
Abstract
A 23-year-old male presented from a nursing home with hypotension, tachycardia, diaphoresis and electrocardiographic evidence of right ventricular strain that was confirmed by echocardiography. His differential diagnosis included sepsis and pulmonary embolism. A high-resolution computed tomography scan demonstrated no pulmonary emboli but did demonstrate multiple bilateral pulmonary nodules. Upon questioning he admitted to injecting a long-acting narcotic that had been manually macerated, dissolved in saline, and injected through an indwelling intravenous line. Lung biopsy findings were consistent with cellulose-induced perivascular granulomatosis. Cellulose granulomatosis can be seen in patients who inject medications designed for oral use and should be considered in patients who present with acute pulmonary hypertension.
Introduction
Foreign body granulomatosis has been described in intravenous (IV) drug abusers who inject medications designed for oral use.1–7 Oral medications such as pentazocine, codeine, hydrocodone, and temazepam contain insoluble fillers such as talc, cellulose, and starch. These fillers are designed to bind tablet particles together as well as prevent the tablet from sticking to machinery during the manufacturing process.1–3 Oxymorphone hydrochloride is a film-coated extended-release tablet that contains silicified microcrystalline cellulose. 8 Microcrystalline cellulose when crushed and injected forms long rod-like crystals in pulmonary arteries and causes granuloma formation.2,4
Case report
A 23-year-old male presented with hypotension, tachycardia, and diaphoresis. The patient’s past medical history was significant for a motor vehicle accident the previous year that resulted in multiple fractures including a left hip and femur fracture. The patient had multiple surgeries and hardware placements in order to repair his injuries. At the time of presentation the patient was residing in a nursing home for rehabilitation following the accident and IV antibiotics were being administered through a central line. On physical examination, he was alert conscious and oriented to person, place and time. Blood pressure was 70/40 mmHg, pulse 104 beats per minute and temperature 98.7°F. The jugular veins were not visible and cardiac examination had accentuated a second heart sound with right ventricular heave. The lungs had clear bilateral air entry with no rales. The left lower extremity had a large wound with mild erythema surrounding the wound with no evidence of purulent discharge. There was a high white blood cell count with elevated D-dimer on blood work. The chest X-ray showed no acute cardiopulmonary process. An electrocardiogram (ECG) demonstrated inverted T waves in leads V1–V6 and lead III and the appearance of an S1, Q3, T3 pattern consistent with right ventricular strain (Figure 1).
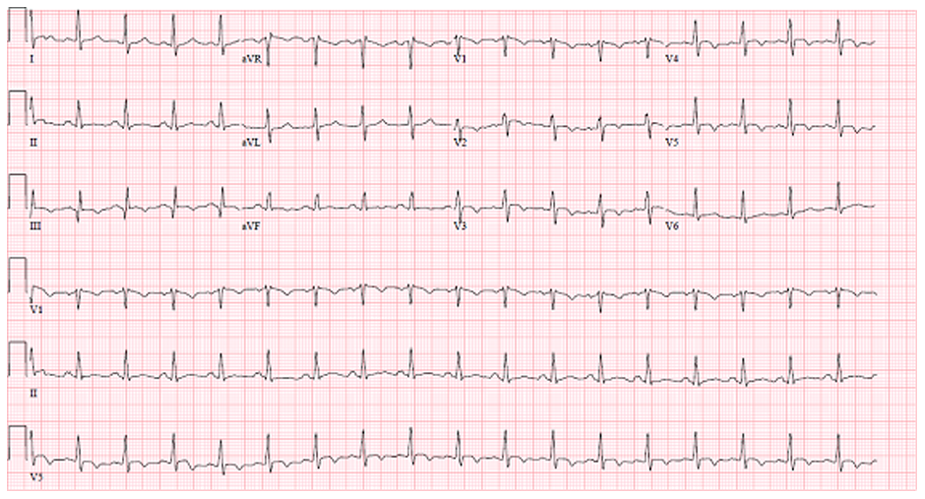
A 12-lead electrocardiogram demonstrating the S1, Q3, T3 pattern with non-specific T wave changes consistent with acute right ventricular strain and consistent with pulmonary embolization.
The patient was admitted with the working diagnosis of pulmonary embolism and sepsis. An echocardiogram, ordered for suspected pulmonary embolism, demonstrated that the right ventricle was severely enlarged with reduced systolic function (Figure 2) and evidence of pressure and volume overload with absence of McConnell’s sign. However, a ventilation perfusion (VQ) scan revealed a low probability of a pulmonary embolism. A subsequent echocardiogram and right heart catheterization demonstrated no evidence of significant intracardiac shunting but there was persistent elevation of right heart pressures.
