
Abstract
The prevalence of pulmonary embolism (PE), PE mortality and treatment-associated costs for the years 2000 to 2006 were analysed using a statutory health insurance sample of AOK Hesse/KV Hesse, which contained information for an 18.75% random sample of 1.9 million persons insured with the AOK Hesse. Within the sample a PE diagnosis was accepted as valid if it was documented as the main discharge diagnosis or as an additional hospital diagnosis during hospitalization and if at least one of the following criteria was met: prescription of oral anticoagulants or heparins, PE documented for at least two quarterly periods or documented in only one quarter for patients who died within 28 days after hospital discharge. The economic burden from the perspective of the insurance fund was assessed by an analysis of resource consumption (direct costs) and by a matched pair analysis with controls without PE to estimate excess costs. A 99% winsorization of each cost category was performed to control for extreme outlying values. The prevalence of PE as the main discharge diagnosis and an additional hospital diagnosis varied from 55.3 to 71.7 per 100,000 insurants in the years 2000 to 2006. Insurants aged 80 years and more had a prevalence of 406.9 per 100,000 (year 2006). From 2001 to 2003 the in-hospital mortality rate ranged from 20.4% to 24.9% and decreased to 14% in 2006. A total of 85% of all patients with PE who survived the first year had at least one prescription of vitamin K antagonists. For patients who survived the first year, treatment costs exceeded € 20,000, with an estimation of additional costs of € 5816 for men and € 8962 for women in the matched-pair analysis. Owing to high in-hospital costs, the overall cost of treatment was highest for patients younger than 60 years. In conclusion, the prevalence rate of PE in Germany is comparable to international data. Treatment costs within the first year after hospital discharge are high, and there is a need to clarify the settings associated with PE in Germany with its high rate of prophylaxis.
Introduction
Because venous thromboembolism (VTE) is associated with substantial morbidity and mortality, great efforts have been undertaken to prevent this disease, especially pulmonary embolism (PE), in patients at risk.1–5 Few studies, however, report a general reduction in PE incidence or mortality.3,6 Silverstein et al. describe how PE incidence decreased between 1966 and 1990, although the incidence of deep vein thrombosis (DVT) remained unchanged in men and even increased in older women. 5 Data from studies examining the incidence of fatal PE in selected patient groups are contradictory, some showing a decrease in mortality from PE 7 while others show no noticeable changes. 8 According to the National Center for Health Statistics (Multiple-Cause Mortality Files compiled from death certificate data), the age-adjusted PE death rates decreased from 191 per million in 1979 to 94 per million in 1998, with a 56% decrease in men and a 46% decrease in women. 9 Different reasons are discussed. A decline in population-based PE mortality rates between 1979 and 1989 may be due to a decreased incidence of PE reflecting improvements in prophylaxis, whereas the continuing decline through 1998 may reflect decreased case fatality rates due to earlier detection and better management. 10
When we analysed WHO mortality data (from 1980 to 2004) for rates of death due to PE, we found that, while in most countries PE mortality decreased over time, there was a slight but continuous increase in Germany. 11 This increase in PE mortality is contrary to all expectations, especially since the ENDORSE-study showed that Germany is one of the countries with the highest rates of appropriate prophylaxis in hospitalized patients at risk for VTE. 12 The prevalence and incidence of PE in Germany have never been analysed in population-based studies. However, routine health-care data provide detailed information about PE prevalence, mortality, treatment and associated costs. According to diagnosis-related groups’ (DRG) data reported between 2005 and 2007, a total of 67,351, 69,234 and 71,223 PEs (ICD-10-GM: I26) were documented as the main or secondary diagnosis in German hospitals, respectively. 13 Since these data do not provide much detail, we used a statutory health insurance (SHI) sample of data gathered by the AOK Hesse/KV Hesse covering the years from 2000 to 2006.
