
Abstract
We examined how pain beliefs are related to symptom severity, expectations of risk/benefits, and baseline physical activity among claudicants. Eligible patients at the Michael E DeBakey Veterans Affairs Medical Center were administered questionnaires that measured: fear-avoidance beliefs (Fear-Avoidance Beliefs Questionnaire [FABQ]), walking impairment, baseline physical activity, claudication type, and risk/benefit attitudes. Among 20 participants, the median age was 69 years (IQR: 66–75). In our efforts to understand how fear-avoidance beliefs influenced physical activity among people with claudication, we found that 12 out of 19 participants (63%) thought that the primary etiology of their pain was walking, while 18 (out of 20) (90%) people thought that walking would exacerbate their leg symptoms – suggesting that there was some confusion regarding the effects of walking on claudication. Those who expected that walking would benefit their symptoms more than surgery reported fewer fear-avoidance beliefs (p=0.01), but those who believed that walking would make their leg pain worse expected greater benefit from surgery (p=0.02). As symptom severity increased, fear-avoidance beliefs also increased (p=0.001). The association between symptom severity and fear-avoidance beliefs indicates that as pain or impairment increases, the likelihood of avoiding behaviors that are thought to cause pain might also increase. Accounting for pain-related beliefs when recommending physical activity for claudication should be considered.
Introduction
Claudication – a symptom of peripheral artery disease (PAD) in the lower extremities – is characterized by pain that is initiated during walking and relieved at rest. While the prevalence of claudication is lower in people younger than 50 years, it more than triples as age increases (2.2–7.7%).1,2 Compared to those without claudication, people with claudication can walk about half as far as their peers. 3 Primary management for claudication is a recommendation to walk for at least 30 minutes every day 4 in addition to addressing common coexisting conditions and smoking cessation.5–9 In supervised environments, the benefits of physical activity for claudication have been well-established.10,11 However, in most healthcare facilities in the United States, supervised exercise programs are uncommon. Home-based or community-based walking obviates the need for supervised programs while offering similar symptom improvement benefits at lower resource and time costs. As a result, efforts to encourage home-based walking initiatives have been examined and are currently being implemented.12–21 While the efficacy of home-based walking is comparable to supervised exercise, adherence to walking recommendations in both programs remains low.14,15 Few studies have examined the underlying reasons for exercise-adherence failure among claudicants.
Claudication is a symptom that manifests as pain, which has physiologic sources and is also a subjective experience; therefore, in addition to accounting for the pathology of the disease, it is advisable to consider any psychological associations.22,23 The importance of pain, pain beliefs, and its impact on treatment uptake has been examined in the low-back pain and osteoarthritis literature.24–30 One model that describes the influence of pain beliefs on behavior is the fear-avoidance model (FAM). 31 The model postulates that individuals may fear and/or avoid specific behaviors based on negative beliefs and misunderstanding of information.24,31 In this study, we examined what people with claudication thought and understood about their leg pain, how it was related to their symptom severity, how their expectations of risk/benefits were affected, and whether their baseline physical activity was associated with any of these beliefs. One hypothesis of this study was that as fear-avoidance belief scores increased, baseline physical activity would decrease. Similarly, as fear-avoidance belief scores increase, an increase in self-reported symptom severity was expected.
Methods
Study participants
The study was conducted at the Michael E DeBakey Veterans Affairs Medical Center in Houston, Texas. Individuals were included in this study if they were referred for initial appointments at the vascular surgery clinic, diagnosed with claudication, and were adults older than 18 years of age. At the time of study participation, all subjects (except one) in this study had not received surgical intervention for PAD – this was confirmed through the medical record. If they consented, participants were called 1–2 weeks before their initial vascular surgery appointment for survey administration. A diagnosis of claudication was defined as: exertional pain in the leg that was relieved by rest and an ankle–brachial index (ABI) of 0.9 or less. Diagnosis of claudication was confirmed by a board-certified vascular surgeon. Individuals were excluded if they presented with rest pain and a toe pressure of less than 50 mmHg. Those with non-healing wounds that were present for more than 2 weeks were also excluded. We received approval to conduct this study from the Baylor College of Medicine’s Institutional Review Board (IRB) and the Michael E DeBakey Veterans Affairs Medical Center Research & Development Committee. Since the survey in this study was administered over the phone, a waiver of written consent was also sought after and approved by the IRB. To participate in this study, all participants provided verbal, informed consent.
