
Abstract
The resting ankle–brachial index (ABI) is a first-line test to diagnose peripheral artery disease (PAD). No randomized controlled trial (RCT) has yet been conducted to determine the best teaching method to become proficient in the ABI procedure. We conducted a monocentric RCT to determine whether didactic learning alone or didactic learning combined with experiential learning improved proficiency in the ABI procedure. Medical students (n = 30) received didactic learning, including (i) a presentation of the ABI guidelines and (ii) a video demonstration. Each student was then randomized into two groups (‘no experiential learning group’ and ‘experiential learning group’). An initial evaluation was performed after the didactic learning and a final evaluation at the end of the intervention. A student was considered to be proficient when he or she performed a correct ABI procedure on a healthy individual and a patient. The correct procedure corresponds to (i) following guidelines and (ii) a difference in ABI measurement between a vascular specialist and a student of ≤ 0.15. No student was proficient at the initial evaluation. At the final evaluation, in the didactic learning group, the number of proficient students was not improved compared with the initial evaluation (0/10 vs 1/10). In the experiential learning group, the number of proficient students was significantly improved (0/20 vs 11/20; p < 0.05). At the final evaluation, there was a significant difference between the number of proficient students depending on their learning group. In conclusion, didactic learning alone is insufficient to gain proficiency in the ABI procedure. Combining didactic learning with experiential learning significantly improved the students’ proficiency.
Keywords
Introduction
Peripheral artery disease (PAD) is a widespread disease affecting more than 200 million people worldwide. 1 The ankle–brachial index (ABI; ratio of the highest systolic blood pressure measured at the ankle to that measured at the brachial artery) at rest is the recommended test to diagnose PAD (i.e. ABI ≤ 0.90) and is a major inclusion criterion in PAD studies. 2 The American Heart Association (AHA) has proposed guidelines for the measurement and interpretation of the ABI, as well as the ABI learning procedure. 3 ‘Didactic and experiential learning under the supervision of a qualified and experienced health professional’ is proposed but the level of evidence remains low (Class I; Level of Evidence C) as no randomized controlled trial (RCT) has yet been conducted. 4 We conducted an RCT to determine whether didactic learning alone or didactic learning combined with experiential learning would improve proficiency in the performance of the ABI among medical students.
Methods
Study design
We conducted an RCT in France, which was approved by the ethics review board of our institution (no. 16.150). All included medical students signed an informed consent form, and healthy and patient cohorts were orally informed according to the approved study procedure.
Student training
For this study, 4th to 6th-year undergraduate medical students (18 women and 12 men), with no prior experience in the evaluation of ABI, received a specific 1-hour didactic course provided by an experienced vascular specialist, including (i) a presentation of the AHA guidelines (50 minutes) 3 and (ii) a video demonstration of the ABI procedure with a clear description of each step and emphasis on correct technique (10 minutes). In this video, a vascular specialist performs an ABI measurement on both lower extremities of a patient. The video was recorded to: (i) explain the utility of the measurement in clinical practice; (ii) describe the appropriate care of the Doppler ABI; (iii) demonstrate the location of the pulses on the arms and lower legs; (iv) listen to the quality of the pulse of arterial blood flow; (v) list the tips for effectively using the Doppler probe; (vi) calculate the ABI; and (vii) state the significance of the ABI result. Following this didactic course, the students were randomized into two groups, as illustrated in Figure 1: ‘no experiential learning group’ and ‘experiential learning group’. This latter group was randomly divided into two groups: ‘experiential learning on healthy individuals group’ and ‘experiential learning on patients group’.