Patients and methods
This study is based on routine health-care data collected by the local statutory health insurance fund (AOK) and the Association of Statutory Health Insurance Physicians (KV) of the Federal State of Hesse in Germany. The AOK is a statutory health insurance fund that covers approximately 37% of all members of the statutory health insurance system in Germany; this corresponds to slightly less than a third of the German population (82 million). It consists of 14 regional funds, one of which covers the federal state of Hesse situated in west-central Germany (6 million inhabitants). Our database – the SHI sample AOK Hesse/KV Hesse – covers an 18.75% random sample of all persons insured by the AOK Hesse between 2000 and 2006, 14 with insurance being defined as being continuously insured in the respective year or, in case of death, having been continuously insured for at least three quarters before the quarter in which the death occurred. We generated patient-related treatment histories by record linkage for each insured individual, including both outpatient and inpatient treatment. The database also included information on patients’ age, sex and period of insurance coverage as well as data relating to the use and cost of medical services (outpatient care, inpatient care, prescriptions, medical devices, and additional nursing care insurance). All regulations regarding data privacy were adhered to.
Both the main discharge diagnosis and additional hospital diagnosis were coded according to the German version of the ICD-10. We used the ICD-10 code I26 to assess PE as a hospital diagnosis. For further validation of PE diagnoses, at least one of the following criteria was additionally required: prescription of oral anticoagulants or heparins, outpatient diagnosis of PE documented for at least two quarterly periods in the respective year or documented in only one quarter for patients who died within 28 days after hospital discharge.15,16 Based on these validation criteria, PE prevalence rates were estimated for the years 2000 to 2006 as the percentage of insurants for whom at least one PE was documented. In 2000 and 2006, data for 326,672 and 286,286 insurants were available, respectively. Mortality was calculated as inpatient mortality and as 28-day, 90-day and 180-day mortality with the date of hospital admission as the index date.
