
Abstract
Background
Although many epidemiological studies show an association of cigarette smoking with suicide the path to the latter is not well understood.
Objective
Using causal inference methodology with observational data, to examine if smoking leads indirectly to suicide through mental health hospitalization.
Design
The study used 11 waves of a cross-sectional national health survey that was linked with hospitalization and death registers.
Methods
The data came from Canadian Community Health Survey respondents (n = 723 665) between the years 2000 and 2014. These respondents agreed to link their data with hospitalization and death registers and were followed for an average of 9.18 (SD: 4.42; range: 3 to 17) years. Mediation models, one each for men and women, were created in which lifetime daily smoking was the exposure, mental health hospitalization was the mediator, and death by suicide was the outcome, adjusting for 11 covariates reported at survey participation.
Results
In both men and women, the direct effect of daily smoking was larger than the indirect effect through hospitalization for mental conditions. The direct effect of smoking was 1.76 (95% CI: 1.47-2.10) for men and 2.60 (95% CI: 1.90-3.57) for women. The indirect effect through mental health hospitalization was 1.07 (95% CI: 1.05-1.09) for men and 1.04 (95% CI: 0.99-1.09) for women.
Conclusion
A relatively smaller proportion of the daily smoking-suicide association is transmitted indirectly through mental health hospitalizations compared to a direct effect. Suicide interventions focusing on people hospitalized for mental disorders may miss many suicidal people, so primary prevention and secondary prevention of smoking are crucial.
Keywords
Introduction
The Global Burden of Disease Study reported that for the 27-year period from 1990-2016, suicide remained among the top 10 causes for years of life lost. 1 In North America, there were 51 000 deaths in the same period or an age-standardized mortality rate of 12.7 deaths per 100 000 1. This is higher than Western Europe (9.6) and about the same as Eastern sub-Saharan Africa (12.5). 1 Suicide deaths can result from several contributing factors including mental disorders,2,3 physical illness requiring hospitalization,4,5 job-related strain, 6 loss of income, 7 and substance use disorders. 8 Since not all factors are foreseeable or preventable, it is important to find modifiable targets of prevention. A meta-analysis of prediction models for suicide attempts or deaths found that these models have a positive predictive value close to zero. 9 This suggests that early suicide prevention efforts may be more fruitful.
Globally, tobacco smoking accounts for about 9 million deaths yearly 10 for 20 percent of cardiovascular deaths in the USA. 11 Cancer and cardiovascular disease are the leading tobacco-related causes of death, so tobacco’s harmful effects on mental health in general, and suicide in particular are overlooked. The predominant view is that smoking is a form of self-medication because nicotine relieves negative emotions, 12 inattention in ADHD, 13 or improves cognition in schizophrenia.14,15 One implication of this view is that the treatment of mental disorders would reduce the need for a coping mechanism. Two alternative views are that (i) smoking and mental disorders are bidirectional 16 and (ii) smoking is harmful for mental health. 17 The latter two raise smoking prevention or cessation as potential suicide prevention levers.
The association of smoking with subsequent death by suicide is consistently observed in both cross-sectional and longitudinal studies.18-22 For this reason, it is important to examine the contribution of smoking to deaths other than from cancer and cardiovascular disease. Whether smoking causes suicide has not been shown unlike its link with these other deaths. The debate is due in part to the lack of a widely accepted, plausible biological mechanism. One possibility is that smoking contributes to serotonin depletion in the brain, 23 more so in those with a pre-existing deficit in serotonin binding in the prefrontal cortex (PFC), an important region for mood regulation and inhibitory control.24,25 Cigarette smoke alters monoamine transmission 26 and decreases the density of gray matter in the PFC. 27 Unlike unmodifiable exposures (i.e., genes) or past events (adverse child experiences), smoking is modifiable throughout the lifetime. To varying degrees, every smoker can quit and be persuaded to do so—something that distinguishes it from other suicide risk factors. However, no study to our knowledge has compared the relative efficacy of prevention vs cessation.