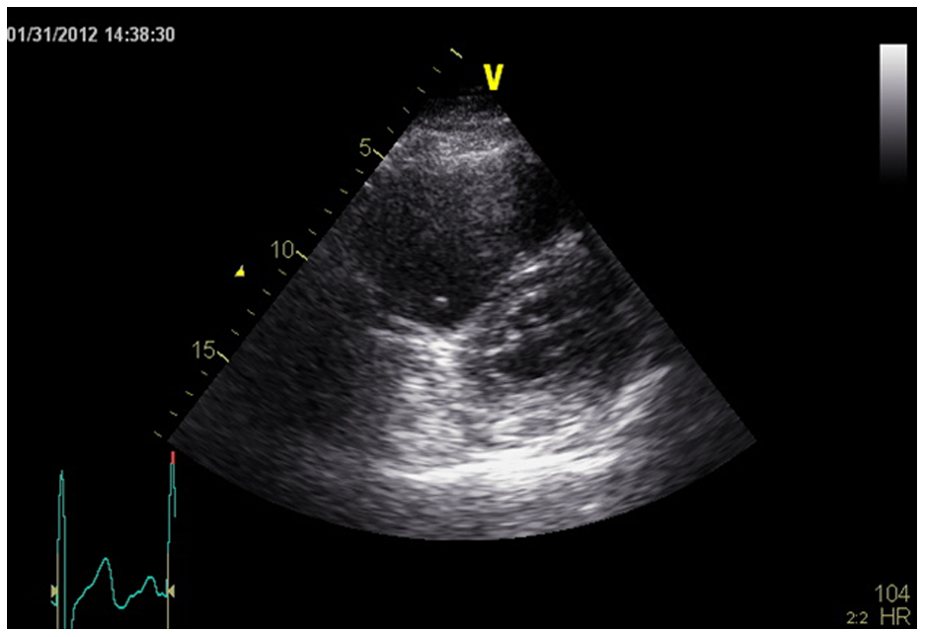
Echocardiogram performed in the parasternal short access view demonstrating right ventricular enlargement and displacement of the interventricular septum in a pattern consistent with right ventricular pressure overload.
After resolution of acute renal insufficiency, which was likely related to hypotension, a high-resolution chest computed tomography (CT) scan demonstrated no evidence of pulmonary embolism; however, bilateral small pulmonary nodules were apparent. One nodule was located in the right middle lobe measuring 0.3 cm in diameter, and another in the right lower lobe. A sub-pleural nodule was located in the left upper lobe near the apex measuring 0.4 cm and another located in the left lower lobe measuring 0.2 cm. All of the nodules had the characteristic of haloing. The patient’s mother mentioned that she saw her son injecting a substance through his IV line and upon further questioning him, he admitted to crushing extended-release oxymorphone (Opana™; Endo Pharmaceuticals, Chadds Ford, PA, USA) and injecting it into his central IV line.
To confirm the diagnosis the patient underwent a bronchoscopy with biopsy that revealed intravascular birefringent material, consistent with cellulose, associated with perivascular granulomas (Figures 3 and 4). CD34 immunostain confirmed the presence of foreign material within the vasculature. Overall, the histomorphology was consistent with intravascular deposition of cellulose fibers with a perivascular foreign body reaction and granuloma formation due to illicit administration of a long-acting oral narcotic administered intravenously.
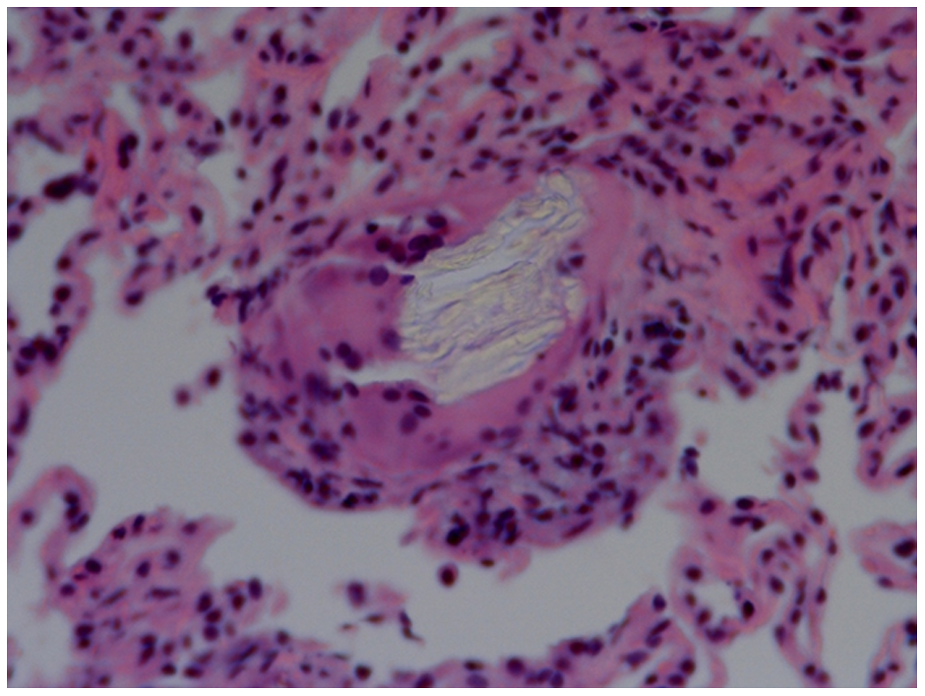
Hematoxylin and eosin stain for an endobronchial lung biopsy demonstrating giant cell formation surrounding a pulmonary arteriole obstructed by microcrystalline cellulose particles (original magnification ×400).