The economic burden associated with PE was estimated from direct costs reimbursed by the AOK and nursing care insurance and from excess costs. Direct costs were estimated only for patients who survived the first year after PE diagnosis in 2006 (n = 176). Excess costs were estimated by a matched-pair analysis of cost differences between a patient with documented PE and a control with a hospital stay but without documentation of PE, matched for sex and age. This approach has been successfully applied to different diseases.17,18 Costs incurred are presented for the subcategories outpatient physician services, outpatient prescriptions, inpatient care, other services (medical devices, transport) and nursing care. All costs are specified in Euros.
Statistics
Age- and sex-adjusted prevalence rates and mortality rates were calculated for the years 2000 to 2006 with the German population of the respective year as the reference population.
For all validated PEs in 2006, treatment was described and treatment costs were estimated. In an additional sensitivity analysis we did a 99% winsorizing, a strategy to reduce the effect of outliers. The costs of the upper 1% of cases and controls were set equal to the value corresponding to the 99th percentile. This transformation of the statistic was done for each cost category for cases and controls.
Analyses were performed using SAS for Windows version 9.2 (SAS Institute Inc., Cary, NC, USA) and MS Excel 2007. The database software used was MS-SQL-Server 2008 for Windows Server 2003.
Results
Estimation of prevalence
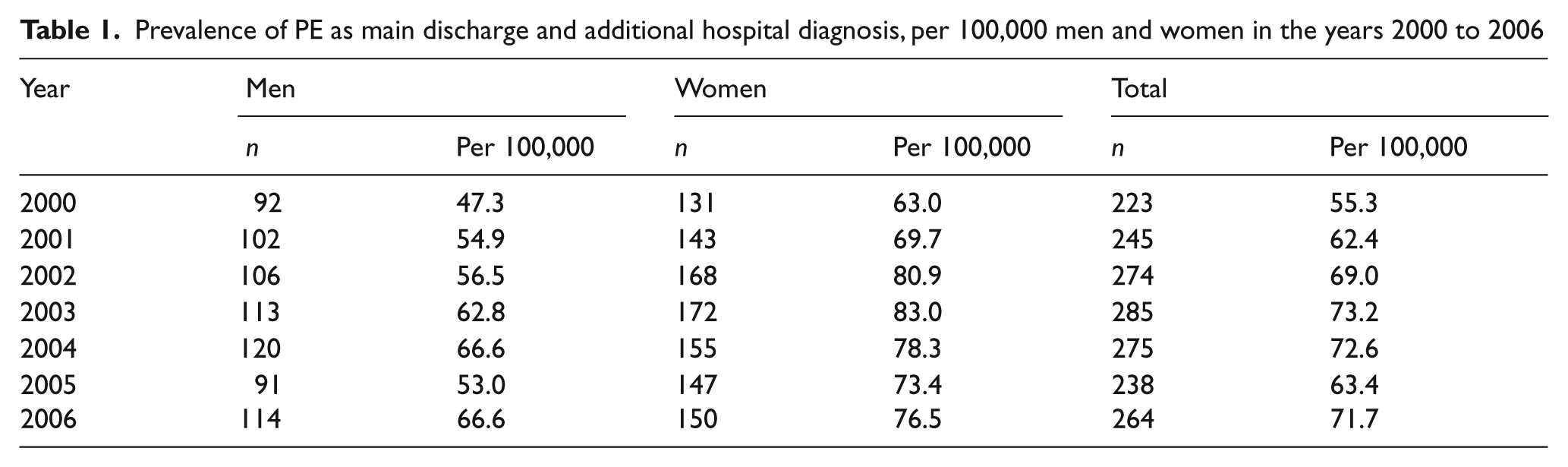
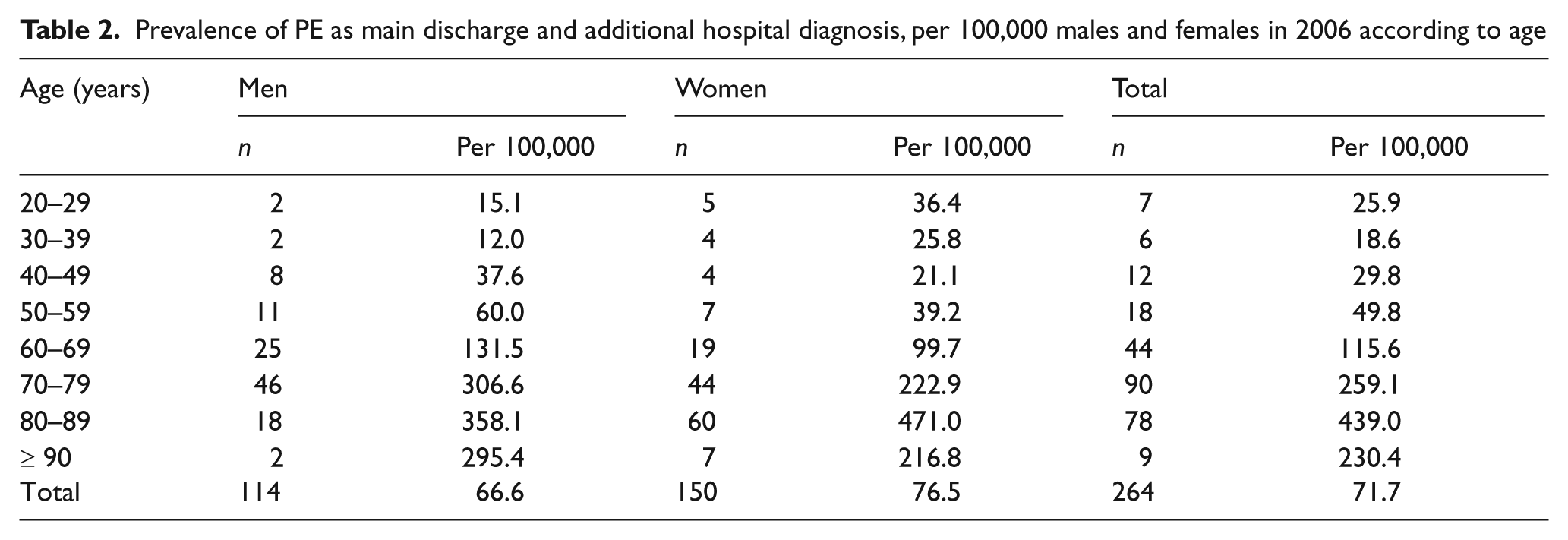
The estimated prevalence of PE (as the main discharge diagnosis or the additional hospital diagnosis) increased from 55.3 per 100,000 insurants in 2000 to 71.7 in 2006 (Table 1). PE was more frequent as the main discharge diagnosis than as the additional hospital diagnosis, with the rates increasing to 46.8 per 100,000 insurants in 2006 for the main discharge diagnosis and 24.8 for the additional hospital diagnosis. Women were more frequently affected than men. Prevalence increased with increasing age. Among insurants between 80 and 89 years of age the prevalence was 439.0 per 100,000 in 2006, whereas among the youngest age group (20–29 years) it was 25.9 per 100,000 (Table 2).