Study measures
Pain beliefs and perceptions
The Fear-Avoidance Beliefs Questionnaire (FABQ) was used to assess whether participants avoided behaviors that were perceived to cause pain due to negative beliefs and misunderstood information. 31 Based on theories of fear and avoidance behavior, this validated measure evaluated participant beliefs regarding physical activity and work. We modified this questionnaire to reflect the pain-affected areas of our target population. For example, participants were asked whether they thought that physical activity might harm their legs and whether they felt that activity made their leg pain worse. The FABQ consists of two parts: physical activity (FAB-PA) and work (FAB-W). Based on the scoring guidelines, specific questions from each scale were summed and total scores were calculated. Increasing scores correspond with increasing levels of fear-avoidance belief.
Physical activity
Daily activity was measured using the Physical Activity Scale for the Elderly (PASE) – a validated instrument that shows significant (p<0.01) correlations between questionnaire responses and quantitative data (pedometers). 32 Scores specific to participating in a type of activity (i.e. leisure-time, household, and work-related) and empirically derived weights were multiplied. The products were then added together for a total PASE score. 33
Type of claudication pain
Type of claudication pain was classified into: exertional/rest, non-calf, atypical calf, and classic claudication using the San Diego Claudication Questionnaire. 34
Symptom severity
From the Walking Impairment Questionnaire (WIQ), the distance and speed sub-scales were used to measure symptom severity. 35 Each sub-scale score was weighted based on the difficulty of the task and divided by the maximum possible weighted score. 36
Risk/benefit attitudes
First, we measured expected improvement at pre-determined levels of risk. Participants were asked how much improvement they presume at levels of risk that were both hypothetical (2% and 10%) and evidence-based (4% 37 ). Then, using previous estimates of the long-term risk of major amputations after revascularization, 37 study participants were asked open-ended questions about how much symptom improvement they would expect for surgical intervention compared to physical activity. Finally, acceptable risks were assessed in the context of possible symptom improvement levels. Participants were presented with four potential levels of symptom improvement – 100%, 75%, 50%, and 35% – and asked how much risk they were willing to accept at each level.
Medical history and demographics were collected from the electronic medical record and included: age, race/ethnicity, sex, and history of hypertension, hyperlipidemia, diabetes mellitus, and chronic obstructive pulmonary disease. Data on tobacco use (history of smoking or current smoking), ABIs, and toe pressures were also collected.
Statistical analysis
Medians, proportions, and interquartile ranges (IQR) were used to describe the spread and distribution of the data. Ordinal values were compared using the Pearson’s χ2, Fisher’s exact, and the non-parametric equality of medians tests. Between-variable correlations were also examined. Fear-avoidance belief scores (total and sub-scale scores) were examined as a continuous variable in a linear regression. Unadjusted relationships between fear-avoidance beliefs and baseline physical activity were examined in addition to expected symptom improvement (physical activity and surgical intervention), expected improvement at different risk levels (2%, 4%, and 10%), and acceptable risk at different symptom improvement levels (100%, 75%, 50%, and 35%). Stata IC version 13.0 (StataCorp, College Station, TX, USA) was used to conduct all analyses. A p-value < 0.05 was considered statistically significant.
Results
Over the course of this study (February – August 2016), 20 participants were enrolled and provided responses to the survey. Four participants (20%) reported bilateral claudication and the type of claudication pain was evenly split between exertional pain (n=10, 50%) and classic claudication (n=10, 50%). The median body mass index (BMI) in this cohort was 28 (IQR: 20–30). Five participants (25%) reported a history of chronic obstructive pulmonary disease. A majority of participants reported a history of hypertension (n=16, 80%) and/or hyperlipidemia (n=12, 60%). Ten participants (50%) reported a history of both hypertension and hyperlipidemia. Three risk factors of PAD (hypertension, hyperlipidemia, and diabetes mellitus) were present in four participants (20%). The distribution of comorbidities and factors measured by the survey is presented in Table 1. In order to enlist, the Armed Services require that individuals have at least a high school diploma. Thus, the Veterans in our cohort have completed a high school education.