There is also increasing evidence that smoking is a risk factor for mental disorders. A previous study with UK Biobank data found that smoking behavior was associated with hospitalization for mental illness after controlling for genetic predisposition to smoking and trait negative affectivity. 28 Smoking-related genes and smoking behavior equally accounted for the hazard of mental health hospitalization. 28 Another study reported that four disorders had particularly high population attributable fractions for suicide attempts: major depression, borderline personality, nicotine dependence, and posttraumatic stress. 29 A survey covering 33 countries and more than 100 000 youth from 12 to 15 years of age reported that primary use of tobacco was associated with 3.4 times higher odds of a suicide attempt. 30 Secondhand smoke exposure was also associated with higher odds of a suicide attempt among adolescent girls. 30 Likewise, a US-based study found that secondhand smoke exposure was associated with higher depressive symptoms in never smokers (but not in former smokers). 31
With the large number of risk factors for suicide, population studies are better powered than clinical studies to distinguish correlation from causation. Causal inference models can be used to verify if a causal interpretation of the smoking-suicide link is warranted. These models involve counterfactual or potential outcomes reasoning. An associational finding compares the risk of an outcome in the treated with the risk of an outcome in the untreated, where these groups are disjoint subsets. 32 In contrast, causal inference asks the hypothetical question: what if the entire population had been treated (untreated)? The term treatment applies to experiments, but causal inference applies to observational studies also, in which an exposure is the putative cause. 33
A causal argument in observational studies requires several assumptions. The most important one is exchangeability: the idea that people assigned to different treatments are comparable or the risk of the outcome is the same for all treatment levels. 33 In an experimental study, random assignment balances the variables affecting the outcome. 32 If the participants assigned to treatment and control groups in a randomized controlled trial were switched, the outcome should remain the same if exchangeability were satisfied.
With observational studies, exchangeability can be satisfied only if a sufficient set of confounders is adjusted for in the analysis. 34 Given such a set, conditional exchangeability can be achieved by means of stratification or inverse probability weighting. 33 Mediation models require that confounders affecting the exposure-outcome, mediator-outcome, exposure-mediator relationships are entered in the model. These variables should also be in the correct temporal sequence 35 to ensure that the confounders are not affected by the exposure, mediator, and outcome. 36 The other two assumptions for the validity of a causal argument in observational studies are discussed in Supplemental File 1, Section A.
Our review of the literature led to the hypothesis that smoking causes suicide and this is mediated by hospitalizations for mental disorders. Accordingly, the objective of the present study was to estimate direct and indirect effects of smoking on suicide with mental health hospitalizations as a mediator and a large set of confounders.
Methods
Data Sources
The participants were Canadian Community Health Survey (CCHS) respondents, pooled over 11 waves between 2000-2014. CCHS is an annual cross-sectional survey of community-dwelling residents 12 years old and above. For the 11 waves, the total number of respondents was 910 839 people. A total of 753 046 (83%) agreed at survey participation to have their data linked with hospitalization and death registers. Please refer to Supplement 1, Section B for the numbers (proportions) of people participating and agreeing to share their data at each wave.
Statistics Canada obtained the consent of CCHS participants in two stages: first to participate in the survey itself and secondly to link their survey data with national hospitalization (past and future) and death records (future). 37 The first stage is an implicit consent by volunteering to participate 38 while the linkage is an explicit consent. The authors of this paper were not involved in securing consent from the participants and were merely granted access to the data. Researchers granted access to the data are exempt from securing an ethics approval or waiver based on Canada’s Statistics Act 39 and the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2). Article 2.2 40 . Researchers are required to become “deemed employees” of Statistics Canada, thereby putting the work under the scope of the Statistics Act which allows “every person employed or deemed to be employed” to “analyse, abstract and publish statistical information relating to the commercial, industrial, financial, social, economic and general activities and condition of the people.” 39 At the editor’s request, we obtained an ethics waiver from the university’s ethics board as this paper was under review.
The hospitalization files captured both day visits and inpatient admissions from 1999-2017. Outpatient mental health visits to psychiatrists and general practitioners are not captured. Day visits are captured by the National Ambulatory Care Reporting System and inpatient admissions, by the Discharge Abstract Database. Although CCHS data was linked with all hospital admissions and day visits, henceforth, we use the term “hospitalization” to refer to mental health related ones only (see the ICD codes under Variables of Interest below for a list of mental health diagnoses).