Prevalence of PE as main discharge and additional hospital diagnosis, per 100,000 men and women in the years 2000 to 2006
Prevalence of PE as main discharge and additional hospital diagnosis, per 100,000 males and females in 2006 according to age
Estimation of mortality
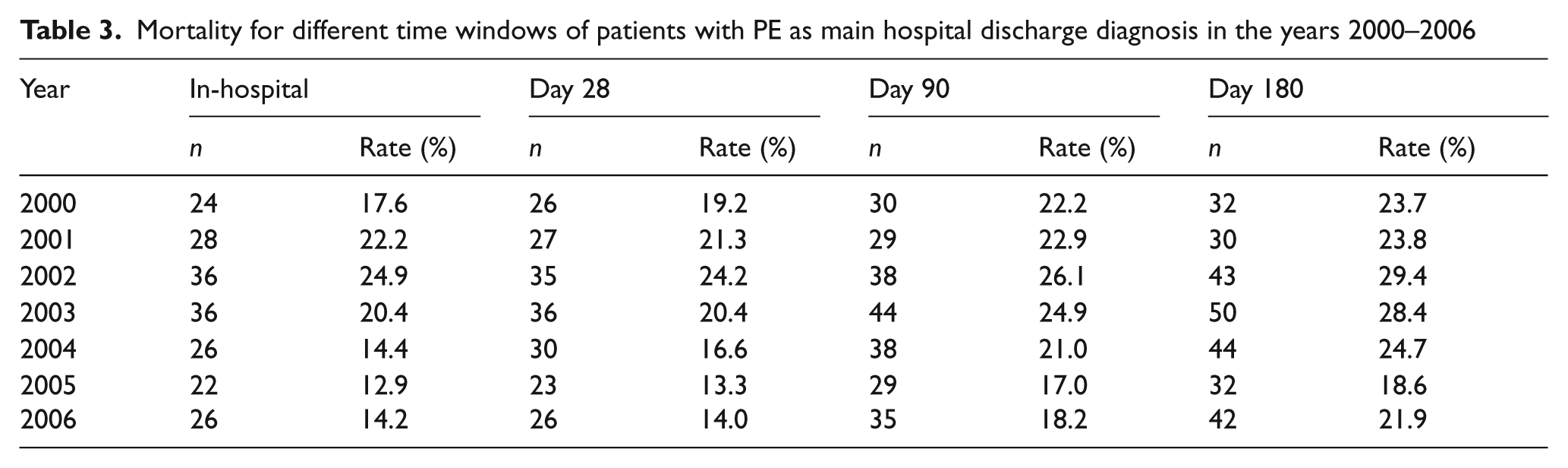
For patients with PE as the main discharge diagnosis, mortality rates did not show a decreasing trend within the period from 2000 to 2006 (Table 3). Most deaths occurred within the first month after hospital discharge (2006: 28 days, 14.0%; 180 days, 21.9%). The difference in mortality rate between men and women was small, but women tend to have slightly higher mortality rates in all years and for all analysed post-discharge times (2006: 180-day mortality, women: 23.0%; men: 20.4%).
Mortality for different time windows of patients with PE as main hospital discharge diagnosis in the years 2000–2006
Treatment after discharge
In 2006, 85.2% of all patients who survived the first year after hospital discharge (n = 176) had at least one prescription for vitamin K antagonists (VKA) and 42.6% received heparin, usually low molecular weight heparins (LMWH) (40.9%). The most commonly prescribed heparin preparations were enoxaparin (25.0%), certoparin (11.4%) and nadroparin (8.5%). The treatment duration differed significantly between the two pharmacological subgroups: patients with VKA received the drug for a mean duration of two-thirds of the observation time, while the mean percentage duration for heparin was 28%. A subgroup of 38 patients showed changes in anticoagulation treatment after hospital discharge: n = 9 (23.7%) changed back from VKA to heparin; n = 6 (15.8%) were on heparin, changed to VKA with a certain delay and then back to heparin; and n = 23 (60.5%) were on VKA, changed to heparin and then back to VKA. Fifteen (28.3%) remained on VKA therapy. Compression stockings were prescribed for 45.5% of women and 36.0% of men who did not die in the first year after hospitalization.
