
Abstract

Acute pulmonary embolism (PE) is associated with high rates of morbidity and mortality. 1 Timely management of acute decompensated PE improves pulmonary artery pressure and right ventricular function for patients with intermediate- and high-risk PE,2,3 although not all hospitals offer comprehensive PE care services. 4 Despite the potential role for a multidisciplinary PE rapid response team in facilitating the transfer process for this high-risk population, 5 systematic transfer protocols for PE care have not been widely developed or endorsed by societal guidelines.4,5 We aimed to examine trends, outcomes, and predictors of patients transferred with PE.
The Nationwide Inpatient Sample (NIS) was queried for all patients hospitalized between 2008 and 2019 with a primary diagnosis of acute PE by using the 9th and 10th revisions of the International Classification of Diseases. 6 Patients were categorized according to whether they were transferred versus not transferred from another acute care hospital using the NIS transfer data element. 7 We excluded hospitalizations in which patients had concomitant codes for ST-elevation myocardial infarction or stroke. This analysis was exempt from institutional review board due to the NIS deidentified nature.
The primary outcome was in-hospital mortality. The secondary outcomes included: (i) annual trends of patients transferred with acute PE, and separately in those who received intervention (defined by concomitant systemic or catheter-directed thrombolysis or thrombectomy, surgical embolectomy); and (ii) independent predictors of patients transferred with PE. Separate multivariable regression models were conducted to explore in-hospital mortality among patients with PE who were transferred versus not, and independent predictors for patients transferred with PE (see the online supplemental material). A linear trend test was used for trend analyses. A p-value less than 0.05 was considered statistically significant. Because the NIS is a stratified sample, all analyses were weighted for discharge to allow national estimation. 6
Among 1,907,110 hospitalizations with a primary diagnosis of PE, 107,753 (5.7%) were transferred from another hospital. The median age was 63 (39–87) in patients transferred with PE versus 64 (40–88) in those not transferred. Men constituted 51% in those transferred with PE versus 47.2% who were not. Transferred patients were more likely to receive systemic thrombolysis, 12.0% versus 4.0%; catheter-directed thrombolysis, 5.8% versus 1.6%; catheter-directed thrombectomy, 1.1% versus 0.3%; and surgical embolectomy, 1.3% versus 0.1% (p for all < 0.001). Patients transferred with PE were associated with higher rates of cardiogenic shock, 2.6% versus 0.6%, and were more likely to have required mechanical ventilation, 6.2% versus 2.4% (p for both < 0.001).
The unadjusted rate of in-hospital mortality was higher among patients transferred with PE (5.0% vs 2.6%, p < 0.001). After adjustment, in-hospital mortality remained significantly higher among patients transferred with PE (odds ratio 1.27, 95% CI: 1.23–1.32; p < 0.001). Whereas among those who received intervention (n = 91,193), there was no difference in the in-hospital mortality among transfer versus nontransfer (odds ratio 1.04, 95% CI: 0.96–1.13; p = 0.32).
The overall rate of patients transferred with PE increased over time (3.7% in 2008 vs 8.5% in 2019 [relative increase 56.5%]; p < 0.001) as well as among those who received intervention during index admission (9.0% in 2008 vs 18.2% in 2019 [relative increase 50.5%]; p < 0.001) (Figure 1). The rate of in-hospital mortality decreased among all transferred patients (6.1% in 2008 vs 4.0% in 2019 [relative reduction 34.4%]; p < 0.001), as well as among those who received intervention (18.0% in 2008 vs 5.7% in 2019 [relative reduction 68.3%]; p < 0.001). Disparities related to sex and race were noted among predictors of transfer with PE: women were less likely to be transferred (odds ratio 0.88, 95% CI: 0.78–0.93; p < 0.001) and Black race was also associated with a lower odds for transfer (odds ratio 0.48, 95% CI: 0.38–0.51; p < 0.001) (Figure 1).