Death records were provided by the Canadian Vital Statistics Database (CVSD) and covered the years 2000-2017. Data linkage was performed by Statistics Canada as described in a report. 37 Since the hospitalization and death registers cover all Canadian residents, we had complete follow-up data for death up to December 31, 2017. These deaths were observed over a mean follow-up of 9.18 years (SD:4.42; range: 3-17).
Inclusion in our study sample was determined by the eligibility to participate in the CCHS. These are: non-institutionalized people 12 years and above. CCHS does not cover full-time Armed Forces members, First Nations people living in reserves, homeless people, and certain remote locations. 37 Using the dates associated with age of smoking initiation, survey completion, hospitalizations, and deaths, we created an analytical sample that satisfied the temporal precedence required by causal inference. Hence, people who had a mental health hospitalization prior to (or in the same year as) smoking initiation were excluded. For the huge majority, age of smoking initiation came before a mental health hospitalization. Only 220 people were first hospitalized for a mental health condition and then later smoked, while 158 people had both events in the same year. We also excluded people who had a mental health hospitalization before participating in the survey. This exclusion was done to enforce the correct temporal sequence of the exposure (smoking), mediator (mental health hospitalization), and outcome (suicide) variables. After excluding people with missing baseline covariates and those whose mental disorders preceded their smoking initiation, the resulting analytical sample consisted of 723,665 people.
We performed a sample size calculation using data from our UK Biobank paper on suicide. 20 UK Biobank data was used because the calculation was performed before access to the data in the present work was obtained. To achieve 80 percent power to detect a significant mediation effect at an alpha of .05, a sample of 95 275 people was required. This was number was obtained by fitting two regression models (exposure to outcome, mediator to outcome given the exposure) adjusting for sex and 10 confounding variables. The model coefficients were then provided as input into the powerMediation package 41 in R.
Variables of Interest
Suicide deaths were indicated by ICD codes X60-X84 in the CVSD. The exposure variable (ever daily smoking) and timing were indicated by the questions “Were you ever a daily smoker?” and the age of smoking initiation. Smoking was assessed only once, and this was at survey participation. Mental health hospitalizations were indicated by ICD-10 codes for substance misuse (F10-19), depression (F32-F39), anxiety (F40-F49), schizophrenia and related disorders (F20-F29), mania (F30-F31), and intentional self-harm (X60-X84). See Supplementary File 1, Section B for details.
We entered a wide range of baseline covariates reported at survey completion. The most important of these was ever considering suicide during the lifetime. The other covariates are known suicide risk (or protective) factors including low income, First Nations ancestry, having children below 12 years old, mean self-rated health, marital status, immigrant status, alcohol drinking in the last 12 months, previous year employment, completion of postsecondary education, and age at survey participation. Education, lower socioeconomic status, substance use, and psychiatric disorders are related both to smoking and suicide and are therefore confounders.11,22,42
Participants also reported whether they were cis- or trans-gender but this variable had a 48 percent missing rate, so it was not entered as a covariate in the models. The rest of the variables had equal to or less than 20 percent missing, so these were handled by multiple imputation. Five imputations were created using the mice package. 43 The five imputed copies were then used to build mediation models.
Causal Mediation Models
The hypothesized mediation models, one each for men and women, can be visualized in Figure 1. These models decompose the total effect into a natural direct effect (NDE) and natural indirect effect (NIE). The definitions for NDE and NIE are given in context in the Results and the formulas are in Supplementary File 1, Section C. Typically, men have at least twice the suicide death rates of women
44
and they are at higher risk for suicide when divorced or separated.
45
Hence, we created separate causal mediation models for men and women using the R package medflex.
46
In essence, medflex creates an extra row for each person where the exposure level is set to the counterfactual (ie, not a daily smoker if the individual was a daily smoker) but fixing the mediator to the observed value.