Those with additional hospital stays within the year after discharge were 58.7% of men and 65.3% of women. The mean number of additional hospital stays was 1.6 for men and 2.0 for women, with a total length of stay of 21.4 days and 23.6 days, respectively.
Estimation of costs
For men and women who survived the first year after PE, per capita treatment costs exceeded € 20,000 (Table 4). Men suffering from PE incurred additional costs of € 5816 compared to matched controls, and for women with PE the additional costs amounted to € 8960. Drug costs were 2.1 times higher than in matched controls, with a ratio of 1.7 for nursing care and 1.6 for in-hospital treatment. The relation between cost subcategories is different between men and women. Men had higher costs for in-hospital treatment but lower costs for nursing care after discharge. However, after winsorization the differences between men and women regarding in-hospital treatment disappeared.
Accumulating treatment costs and excess costs of a PE patient surviving 1 year, by sex
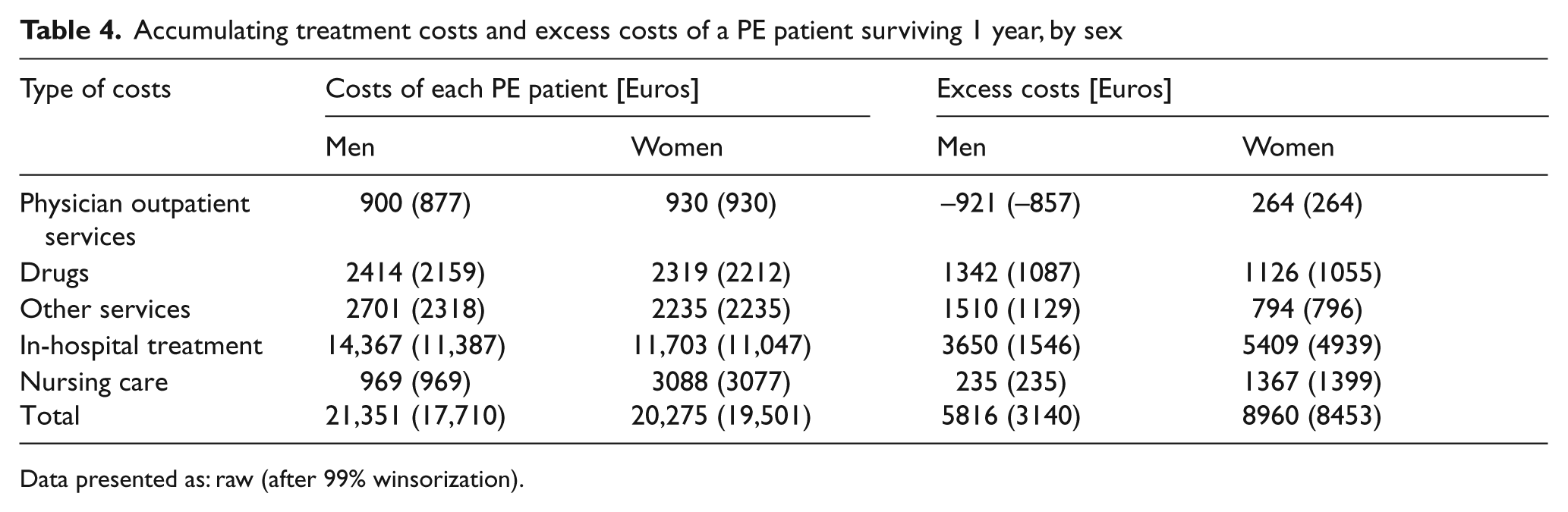
Data presented as: raw (after 99% winsorization).
Treatment costs tend to be higher in younger age groups. Patients younger than 60 years show the highest costs, especially due to high in-hospital treatment costs (Table 5). After winsorization the estimate for in-hospital costs in the youngest age group decreased to € 11,861 and treatment costs were highest for patients above 70 years of age.
