of PAD on the sensitivity of the resting and postexercise ABI. Previous research has shown that the ABI has higher sensitivity in severe disease, and lower sensitivity in mild disease, 28 a finding we did not replicate. However, due to the inclusion criteria of the study, the majority of participants had severe disease, which made our subgroups of mild and moderate disease severity very small and therefore our sensitivity based on disease severity results may not be meaningful and should be interpreted with caution.
Potential limitations
The major limitation to this study was the use of CDU as the reference standard. Although CDU is used extensively clinically, and has been used in previous diagnostic accuracy studies, the gold standard reference for studies of diagnostic accuracy for PAD is angiography. CDU is operator dependent, has limitations in visualising arteries affected by medial arterial calcification, which is particularly prevalent in people with diabetes, and interpretation is variable. Our findings need to be considered in light of this and the criteria used to classify PAD in this study.
Overall, the population had a high prevalence of PAD; ideally a larger number of participants without disease would be included in a diagnostic accuracy study to prevent spectrum bias. However, given that the sample was in participants with suspected PAD, this was not possible. Therefore, it is likely our results overestimate the diagnostic accuracy of both ABI tests. In the whole sample, there was a large number of participants with diabetes, and this likely influenced the sensitivity of the ABI as well as the overall test performance (AUC) for the whole group. Although in subgroup analysis sensitivity of the ABI was similar between the diabetes and non-diabetes groups, the utility of the ABI was affected by the presence of diabetes, and the high proportion of participants with diabetes in the study would have reduced the performance in the entire sample.
There was also some variation in the amount of exercise completed by each participant in accordance with individual capacity to perform treadmill walking which may have affected the results; however, all participants fulfilled the minimum amount to achieve a physiological response. Our sample size was limited due to our inclusion criteria and the size of the vascular laboratory. Bias may have been introduced to the results as all measurements were made by the same clinician meaning that CDU was performed with knowledge of the resting and postexercise ABI results. Owing to data extraction methods, we did not have systolic ankle pressure measurements for all participants, only a subset, so this sample is smaller in size compared to the overall number of participants. Owing to this smaller subset, we were not able to include ankle systolic pressures in our analysis by anatomical location or disease severity.
Conclusion
While the addition of exercise improved the sensitivity of the ABI in individuals both with and without diabetes, the overall diagnostic accuracy of the test for diagnosing PAD was not greatly improved compared to the resting ABI. The overall accuracy of both the resting and the postexercise ABI in people with diabetes and people without diabetes was low. This suggests that both the resting ABI and the postexercise ABI results in people with and without diabetes should be interpreted with caution. Based on our findings, there is a significant risk of disease remaining undiagnosed if these results are used alone to determine lower limb vascular status.
Footnotes
Acknowledgements
A special thank you to Sean Sadler for his personal support to finalise this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this project was funded through a University of Newcastle Faculty of Health Pilot Grant and a Hunter Medical Research Institute Grant.