47
The counterfactual outcome is then imputed based on the two alternative exposure values, the mediator, and the baseline covariates. Hypothesized model of smoking (exposure), mental health hospitalization (mediator), and suicide death (outcome). Dashed lines represent the indirect path and solid line the direct path. Only people who had the correct temporal sequence of exposure, mediator, and outcome were included. Separate models for men and women were estimated and adjusted for the following confounding variables: ever considered suicide, low income, First Nations ancestry, having children below 12 years old, mean self-rated health, marital status, immigrant status, alcohol drinking in the last 12 months, previous year employment, completion of postsecondary education, and age at survey participation.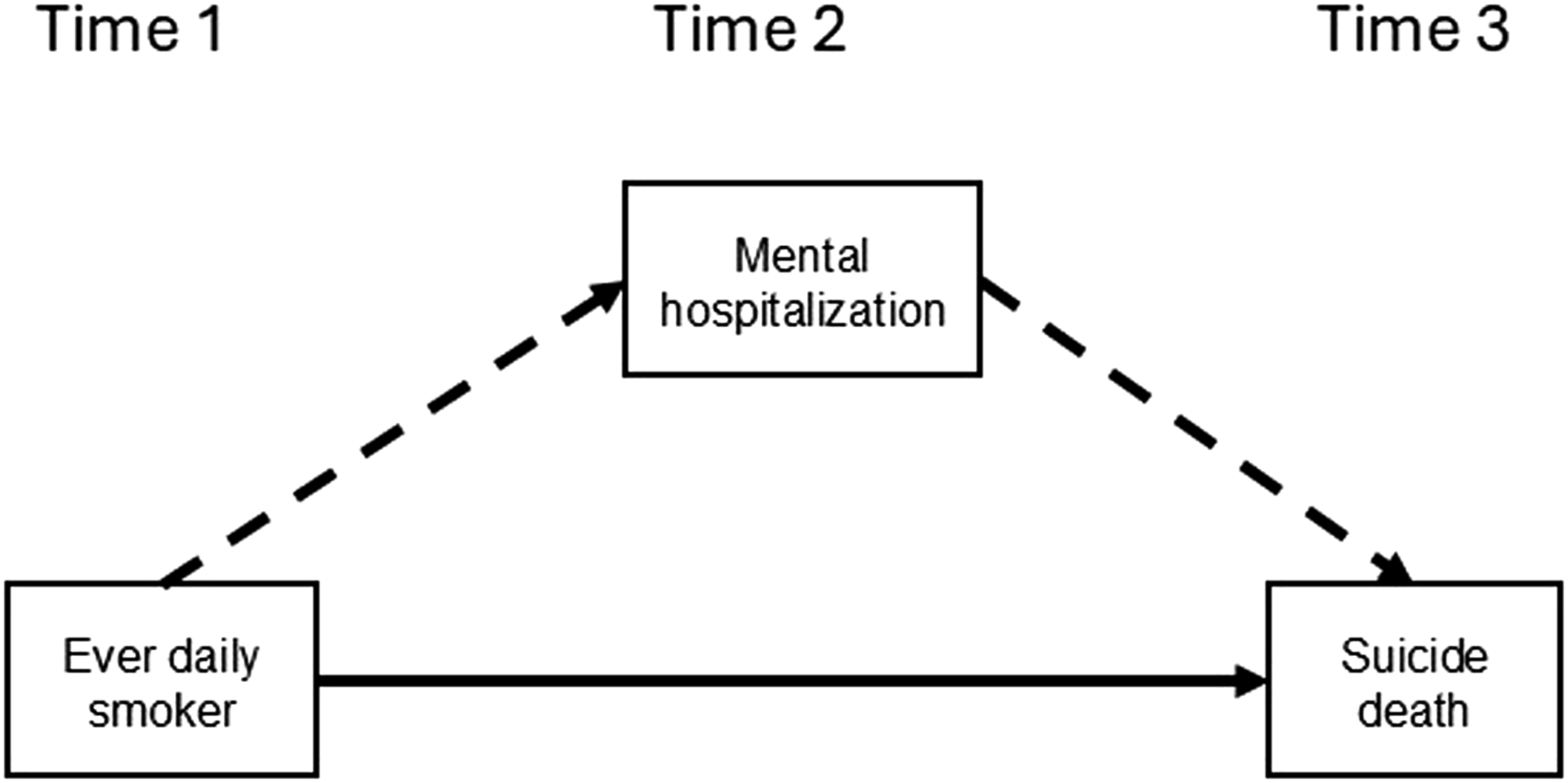
Mental health hospitalization and suicide are both dichotomous variables, so a logistic link was used in mediator and outcome models. The models allowed for a possible interaction between exposure and mediator, even when these were not statistically significant, as suggested by VanderWeele. 35 This interaction term allows the indirect effect to vary by exposure level.