Baseline descriptive characteristics of study participants.
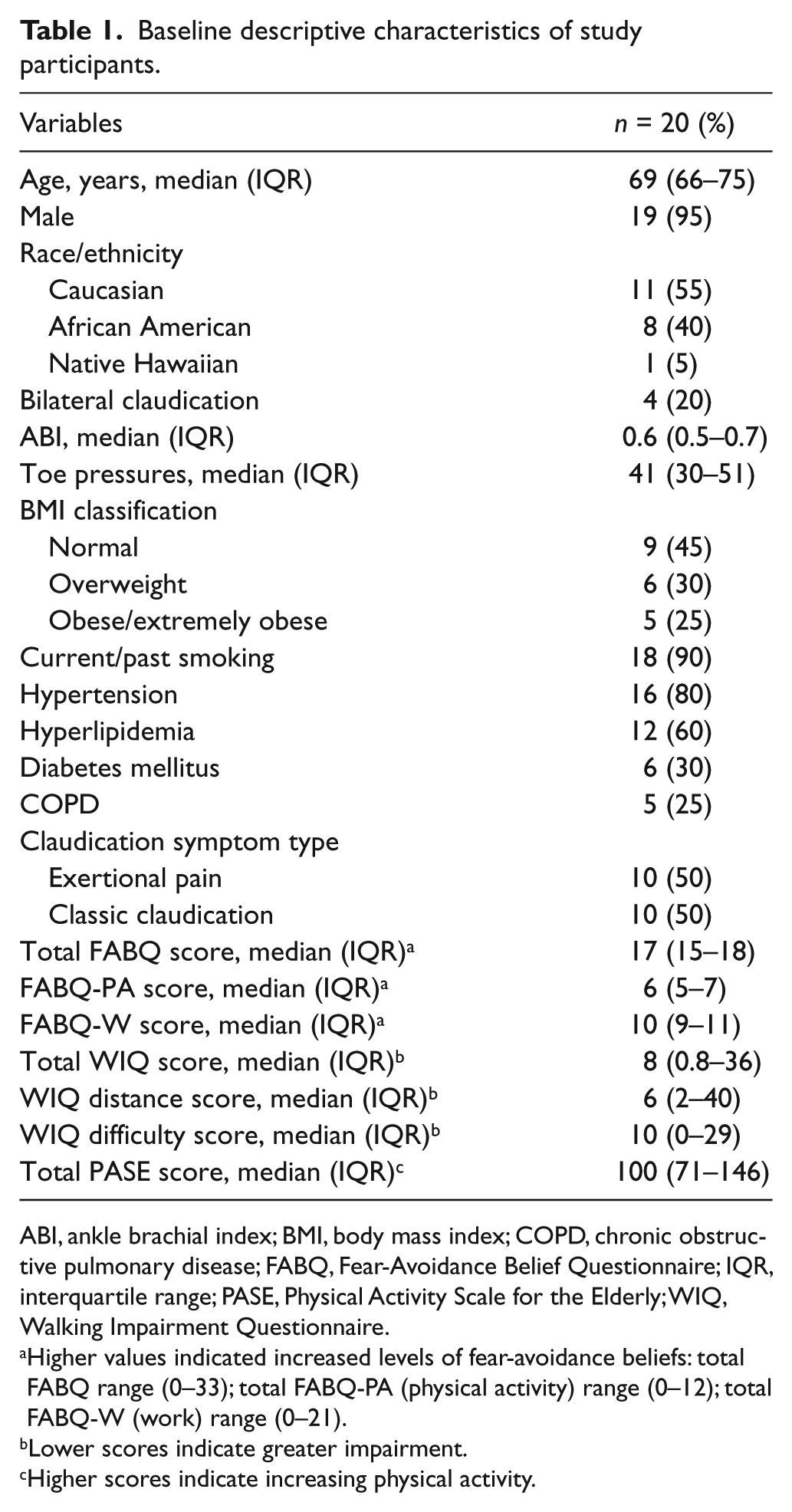
ABI, ankle brachial index; BMI, body mass index; COPD, chronic obstructive pulmonary disease; FABQ, Fear-Avoidance Belief Questionnaire; IQR, interquartile range; PASE, Physical Activity Scale for the Elderly; WIQ, Walking Impairment Questionnaire.