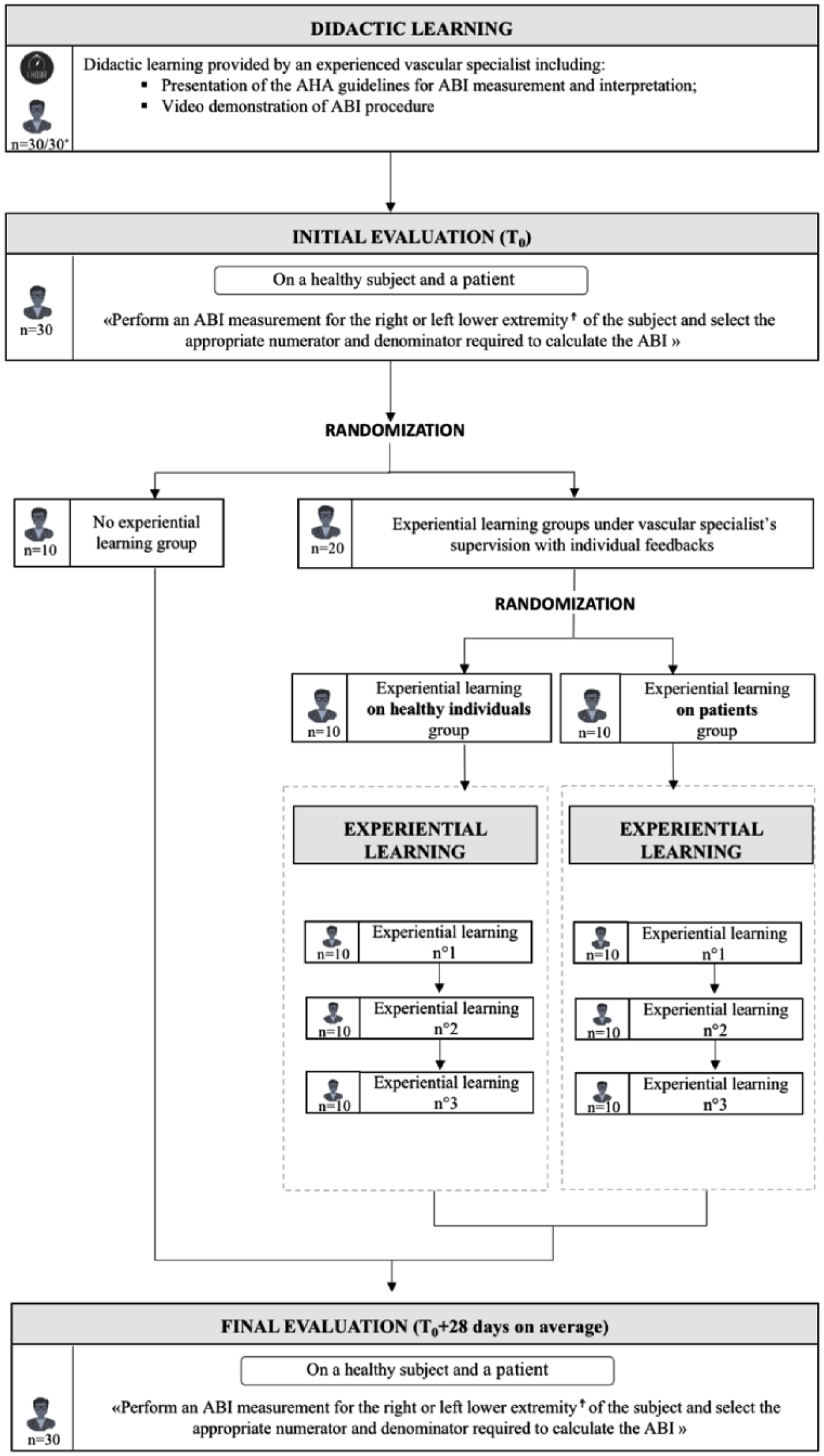
Study design flow chart.
The healthy cohort had no medical risk factors and normal ABIs, whereas the patient cohort consisted of consecutive patients admitted to the vascular unit of the university hospital of Rennes, France for an ultrasound exam. We excluded patients with recent below the knee lower extremity arterial bypass, the presence of open wounds, ulcers, or fistulae contraindicating cuff placement, or who were unable to provide oral informed consent.