Accumulating treatment costs and excess costs of a PE patient surviving 1 year, by age
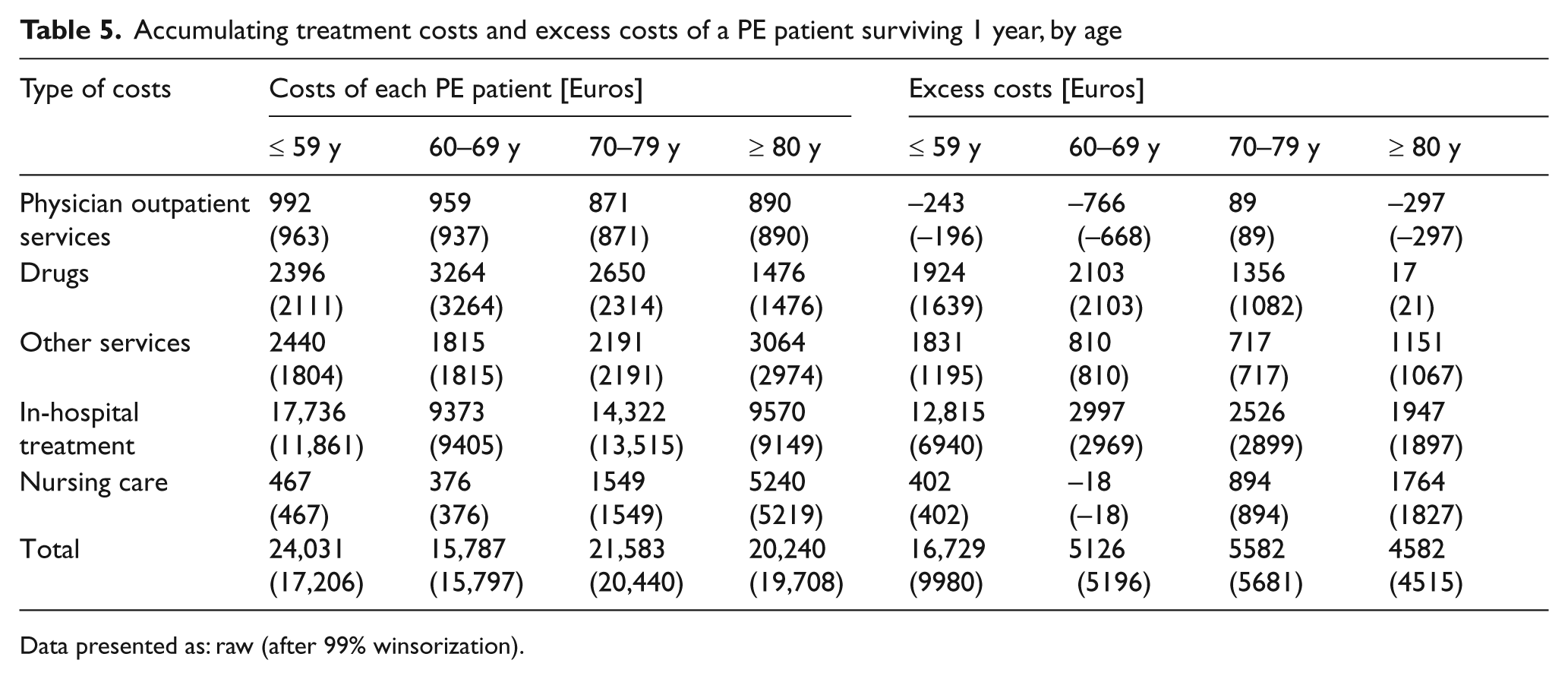
Data presented as: raw (after 99% winsorization).
Discussion
The data presented here are derived from the statutory health insurance sample AOK Hesse/KV Hesse and for the first time give detailed information on PE prevalence and mortality in Germany for the years 2000 to 2006. They also provide relevant information on specific outpatient treatment and associated costs.