Higher values indicated increased levels of fear-avoidance beliefs: total FABQ range (0–33); total FABQ-PA (physical activity) range (0–12); total FABQ-W (work) range (0–21).
Lower scores indicate greater impairment.
Higher scores indicate increasing physical activity.
Fear-avoidance beliefs and perceptions
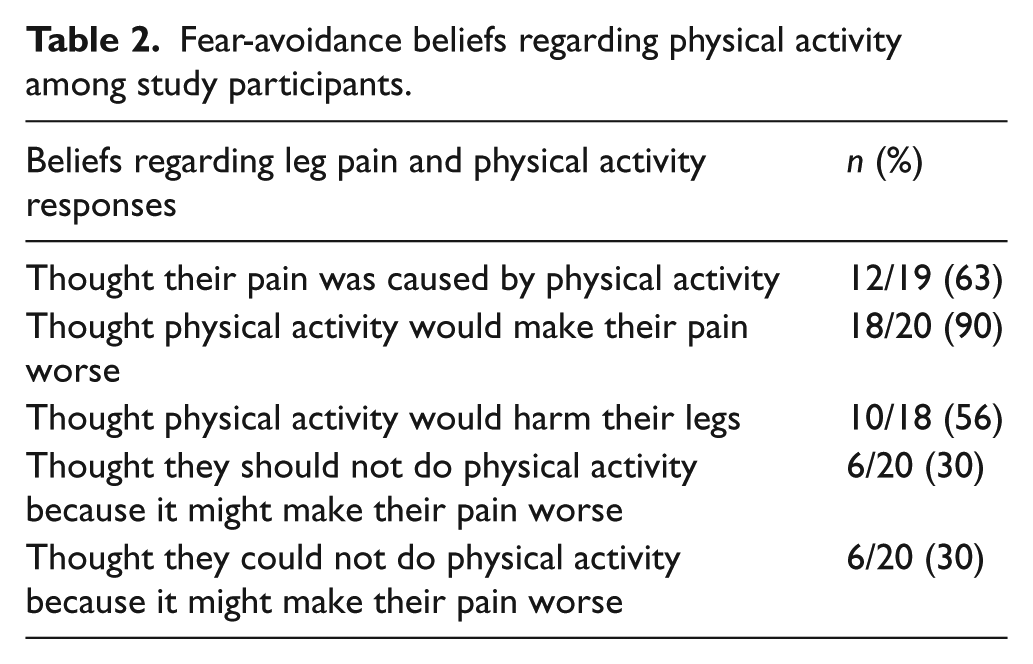
Higher values indicate a disposition to avoid behaviors (either at work or during physical activity) due to pain-related fear. The possible ranges of the scales in this study were: FAB, 0–33; FAB-PA, 0–12; FAB-W, 0–21. In our cohort, the median total FAB score was 17 with an IQR between 15 and 18. When considering specific questions in the instrument, 12 out of 19 participants (63%) believed that the primary etiology of their leg pain was walking and 10 (out of 20) participants (56%) believed that walking would harm their leg (Table 2). Among the 12 participants who stated that their pain was caused by walking, seven (58%) participants said that they should not walk because their pain might become worse. However, 14 (70%) participants did not think they should stop walking because their pain might become worse.
Fear-avoidance beliefs regarding physical activity among study participants.