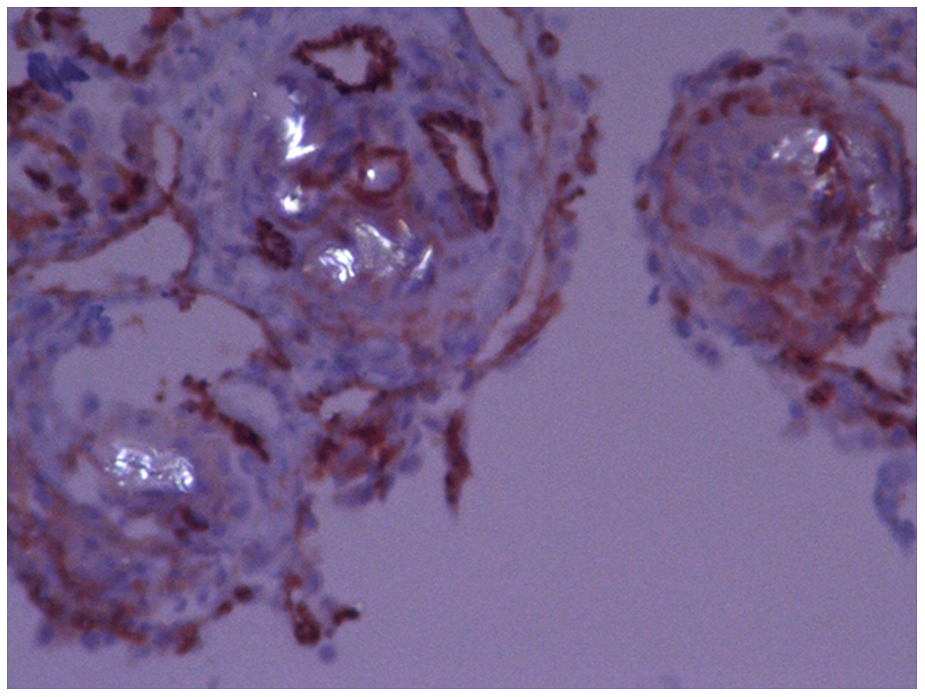
Polarizing light microscopy demonstrating birefringent microcrystalline cellulose particles in pulmonary arterioles (original magnification ×400).
Pulmonary function tests (PFTs) showed moderate restriction of lung volume compartments and reduction of diffusion capacity, suggestive of moderate interstitial lung disease with a moderate parenchymal gas exchange defect, and hypoxia with exertion. The patient’s condition stabilized, his indwelling IV access was removed and he was treated with oral steroids as an outpatient.
Discussion
Abuse of prescription narcotic analgesics is a growing crisis in the United States and is now a common cause of death. However, pulmonary vascular disease is an infrequently recognized complication associated with this problem. Foreign body granulomatosis has been discovered in IV drug abusers who inject medications designed for oral use.1,2 The trapping of the particles in the arteriole wall causes phagocytosis by macrophages and giant cells which leads to granuloma formation, emphysema, right ventricular hypertrophy, and pulmonary hypertension.1,2 Microcrystalline cellulose-induced foreign body granulomatosis should be considered in patients who present with pulmonary complaints that have venous access.1,7
Diagnosis of foreign body granulomatosis is often a diagnosis of exclusion. It is not typically on the initial differential diagnosis, unless the patient’s history indicates IV drug abuse.3,6 As is the circumstance in the current case, oftentimes patients do not divulge a history of substance abuse even when questioned. The diagnosis of foreign body granulomatosis is often made after other common conditions have been excluded. A CT image of the chest may reveal the presence of nodules associated with foreign body granulomatosis.1,3 However, a lung biopsy is required in order to diagnose foreign body granulomatosis.3,4,6 Microcrystalline cellulose can be stained with Congo red and Grocott’s methenamine silver, aiding in the diagnosis.4,6,7
There is no specific treatment for foreign body granulomatosis with the exception of lung transplantation. 3 Pulmonary hypertension associated with foreign body granulomatosis should be treated with vasodilators.3,9 Whether or not inhaled or oral steroids play a role in the treatment of foreign body granulomatosis is debatable.3,10 Houck et al. describes the use of oral prednisone in a patient with cellulose granuloma-induced pulmonary hypertension. The use of prednisone resulted in a decrease in labored breathing, a drop in pulmonary artery and mean arterial pressure, as well as symptomatic relief of chest pain. 5 Chau et al. showed an improvement in dyspnea, hemoptysis, and chest X-ray within 1 week of inhaled budesonide treatment. 10 These case reports demonstrated the potential benefit of steroids in patients with foreign body granulomatosis.5,10
In conclusion, for patients presenting with acute right ventricular strain but who fail to demonstrate evidence of pulmonary embolization or another identifiable cause of pulmonary hypertension, consideration should be given to illicit injection of oral narcotics as a cause of foreign body-induced perivascular granulomatosis and pulmonary hypertension.
Footnotes
Conflict of interest
The authors declare no conflicts of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.