For experiential learning on healthy individuals, students came three times in pairs for a 1-hour session during which students trained on one another. For experiential learning on patients, students came three times individually when a vascular ultrasound exam was programmed. For each experiential learning session, students performed an ABI measurement on both lower extremities (right and left lower extremities) of the volunteer under the vascular specialist’s supervision (i.e. seven pressures were recorded: right brachial artery, right posterior tibial artery, right dorsalis pedis artery, left posterior tibial artery, left dorsalis pedis artery, left brachial artery and right brachial artery). The equipment provided to the student included adult medium and large sized blood pressure cuffs, an 8-MHz Doppler ultrasound probe, ultrasound gel, a stethoscope, and an automatic blood pressure monitor, as previously reported by Wyatt et al. 5 Students were then instructed to calculate and interpret the ABI, according to the AHA recommendations (i.e. the ABI of each leg should be calculated by dividing the higher of the posterior tibial artery or dorsalis pedis artery pressure by the higher of the right or left arm systolic blood pressure).
During each experiential learning session, the vascular specialist identified all problems of the measuring process that may affect the accuracy of the ABI to provide pertinent and personalized feedback to the students. For example, the vascular specialist was careful with the choice or attachment of the cuff, the position and angle of the Doppler probe, or of insufficient contact via the transmission gel for the Doppler probe, which may dislocate during the measurement, and deflation of the cuff.
Immediately after completion of the ABI measurement, the vascular specialist provided (i) feedback to the students on their individual errors in performing the ABI measurement and its calculation and interpretation and (ii) a demonstration of the ABI measurement on both lower extremities of the same volunteer.
Initial and final evaluations
After the didactic course, a technician supervised an initial ABI procedure evaluation. During this evaluation, each medical student attempted to (i) perform an ABI measurement for the right or left lower limb extremity of a healthy subject, and then a patient, and (ii) select the appropriate numerator and denominator required to calculate the ABI of a hypothetical patient. One minute after the student finished, a vascular specialist blinded to the student’s ABI measurements entered the examination room and repeated the ABI measurement.
The final evaluation was performed following the same procedure.
Outcome measures
A student was considered to be proficient in performing the ABI measurement if he or she correctly performed the following procedure during the evaluation on both a healthy individual and a patient: (i) installed the patient in a supine position with the head and heels supported; (ii) used the appropriate device among the equipment provided for each participant (i.e. sphygmomanometer cuff with a width of a least 40% of the limb circumference placed just above the malleoli, an 8-MHz Doppler probe with Doppler gel applied over the probe and placed in the area of the pulse at a 45° to 60° angle to the surface of the skin); (iii) inflated the cuff progressively up to 20 mmHg above the level of flow signal disappearance and then deflated slowly to detect the pressure level at flow signal reappearance; (iv) performed the pressure measurements in the accurate order (i.e. for the right ABI measurement: right brachial artery, right posterior tibial artery, right dorsalis pedis artery, left brachial artery, and right brachial artery again); (v) recorded each pressure; (vi) selected the appropriate numerator and denominator to calculate the ABI; and (vii) obtained an accurate ABI. Even if the ABI of the student was accurate, but the pressure measurements were not performed in the correct order, or the sphygmomanometer cuff was not correctly placed, the student was not considered to be proficient.
An ABI was considered to be accurate if the difference between the ABIs measured by the vascular specialist and the student was ≤ 0.15, as previously reported.6,7 Furthermore, this cut-off was chosen since a decrease of the ABI > 0.15 over time is effective for detecting significant PAD progression, as stated in the AHA recommendations. 3 The intra-observer coefficient of variation for the ABI in our vascular laboratory is 9.4% (typical error of the estimate is 0.06).
Statistical analyses
The statistical analysis was performed using MedCalc Statistical Software version 12.6.1.0 (MedCalc Software bvba, Ostend, Belgium). A Fisher’s test was used to compare the number of students proficient in performing the ABI procedure in each group between the initial and final evaluations. Between-group comparisons were also performed at the initial and final evaluations. A two-tailed p-value < 0.05 was considered to be statistically significant.