Symptom improvement expectations and acceptable risks
We found a significant association between fear-avoidance beliefs (both total scores as well as the physical activity sub-scale) and expected benefit from exercise (p = 0.05, p = 0.01, respectively; unadjusted). In other words, people who had fewer fear-avoidance beliefs about walking harming their legs also expected greater benefit from walking. The association between increased expectation of benefit from walking and lower fear avoidance was still significant, when adjusted for physical activity (p = 0.01). Participants who expected greater improvement in their symptoms because of physical activity were also less likely to believe that they should not or could not attempt physical activity due to their leg symptoms (mean difference = −40.6, p = 0.02). In contrast, participants who stated that they thought that walking made their leg pain worse were more likely to expect greater benefit from surgical intervention rather than walking (mean difference = 47.5, p = 0.02). The varying levels of risk that participants were willing to accept, in exchange for symptom improvement, was not associated with fear-avoidance beliefs.
Physical activity
Total physical activity scores were not associated with total FAB scores or FAB-PA scores.
Type of claudication pain and symptom severity
As shown in Table 3, those who reported increased walking impairment were also more likely to report higher fear-avoidance beliefs (p = 0.001). When examining the difficulty and distance WIQ sub-scale scores separately, the same association was observed: as walking difficulty increased, fear-avoidance beliefs also increased (p = 0.001). Similarly, as the distance that a participant was able to walk decreased, fear-avoidance beliefs increased (p = 0.005). Increasing fear-avoidance beliefs, specifically regarding physical activity, were significantly associated with walking impairment (difficulty and distance). Type of claudication pain was not associated with fear-avoidance beliefs.
Factors associated with fear-avoidance beliefs in univariate models.
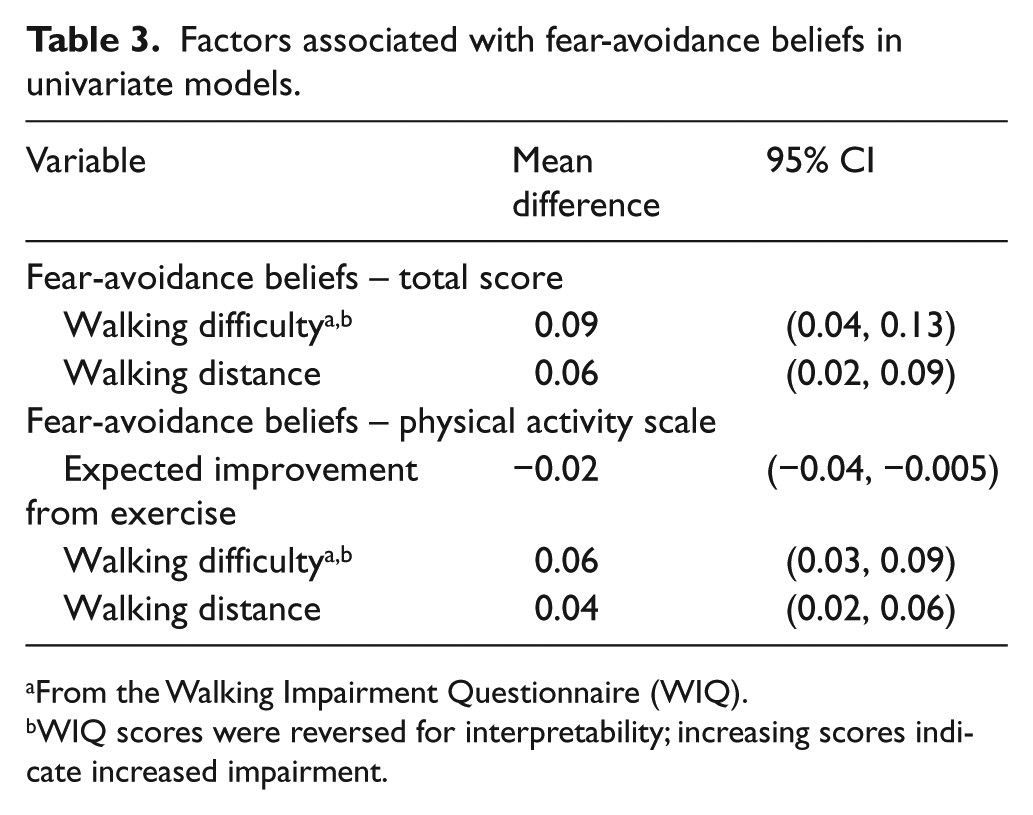
From the Walking Impairment Questionnaire (WIQ).