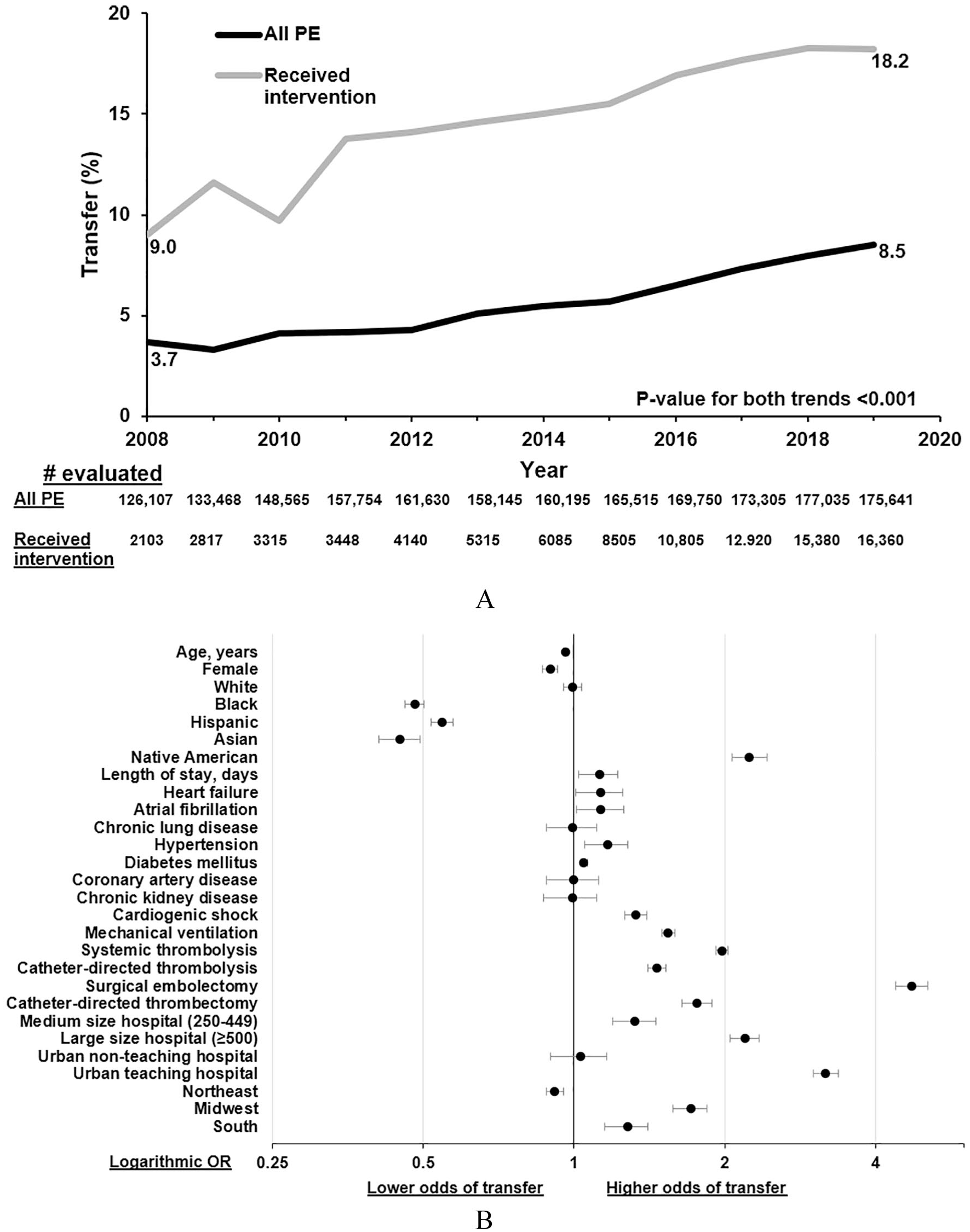
Nationwide Inpatient Sample data between 2008 and 2019 showing the trends
This analysis includes important limitations. We could not ascertain that PE was the only reason for transferring the patient; however, limiting our analytic cohort to primary diagnosis with PE which is defined by NIS as the main reason for hospitalization 6 and excluding other conditions that mandate transfer, decrease the risk of contamination for our analytic cohort. We were unable to define patients with intermediate- to high-risk PE who did not receive intervention, determine the severity of cardiogenic shock, or contraindications to either thrombolytics or surgical embolectomy.
In this nationwide analysis, patients transferred with PE were more complex and had a higher risk of mortality relative to patients who do not require transfer; however, among those who received intervention, there was no difference in the in-hospital mortality among transfer versus nontransfer. The rate for patients transferred with PE has increased over time, with improvement in mortality rates and a higher relative reduction among those who received intervention. This may indicate improved recognition that safe and effective treatments for PE exist for this high-risk group of patients, warranting transfer of care; however, future studies are required to examine whether those interventions are associated with reduced mortality or cost-effectiveness. Previous research focused on sex and racial disparities in presentation, management, and outcomes for patients with PE.8,9 Our study is adding a different perspective with a notable lower chance of transfer with PE if patients were women or Black race, which requires more investigation. Further research should evaluate the characteristics of patients with PE requiring transfer for higher acute care in order to develop standardized protocols for this process.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X221117607 – Supplemental material for Trends, outcomes, and predictors of patients transferred with acute pulmonary embolism in the United States: Analysis of the Nationwide Inpatient Sample
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X221117607 for Trends, outcomes, and predictors of patients transferred with acute pulmonary embolism in the United States: Analysis of the Nationwide Inpatient Sample by Ahmed Elkaryoni, Islam Y Elgendy, Marwan Saad, David Luke, Islam Shatla, Sovik DeSirkar, Matthew C Bunte, J Dawn Abbott, Herbert D Aronow and Amir Darki in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Islam Y Elgendy receives research funding from Caladrius Biosciences, Inc.; J Dawn Abbott receives research funding from MicroPort and Boston Scientific, serves on advisory boards of Philips and Medtronic, and is a consultant for Abbott and ReCor; and Herbert D Aronow is a consultant for Philips and Silk Road Medical.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.