Results
Thirty medical students were included in this RCT (Figure 1). Demographic and clinical characteristics of the patients who participated in the evaluations are presented in the online supplemental material. Of the 60 patients, 10 (17%) had diabetes mellitus, 25 (42%) dyslipidemia, 36 (60%) hypertension, 21 (35%) a kidney injury and 11 (18%) were current smokers. Thirteen (22%) had an ABI ≤ 0.90 or > 1.40.
The number of patients with an ABI ≤ 0.90 and > 1.40 was not statistically different between the groups at the initial and final evaluations. At the initial evaluation, after the didactic learning alone, no student was proficient in performing the ABI procedure.
At the final evaluation, the number of proficient students in the didactic learning group was not significantly improved compared with the initial evaluation (0/10 vs 1/10; p = non-significant; Figure 2). In the experiential learning group, the number of proficient students significantly increased (0/20 vs 11/20; p < 0.05) after three experiential ABI measurements on both lower extremities (right and left). At the final evaluation, there was a significant difference between the number of proficient students depending on their learning group (didactic alone (1/10) or didactic + experiential training (11/20)). There was no significant difference in the proficiency of the students according to their experiential learning group affiliation (healthy individuals vs patients).
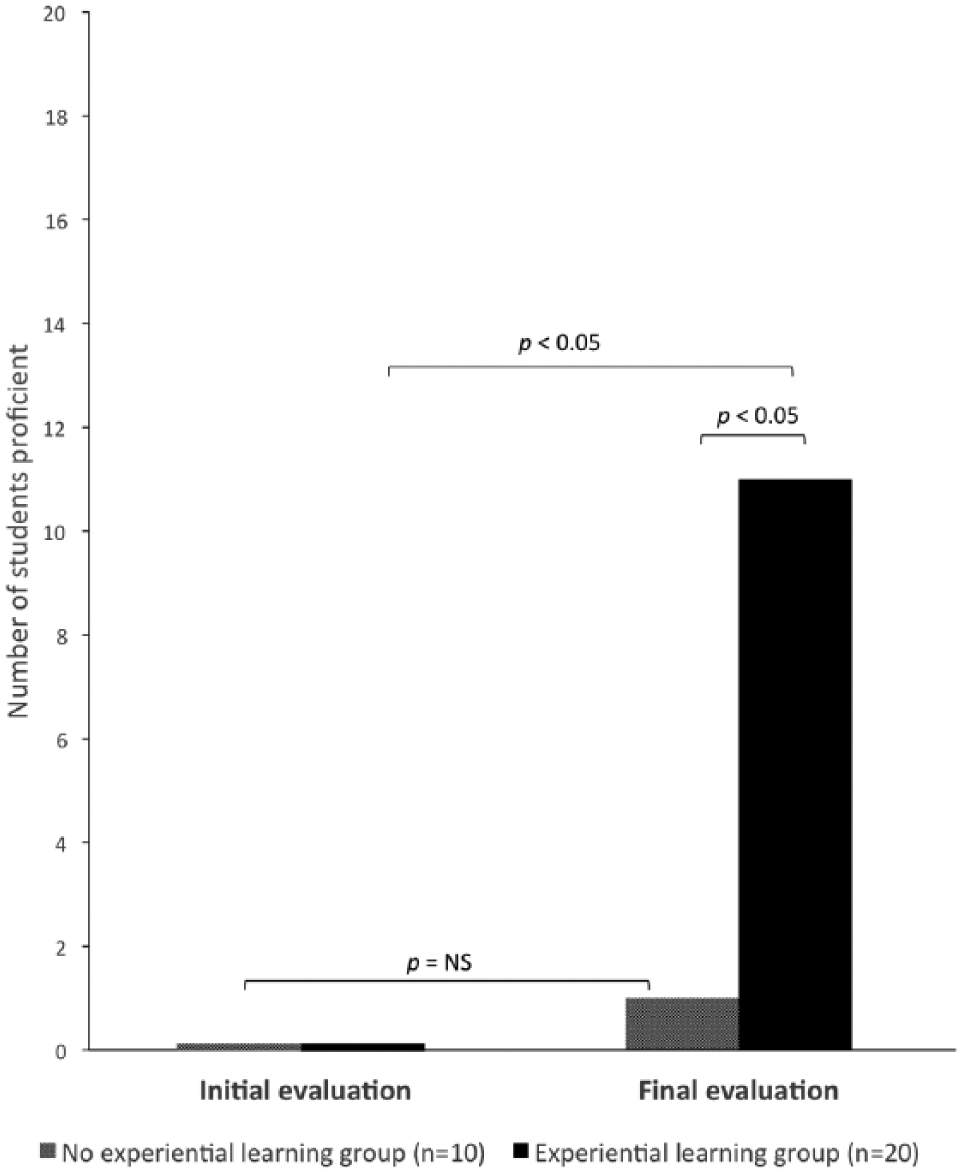
Comparison of the number of medical students proficient in performing the resting ABI procedure on healthy individuals and patients at the initial and final evaluation between the ‘no experiential learning group’ and the ‘experiential learning group’.
Discussion
ABI is an important and widely used non-invasive tool for the diagnosis of PAD and is part of the medical curriculum.8,9
Our RCT showed that (i) didactic learning alone, even with a video demonstration, is insufficient to ensure the proficiency of medical students in performing the ABI procedure, and (ii) didactic learning associated with three experiential training sessions significantly improved the students’ proficiency relative to didactic learning alone.
Teaching of the ABI procedure in major medical schools consist of only a didactic session, evaluated by questionnaire,4,10,11 which is insufficient to ensure competence with the theoretical procedure. Our RCT supports dropping didactic learning alone or combining it with experiential training.