Sensitivity Analysis for Unmeasured Confounding
The pathway from daily smoking to suicide (direct effect) was assessed for potential unmeasured confounding using the E-value. 48 This was motivated by the lack of genomic data from participants—an unmeasured confounder. The E-value is an estimate of how large an effect a missing confounder should have on the exposure-outcome association to preclude a causal interpretation by reducing it to null. 48 Once the E-value was calculated it was then compared to the magnitude of the strongest baseline confounder, to get a sense of the bias.
Population Attributable Fraction (PAF)
PAFs estimate the proportion of a disease that could be avoided if a risk factor could be eliminated. 49 We estimated pathway-specific PAFs for the direct and indirect effects of smoking. This was implemented in the R package graphPAF50,51. Sensitivity analysis for the PAF estimates was also performed to examine the effect of an omitted variable and the low number of suicides on the PAF estimates. Supplementary File 1, Section D describes the calculation of PAFs in men and women.
Results
Characteristics of Respondents to the Canadian Community Health Survey (2000-2014) at Survey Completion
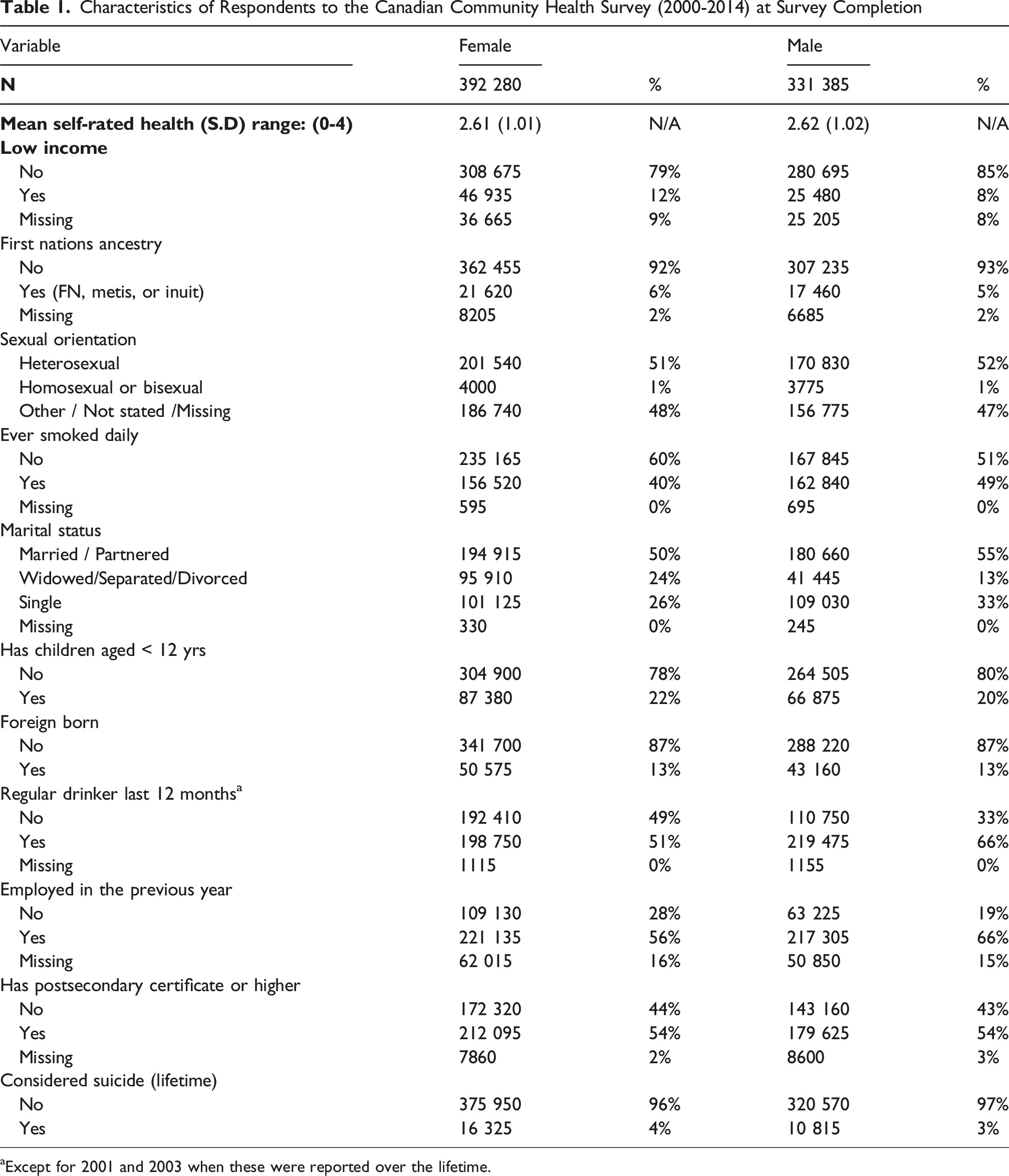
aExcept for 2001 and 2003 when these were reported over the lifetime.