Data from numerous robust clinical trials have demonstrated that with appropriate prophylaxis many venous thromboembolic events can be prevented in both surgical and medical patients.1,12,19 Even though the strong evidence supporting VTE prophylaxis spans several decades, a number of large American and global registries have documented very poor use of appropriate thromboprophylactic measures. In contrast, the multinational cross-sectional ENDORSE study showed that pharmaceutical prophylaxis was correctly implemented for both surgical and medical patients in Germany. 12
With a PE prevalence of 55.3 in 2000 per 100,000 insurants rising to 73.2 in 2003, our figures match the data from the EPI-GETBP Study Group published in 2000, which reported pulmonary incidences of 52 to 69 per 100,000 inhabitants. 20 Thus, despite an established use of pharmaceutical prophylaxis in hospitalised patients in Germany, no reduction in PE prevalence could be seen. The reasons remain unclear, but it can be supposed that a number of PEs occur outside medical settings where they are not as well documented. Our data are also in accordance with a study by Park et al. 21 who analysed discharge data from US acute care hospitals taken from the Nationwide Inpatient Sample during the 8-year period between 1998 and 2005. During this time the number of patients discharged with primary or secondary PE increased from 126,546 to 229,637, while hospital case fatality rates for these patients decreased from 12.3% to 8.2% (p < 0.001), the length of hospital stay decreased from 9.4 days to 8.6 days (p < 0.001) and total hospital charges increased from $25,293 to $43,740 (p < 0.001). 21 Better diagnostic techniques may account for increased PE rates in recent years. Within the New York State’s (NYS) Statewide Planning and Research Cooperative System (SPARCS) the use of CT scans in patients with suspected PE increased, leading to an increase in PE diagnoses between 1994 and 2004 but showing no corresponding decline in mortality. 22 Further evidence with more detailed data from individual patients is needed to differentiate the role of better diagnostic techniques and the true changes in PE rates over the years.
Whereas in men the prevalence of PE increases stepwise with age, there is a dramatic increase for women between the 7th and 8th decades of life, with almost two-thirds of all PEs in women occurring within the 8th and 9th decades of life. 13 This high increase of PE in older women might be an effect of differences in the diagnostic process, but data from the National Hospital Discharge Survey analysed by Stein et al. 23 do not support a sex bias in the diagnosis of PE or DVT, the use of diagnostic tests or the duration of hospitalization for PE or DVT. The increase in PE might be compared to the high increase in postmenopausal incidence of coronary heart disease (CHD), which is assumed to be associated with a decrease in the protective effect of female hormones. However, the discussion of such an effect for PE is difficult since hormone replacement therapy usually increases the risk of VTE in women. 24
In a multicentre PE registry in Germany, the overall hospital mortality rate ranged from 8.1% in the group of stable patients to 25% in those presenting with cardiogenic shock and 65% in patients needing cardiopulmonary resuscitation. 25 Since the prognosis for most patients who are referred to hospital with a PE diagnosis and reach the hospital alive is rather good, we were surprised to see that in our data a high rate of death is associated with PE as a main diagnosis. In the RIETE registry, the all-cause mortality rate for 8053 PE patients included between 2001 and 2003 was 4.1%. 26 Within the same time period death rates of 12% were reported in the administrative database from the Spanish Ministry of Health, which covers 87,733 PE patients from 256 public hospitals. These rates are more comparable to our own data. 26 From 2001 to 2003 in-hospital mortality rates seen in our data ranged from 20.4% to 24.9% and decreased to 14.0% in 2006.
Data on anticoagulation treatment and wearing of compression stockings after hospital discharge are not available in the literature. A VKA treatment rate of 85% seems to be reasonable as select patients may remain on long-term LMWH. Since health insurance pays for LMWH in Germany, the threshold to prescribe LMWH instead of VKA is rather low. Bridging with LMWH was necessary in a relevant number of patients. The prescription rate for compression stockings appears to be low (45.5% of women and 36.0% of men).
Treatment costs in the first year after discharge for surviving patients exceeded € 20,000, with additional costs incurred by PE being estimated at € 5816 for men and € 8960 for women. Owing to differences in national health systems the comparison of studies is difficult.27–30 Nutescu et al. 27 reported US data showing that after controlling for potential confounders, DVT following major orthopeadic surgery was associated with a 22% and 74% increase in the average number of expected outpatient and emergency department visits, respectively, during the 6-month post-discharge period. Dobesh 29 reported treatment costs for PE in the US with the costs of managing an initial episode of PE ranging from $9566 to $16,644. Although much of the costs incurred by VTE are associated with managing the acute event, the costs associated with its long-term complications such as recurrent VTE, post-thrombotic syndrome and pulmonary hypertension are also significant. Spyropoulos and Lin 28 published a retrospective analysis using the US Integrated Health Care Information Services (IHCIS) National Managed Care Database, analyzing the period from February 1998 to June 2004. For the cost analyses, they included patients who had been enrolled in a health-care plan for a minimum of 30 days prior to and 365 days following the DVT or PE hospitalization. For a primary diagnosis, the average total annual costs (total annual provider payments made by a health plan) were $10,804 for DVT and $16,644 for PE. For secondary diagnoses, the average was $7594 for DVT and $13,018 for PE. All these studies describe DVT- and PE-associated costs. As we also saw in our study, treatment costs within the first year are high and prevention of each single PE is therefore desirable.