The number of students proficient in performing the ABI procedure on both healthy individuals and patients was low (11/20), even after experiential learning. This result is in agreement with previous studies5,12 and supports the necessity to repeatedly practice ABI measurements over time to ensure the comfort and competence of the students with both the equipment and the procedure.
There was no difference in student proficiency between the two experiential learning modalities (healthy individuals vs patients). Thus, experiential learning on healthy individuals may be preferable from a practical point of view (i.e. organization, feasibility) as a first step of teaching the ABI procedure.
The strength of this study is that we used the ABI measurement value of our vascular specialists as a ‘gold standard’ for comparison with the measurements performed by the students.
Limitations
This study had some limitations. First, students in the ‘no experiential learning group’ received only 1 hour of didactic learning. It cannot be excluded that repeat didactic learning might have improved the final proficiency of the students in measuring the ABI. However, following only one didactic course corresponds to current practice in most French medical schools. 9 The present study confirms that such learning is insufficient and experiential training should be performed, as suggested by other studies.5,12
Second, the absence of a difference in the students’ proficiency between the two experiential learning modalities must be considered with respect to the clinical characteristics of the patients in the final evaluation (ABI values between 0.58 and >1.40; see the online supplemental material), since it is more difficult to measure an ABI in severe PAD patients. 12 However, our aim was to determine the best teaching method to diagnose PAD and not to train vascular specialists.
Conclusion
Didactic learning alone is insufficient for proficiency in performing the ABI procedure on both healthy individuals and patients; it should be combined with experiential learning (on healthy individuals or patients). Further studies are needed to: (i) determine the minimal amount of experiential learning required to be proficient; (ii) assess the effect of experiential learning modalities (healthy individual vs patient) on a larger population; and (iii) evaluate the students’ proficiency in a follow-up study.
Footnotes
Acknowledgements
The authors thank Awenig Carel, Marielle Delalande, Virginie Jégou, Philippe Landreau and Mathilde Ouvrard for their technical help. S. Chaudru has received a grant from the region ‘Bretagne’ (Bourse ARED).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.