WIQ scores were reversed for interpretability; increasing scores indicate increased impairment.
Discussion
In this study, we examined how pain-related fears and beliefs were associated with patient expectations, self-reported symptom severity, type of claudication pain, and baseline physical activity. To our knowledge, this is the first study examining pain-related beliefs among patients with claudication. We found that: (1) a majority of the cohort was misinformed/confused about the relationship between claudication and walking; (2) those who expected greater benefit from physical activity did not avoid walking due to pain; and (3) fear-avoidance beliefs increased as self-reported symptom severity increased. We did not find a significant relationship between fear-avoidance beliefs and self-reported physical activity.
The significance of avoiding behavior because of pain-related fear has been underscored by the use of the FAM in the low-back pain and osteoarthritis literature.24–30 As patients with claudication present with muscular pain that is best served by physical activity, the implications of psychological factors in physical activity recommendations are highly relevant. The FAM postulates two pathways that lead to either physical disuse or overuse. 38 Physical disuse refers to the deliberate avoidance of pain-eliciting physical and social activities. This disuse leads to long-term physical deconditioning due to decreasing physical activity (disuse). 38 Psychologists have suggested that avoiding perceived ‘pain-causing’ behaviors is a frequent and pronounced response to pain. The first step that people usually take is avoiding physical activity and then, later, they begin to avoid social activities that could cause pain. Practically, in claudicants, unawareness of fear-avoidance beliefs could mean discounting a factor that, if addressed, could improve adherence to physical activity recommendations.
Specific questions in the FABQ measured patient’s beliefs regarding their understanding of claudication. At the beginning of the interview, the etiology of claudication was briefly described to the participants. All participants reported earlier knowledge of claudication, yet more than half of them stated that their pain was caused by walking. Strictly speaking, this is true; the act of walking does cause leg pain but the underlying etiology of claudication is atherosclerotic build-up that is unrelated to walking. Despite the fact that walking causes pain temporarily, it is also the source of symptom improvement. It appeared that individuals at the very least were confused by the etiology of claudication and were uncertain as to why it was being recommended as a source of relief. This uncertainty may contribute to physical inaction: 58% of those who thought their pain was caused by walking did not think they should walk for fear of exacerbating the pain. Galea et al.’s examination on the role of pain in walking behavior among claudicants adds some insight to our results. 39 The authors reported that perceived pain intensity did not have an independent effect on behavior or moderate the relationship between the intention to walk and behavior. We found similar results in our cohort – self-reported physical activity was not related to avoidance beliefs. However, we did see associations between FAB and symptom severity as well as benefit expectations. Galea and colleagues postulated that the lack of association between pain intensity and behavior might be explained by the distribution of pain (i.e. the lack of representation in the extremes). In the current study, the absence of an association between activity, symptom severity, and FAB might be due to a misrepresentation of walking behavior by our participants. Previous examinations have indicated that the correlation between direct and self-reported measures of physical activity is low to moderate. 40 In addition, approaches to understanding pain and its effect on walking behavior and walking intention differed between our studies. We directly measured symptom severity – a surrogate pain intensity measure as well as the participant’s beliefs regarding their pain and how it affected their walking; Galea et al. measured pain as an average intensity and used intentions to understand pain beliefs. Taken together, these studies highlight the effect that pain has on walking behavior and the importance of understanding how individuals with claudication understand, think, and relate to their leg pain.
Other pain-related findings from our study are in agreement with similar studies that examined illness beliefs and walking behavior among claudicants.41,42 Study participants in Scotland, reported a fear of walking while others did not understand the source of their pain and the effect that exercise or walking would have on their symptoms. 41 Galea et al. noted that pain-related factors figured prominently in their examination of barriers and facilitators of walking among claudicants. 42 When describing their walking, individuals highlighted the necessity to account for psychological and environmental factors specifically related to their pain – namely, implementing coping strategies to push through the pain and the necessity for resting places when walking for activity. 42 Some individuals questioned whether walking through pain was wise – thus, emphasizing the necessity for specific guidelines and clear directions on what to expect while walking with claudication. 43 Importantly, Cunningham et al. highlighted the lack of understanding regarding the long-term effects of PAD and claudication. 41 Our participants, too, did not consider greatly the long-term impact of PAD and most were interested in acute relief.