Age at Various Milestones for Respondents to the Canadian Community Health Survey (2000 – 2014)

aThis was the baseline event. The ages of first smoking (daily smoking) were self-reported during the survey. The ages at first mental health hospitalization and suicide death were derived from hospital or coroner records.
Causal Mediation Models
The NDE is defined as “the expected exposure-induced change in outcome when keeping the mediator fixed at the value that would have been naturally observed if unexposed 46 (page 4).” For men, the NDE of smoking for suicide was 1.76 (95% CI: 1.47-2.10). In other words, changing ever daily smoking from “No” to “Yes” and controlling mental health hospitalization at naturally observed values if unexposed (and adjusting for baseline covariates) increases the odds of suicide by 1.76. The NDE for women was 2.60 (95% CI: 1.90-3.57).
Natural Direct and Indirect Effects of Daily Smoking on Suicide for Men in the Canadian Community Health Survey (2000-2014)

aMH = mental health hospitalization ** Except for 2001 and 2003 when these were reported over the lifetime.
Natural Direct and Indirect Effects of Daily Smoking on Suicide for Women in the Canadian Community Health Survey (2000-2014)

aMH = mental health hospitalization **Except for 2001 and 2003 when these were reported over the lifetime.
The mediated interaction effect for men was significant (OR: 0.96 95% CI: 0.95-0.97) but not for women (OR: 1.00, 95% CI: 0.94-1.07). The former suggests that men smokers with a mental health hospitalization are 0.96 times as likely to die of suicide than non-hospitalized ones, ie, men smokers who were hospitalized had lower suicide risk. Figure 2 is a visual representation of the natural effects, with separate models by sex. Natural Effects of Smoking on Suicide Death in the Canadian Community Health Surveys 2000-2014.
Sensitivity Analysis for Unmeasured Confounding
For men, an unmeasured confounder would have to have an odds ratio of 2.92 to shift the point estimate to null, and 2.30 to shift the lower limit of the confidence interval to null. In relative terms, the missing confounder(s) should be as strong as “ever considering suicide” at baseline. For women, the unmeasured confounder should be 4.64 for the point estimate and 3.21 for the lower limit of the confidence interval. By comparison, the odds ratio of ever considering suicide for women was 3.69, suggesting that the missing confounder(s) should exceed its effect.
Population Attributable Fractions (PAF)
Sensitivity Analysis of How the Proportion Attributable Fraction (PAF) Changes by Omitting a Strong Covariate a and Oversampling Suicide Deaths in the Canadian Community Health Survey (2000-2014)

aThis was “ever considered suicide in the lifetime” at baseline.
bThe numbers differ from those of the causal mediation models due to missing values.
Discussion
We calculated natural direct and indirect effects of daily smoking on suicide in a representative cohort of Canadians. In both men and women, the direct effects were larger than the indirect effect via mental health hospitalizations. For both men and women, the direct effect of daily smoking (in the odds ratio scale) was larger than all other baseline covariates except for lifetime suicidal ideation (Tables 3 and 4). We further found that an unobserved confounder(s) would need to be as strong as lifetime suicidal ideation in men to make the direct effects vanish, and stronger than the same for women. Taken together, our results indicate that daily smoking is probably a causal factor for suicide. Our calculation of PAFs indicate that eliminating smoking would reduce the suicide burden by 27 percent in men and 42 percent in women.