Strengths and limitations
For the first time, data on PE prevalence and mortality are presented for a German state, covering the years 2000 to 2006. Our retrospective cross-sectional study is based on comprehensive medical routine data gathered for insurance purposes without preselection or recall bias. The database is suitable for epidemiologic research as well as research on health care and health economics.
Although routine data are frequently used for secondary purposes, there is currently no systematic analysis of coding quality in Germany.15,16,31 Whether coding matches reality (a prerequisite for using routine data for health politics) has to be investigated in special trials. Since we cannot estimate the rate of inadequate coding for PE, we recommend further health economic studies to quantify this effect. We applied a strong case definition with additional criteria used to verify the ICD-10 code to minimize flaws caused by imperfect coding practice.
Our database covers one region and one health insurance fund. Patients insured with the AOK in Hesse may not be representative of the German population in general. The individuals insured with this particular insurance fund were historically known to have a socio-economic status slightly below average, which might have an impact on PE prevalence and health-care utilization as analyzed here. Nowadays, however, only very minor differences exist in the health services covered by the different German statutory health insurance funds. Differences are likely to exist between statutory and private insurance (< 10%), although treatment of PE would be similar. 32 It seems rather unlikely, though, that patients insured by statutory health insurance would be treated any differently depending on their health insurer. In comparison with other studies our data show good comparability, favouring the assumption of a certain amount of reliability for these data.
The cost analyses cover only costs reimbursed by the health insurance fund. The actual costs both for the patients affected and for society as a whole are of course higher.
In comparing our data with those from other studies both differences in study populations and uncertainties regarding the validity of a PE diagnosis should be considered. In our study, as in the study of Park et al., 21 the validation of PE diagnosis by objective tests such as imaging was not required since the results of diagnostic procedures are not available in the database. Since our study is based on hospital diagnoses, we are confident that misclassification of documented cases is low but we cannot rule out that some cases might have been overlooked.
Although the statutory health insurance sample AOK Hesse/KV Hesse is a reliable database with regard to the total number of PEs, it does not give any information about the individual settings of PEs and their preventability. As other studies show, more VTEs were diagnosed in the 3 months following hospitalization than during hospitalization. 33 The development of more effective strategies in primary, secondary and tertiary prevention of PE should therefore rely on analyses not only of case management during hospitalization, but also of the pre- and post-hospital period.
In conclusion, the prevalence rate of PE in Germany is comparable to international data but the in-hospital mortality rate remains high. Treatment costs within the first year are high and there is a general need to reduce PE rates, but an intensification of pharmaceutical prophylaxis for hospitalized patients, which is already quite high in Germany, will not achieve this goal. Efforts to improve in-hospital use of VTE prophylaxis may help to decrease the incidence of outpatient VTE. However, given the shortening of hospital stays, studies of extended VTE prophylaxis after hospital discharge are warranted, 33 and there is a need to clarify the settings associated with PE in Germany.
Footnotes
Acknowledgements
The authors thank the ‘AOK – Die Gesundheitskasse in Hesse’, and the Association of Statutory Health Insurance Physicians of Hesse for provision of the data for the SHI sample AOK Hesse/KV Hesse.
Funding
The analysis was funded by Sanofi-Aventis Germany GmbH.
Conflict of interest
K Kröger, Ch Moerchel and Th Moysidis have done studies for Sanofi-Aventis and act as speakers. The PMV Research Group (J Küpper-Nybelen and I Schubert) has received unrestricted research grants from the Ministry of Health, Ministry of Education and Research, sickness funds, private foundations and drug companies. C Kienitz is an employee of Sanofi-Aventis Germany, a company active in marketing LMWH.