This study was unique, in that participants were apprised of the potential long-term risk of amputation and even asked about their preferences for treatment based on amputation risk. We found that a majority of people (72%) were willing to accept some risk of amputation in exchange for any symptom improvement. In light of this apparent urgency for recovery and the possibility that fear of pain acts as a deterrent for walking, it is essential to gauge the patient’s understanding of their symptom’s sources and how their treatment options (including the underlying mechanisms) will benefit them, both in the short and long term.
Fear-avoidance beliefs were also associated with benefit expectations. Participants who expected greater benefit from activity did not report avoidance behaviors but this association did not affect walking behavior as measured by the PASE. There could be other factors, unaccounted for in our study, in the pathway between fear avoidance, expectations, and behavior that mediate this relationship. Yet, it is still illuminating that fear of pain seems to act as a deterrent for walking. Although this is intuitive, few studies have described this association among claudicants. By showing the potential relationship between these factors, we hope to influence daily clinical practice by emphasizing to patients that foundationally there is a non-causal relationship between walking and pain. It also bears mentioning that as symptom severity increased, fear-avoidance beliefs also increased – showing, perhaps, that the fear of pain because of walking increases as discomfort or unease increases.
Appreciating the psychological effects of pain on treatment recommendations would bolster physical activity interventional research in claudication – increasing adherence rates and overall quality of life. If we were to interpret our findings in the context of the transtheoretical model, a majority of the participants in our study (58% thought they should not walk because of their leg pain) are in the pre-contemplation stage. 44 Future studies should focus on ideas to mobilize these people into the next stages of contemplation, preparation, and action. The first step might be to manage the patient’s expectations by describing in detail the relationship between claudication and the benefits of walking. Our study explored the possible association between fear-avoidance beliefs and walking in a small cohort of claudicants. We cannot clearly comment on the causal relationship of these two factors, but their importance should not be diminished and should be explored in the future utilizing robust study designs. By definition, the FAM suggests that individuals tend to avoid behaviors that cause pain due to an expectation that the pain is an indication of harm or simply to avoid the discomfort of pain. In this study, our goal was to examine whether fear avoidance existed among claudicants, and we showed that there were some interesting relationships between positive benefit expectations and fear avoidance – something that is perhaps a little less evident from the FAM.
Strengths and limitations
Most of the analyses conducted in this study were univariable. Owing to the size of our sample, we were unable to account for factors that might confound associations – therefore threatening the internal validity of the study. Because our cohort was primarily male, we were unable to measure these perceptions and beliefs among women. Another source of bias, unmeasured in this study, is the effect of a vascular surgery referral on the patient’s treatment expectations. It is possible that a referral to a surgical clinic comes with an inherent expectation of surgical treatment. To address this bias, future studies should restrict inclusion of study participants to those who have not yet been referred to a specialty clinic for further care. Lastly, the measure used to describe physical activity is self-reported and there is a possibility that participants over-reported their levels of activity. 40 Despite this, some factors that strengthen our study include: (1) identification of alternative deterrents to physical activity among Veterans – a unique population in terms of significant comorbidities and psychological factors; (2) measure of baseline physical activity among these participants to determine effects of perceptions on behaviors; and (3) assessment of how risk and benefit perceptions are related to the factors described previously.
Conclusions
We assessed how fear of pain affected walking among a group of people with claudication. A large proportion of participants believed that their pain was caused by walking, but those who did not avoid walking specifically because of pain also expected more benefit from walking. On the other hand, those who believed that surgery was more effective thought that walking worsened their symptoms. We found that as symptom severity increased, the likelihood of avoiding walking also increased. Because pain has psychological implications, understanding patient beliefs in the context of pain would highlight factors that could strengthen the way physical activity recommendations are delivered. Discounting the influence of these perceptions and beliefs could mean overlooking factors that, if addressed, could encourage physical activity and decrease adherence failure.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.