Our study showed that the mean ages for smoking initiation, mental health hospitalizations, and suicide deaths tend to occur in that sequence, if they occur at all. This aligns with a UK Biobank study which showed that smoking initiation tends to occur before mental health hospitalizations. 28 The present work adjusted for a large set of baseline confounders—probably an adequate set. Admittedly, risk factors such as childhood sexual abuse or bullying were not available. On the other hand, it can be argued that lifetime suicidal ideation and self-rated general health are suitable proxy variables because they are downstream relative to childhood events, 52 but upstream of mental health hospitalizations. This means that these variables capture part of the risk, although residual confounding likely remains. For this reason, our E-value analysis quantified how strong an unmeasured confounder should be to nullify the direct effect of smoking on suicide.
Without a plausible biological mechanism, our findings would amount to nothing more than an exercise in number crunching. Previously offered biological mechanisms neglected the unity of brain and body, because of the mind-body dualism of Western psychiatric tradition. 53 We hypothesize that smoking-induced inflammation in the periphery may contribute to central nervous system (CNS) inflammation, 54 thereby worsening mood and mental health. Elevated plasma levels of cytokines (eg, IL-6, TNF-α) and C-reactive protein have been consistently found to be associated with major depression.55,56 Additionally, their induction by endotoxin injection has been linked to anxiety and depressed mood. 57 The view of the brain as an immune-privileged organ was refuted by the discovery of the glymphatic system. 58 It provides a pathway for bodily inflammation to reach the CNS 59 and allows the immune system to surveil the CNS. 60 Furthermore, microglia, the brain’s resident immune cells, have been implicated in neuroinflammation, with smoking-induced toxins triggering a shift to a pro-inflammatory state. 61 Inhibiting microglial activation has been shown to alleviate depressive symptoms in animal models, while postmortem studies have revealed greater microglial activation (though not consistently) in people with mental disorders or dying from suicide. 62
Our proposed mechanism requires biological studies to verify or refute and it is offered as a testable hypothesis and not a positive finding. Targeting inflammation has been suggested as a means of suicide prevention (see Brundin 63 for a review) in clinical samples. Cigarette smoke is a highly pro-inflammatory agent with carcinogenic, mutagenic, and cytotoxic components. 64 Therefore, we propose that the primary prevention of smoking is a form of suicide prevention. Compelling evidence of cigarette smoke as a pathogen (vis-à-vis nicotine) is the lower cancer rate in users of Swedish snuff (which has high nicotine content) compared with cigarette smokers. 65 Similarly, tobacco smoking was associated with higher multiple sclerosis risk, which was untrue of Swedish snuff use. 66 Considering that smoking harms respiratory, cardiovascular, reproductive systems, it would be the absence of harmful effects on mental health that ought to be more surprising. Yet the idea that bodily inflammation can cause major depression is a disruptive one in psychiatry. 53
Whether changes in smoking policies influenced suicide rates is a question addressed by two ecological studies. Grucza and colleagues studied if cigarette taxes and smoke-free policies in 50 states in the US were related to suicide deaths from 1990-2004. 67 They found that either policy by itself or combined with the other measures reduced suicide deaths within each state. They estimated that a $1 increase in cigarette tax results in a 10.5% decrease in suicide risk. 67 In Korea, the impact of a quit line number, an 80% price hike, and graphical warnings were analyzed. 68 Their interrupted time series analysis showed that these policies were associated with a reduction in suicide deaths.
Physicians are influential actors in smoking cessation, but a Cochrane review found a relatively small influence. Compared to a natural quit rate of 1 to 3 percent, physician advice increased quite rates by another 1 to 3 percent. 69 Psychiatry was the least likely specialty to offer smoking cessation support to its patients. 70 Given the limited impact of cessation, population-wide reduction of exposure to smoking and second-hand smoke seems more promising.30,31,70
The present study was subject to several limitations. First, genomic data for the participants was not available. We mitigated this by estimating a minimum effect size required for a polygenic score to make the effect of daily smoking disappear. Secondly, our single mediator was mental health hospitalizations. There could be other potential mediators such as mental health disorders that did not result in hospitalization. This was the actual mediator of interest because many mental disorders begin in late adolescence or early adulthood, and therefore more proximal to smoking initiation. Unfortunately, this was not available in the data, so we relied on hospitalized mental disorders as a proxy. It is probable that despite adjustment for confounds, what we call the “natural direct effect” of daily smoking includes other mediating variables. This may also have resulted in a higher-than-expected PAF of daily smoking. For women especially, the lower number of suicide deaths in the sample may have led to an inflated PAF of the direct effect. Note however, that for women, the confidence interval of the indirect effect straddles 1, so a higher direct effect and PAF are to be expected. The sampling frame of the CCHS covers only community dwelling individuals so our findings may not apply to people living in institutions, Canadians living in First Nations reserves, homeless individuals and full-time Armed Forces members. People who participate in national surveys such as the UK Biobank 71 tend to be healthier than average and we expect this to be true of the CCHS also. A longitudinal record of changes in smoking status was not available because each participant had smoking data for one wave only. For this reason, we cannot rule out a bi-directional relationship between smoking and mental health disorders.
Finally, our analysis inherits the limitations of causal modeling itself, of which the most important one is that all relevant covariates have been entered. Whether we achieved conditional exchangeability is fundamentally untestable. It would therefore be valuable for future studies to replicate our analysis in sample with a larger number of suicide deaths, mental disorders not leading to hospitalization, and genomic information.
Conclusion
A relatively smaller proportion of the daily smoking-suicide association is transmitted indirectly through mental health hospitalizations compared to a direct effect. Two possible explanations are: (1) the direct effect is probably mediated by other pathways, and it is important to identify what these are, (2) there is a true direct effect of daily smoking on suicide deaths. Significant effects through both pathways may co-exist. Suicide interventions focusing on people hospitalized for mental disorders may miss many suicidal people, so primary prevention and secondary prevention of smoking are crucial.
Supplemental Material
Supplemental Material - Does the Path From Cigarette Smoking to Suicide Death Go Through the Hospital? A Causal Mediation Analysis in a National Canadian Sample
Supplemental Material for Does the Path From Cigarette Smoking to Suicide Death Go Through the Hospital? A Causal Mediation Analysis in a National Canadian Sample by Lloyd Balbuena, Fredrik Åhs, Evyn Peters, Ana Mendes-Silva, and Doug Speed in Tobacco Use Insights
Footnotes
Acknowledgements
The authors acknowledge the support of Dr Ruben Mercado of Statistics Canada for reviewing the statistical outputs prior to release. This research was conducted at Saskatchewan Research Data Centre (SKY-RDC), a part of the Canadian Research Data Centre Network (CRDCN). This service is provided through the support of the Canada Foundation for Innovation, the Canadian Institutes of Health Research, the Social Sciences and Humanities Research Council, and Statistics Canada, and through the support of the University of Saskatchewan. All views expressed in this work are our own.
Author Contributions
LB acquired the data, applied for funding, conceptualized the study, performed the statistical analysis, and wrote the initial draft. FA critically reviewed the initial draft and contributed to the writing. EP critically reviewed the initial draft and contributed to the writing. AMS critically reviewed the initial draft and contributed to the writing. DS conceptualized the study, reviewed the statistical analysis and contributed to the writing. All authors approved the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received funding from the Royal University Hospital Foundation, which did not participate in the analysis, interpretation, and writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this project were provided by Statistics Canada and accessed through one or more of the RDCs (Research Data Centre) in the Canadian Research Data Centre Network (CRDCN). The following datasets were used in this project: Canadian Community Health Surveys 2000-2014, Canadian Vital Statistics Database, National Ambulatory Care Reporting System, and the Discharge Abstract Database.Because of the confidential nature of these microdata, they cannot be shared. Researchers in Canada working at one of CRDCN’s member institutions can access the data at no additional cost to the researcher. Other researchers will have to pay cost-recovery to access the data. Access to the data is subject to a background check and research approval process. The protocols for data access, including fees for researchers at non-CRDCN institutions, can be found on the CRDCN website. https://www.statcan.gc.ca/rdc-cdr/eng/user/login. ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.