
Abstract
Introduction
Persons living with HIV (PLWH) use tobacco at higher rates than the general population in both high-income countries and low- and middle-income countries. Tobacco use rates are increasing in sub-Saharan Africa, the home to most of the world’s PLWH. As the reach of antiretroviral therapy (ART) expands and HIV-related morbidity and mortality wanes, tobacco use is emerging as a leading cause of disease and death in PLWH. A better understanding of tobacco use behaviors in various settings will be crucial to designing optimal tobacco control strategies.
Methods
In late 2019, we enrolled 50 PLWH cigarette smokers from 6 clinical sites in Nairobi, Kenya (4 HIV care clinics and 2 methadone maintenance programs) for one-on-one interviews focusing on their behaviors and beliefs related to tobacco use.
Results
Fifty PLWH smokers completed the interviews. The mean age was 38.5 ± 9.7 years (range 20-57 years) and 68% were male. All were currently receiving ART. They smoked a mean of 14.9 ± 12.4 cigarettes per day, and 82% reported smoking every day. Only 6% reported dual use of smokeless tobacco products. Nicotine dependence was moderate or high in 74%. More than a third (36%) reported a prior history of tuberculosis. In our sample, use of other substances was common, especially alcohol, marijuana, and methadone. On the motivation to quit scale, 90% were at least in the contemplation stage, but only 2% had ever received behavioral cessation counseling, and only 8% had ever used pharmacotherapy (exclusively nicotine replacement therapy). Participants reported significant concern about developing smoking-related illness, exposing others to secondary smoke, and the financial burden associated with their tobacco use. Measures of intrinsic and extrinsic motivation to quit, smoker and abstainer self-concept, and social support yielded encouraging results regarding the possibility of successful quitting.
Conclusions
Tobacco use is an important health concern in PLWH in Kenya. A more thorough understanding of their tobacco use behaviors and beliefs will provide critical information for providers, public health officials, and policy makers as they redouble their efforts to confront this urgent health challenge.
Introduction
Notwithstanding regional successes in the public health battle against tobacco use, cigarettes remain the leading preventable cause of death in the world today. Unless significant changes in smoking behaviors occur, tobacco use will claim over a billion lives in this century.1,2 More than 80% of these unnecessary deaths will occur in low- and middle-income countries.1,2 The World Health Organization (WHO), in its Framework Convention on Tobacco Control (FCTC), established in 2003 with 180 nation-signatories, took concerted action against these trends. 3 Despite these efforts, smoking prevalence in Africa is projected to rise from 15.8% in 2010 to 21.9% in 2030.2,4
In 2018, 37.9 million people were living with HIV in the world, and 25.6 million of these (67.5%) were living in sub-Saharan Africa. 5 Low- and middle-income countries in South America, Asia, and Africa consistently report elevated smoking rates in persons living with HIV (PLWH). 6 This has emerged as a critical public health challenge since in the era of effective antiretroviral therapy (ART), tobacco use has overtaken all other causes as the leading driver of mortality in PLWH.7,8
Kenya is a nation of over 53 million people in East Africa. Similar to many non-Western countries, cigarette smoking is a largely male practice in Kenya, with very low rates among females. The most recent available national statistics estimate current smoking prevalences of 17.3-22.0% among Kenyan men and .18-2.0% among Kenyan women.2,9,10 The most recent Global Youth Tobacco Survey (2013) demonstrated a troubling rise in the female:male ratio (4.0% of girls:9.6% of boys) among Kenyan adolescents smoking tobacco. 11 In addition to the male predominance, smoking is concentrated among the poorer and less-educated strata and among those who drink alcohol. 10 Tobacco use in Kenya is also entangled with illicit substance use.12,13 The government of Kenya has been extremely proactive in its battle against tobacco use, and it has led all other African nations in its implementation of the FCTC.4,14
Kenya is also home to 1.6 million PLWH, 68% of whom are receiving ART. 15 Smoking rates are higher in Kenyan PLWH than in the general population, and the PLWH in Kenya smoke at higher rates than the PLWH of any other East African country. 6 Over 26% of male Kenyan PLWH and over 1% of female Kenyan PLWH smoke cigarettes. 6 Certain subgroups of Kenyan PLWH smoke at much higher rates, for example, those in methadone maintenance programs, where tobacco use prevalences can approach 100% (unpublished data, Mathare and Ngara methadone clinics in Nairobi, Kenya). Although sub-Saharan Africa is home to more PLWH smokers than any other area in the world, aside from limited research conducted in South Africa,16,17 there is little in-depth information about tobacco use beliefs and behaviors in PLWH smokers from this region.
In 2018, we initiated a project aimed at gathering information about cigarette smoking behaviors in Kenyan PLWH with the goal of using these data to develop a culturally appropriate tobacco treatment intervention. We present herein the results of a structured interview that was conducted in a cohort of PLWH smokers in Nairobi.
Methods
Between September and November 2019 trained staff completed a cross-sectional interview study of a sample of PLWH smokers in Kenya. They administered structured interviews about tobacco use to PLWH smokers recruited from 4 HIV care clinics and 2 methadone maintenance facilities in Nairobi. A prescreening form was given to clinicians in these clinics to identify HIV-infected smokers who were willing to quit and to participate in the formative study. Those meeting the criteria were referred to the study clinic for further evaluation by the research assistants (RAs) and to complete the informed consent process. Of the 58 individuals who were referred, 50 agreed to participate and completed the study.
The RA read the questions for the participant in Swahili or English and noted his/her responses on the questionnaire. Each interview took between 1-2 hours. Participants were paid 500 Kenyan shillings (approximately USD $5) upon completion.
Tobacco behaviors and beliefs measures.

Note: Ref. = reference, NA = not applicable (measure was developed by the investigators).
Interview responses were keyed into a REDCap database. Categorical variables are presented as proportions, and continuous variables are presented as means and standard deviations. All statistical analyses were completed using SPSS V26.0.
The study was approved by the Institutional Review Board of the University of Maryland and the Ethics and Research Committee of the Kenyatta National Hospital/University of Nairobi (Approval #901/12/2018).
Results
Sociodemographic and clinical characteristics of study participants.
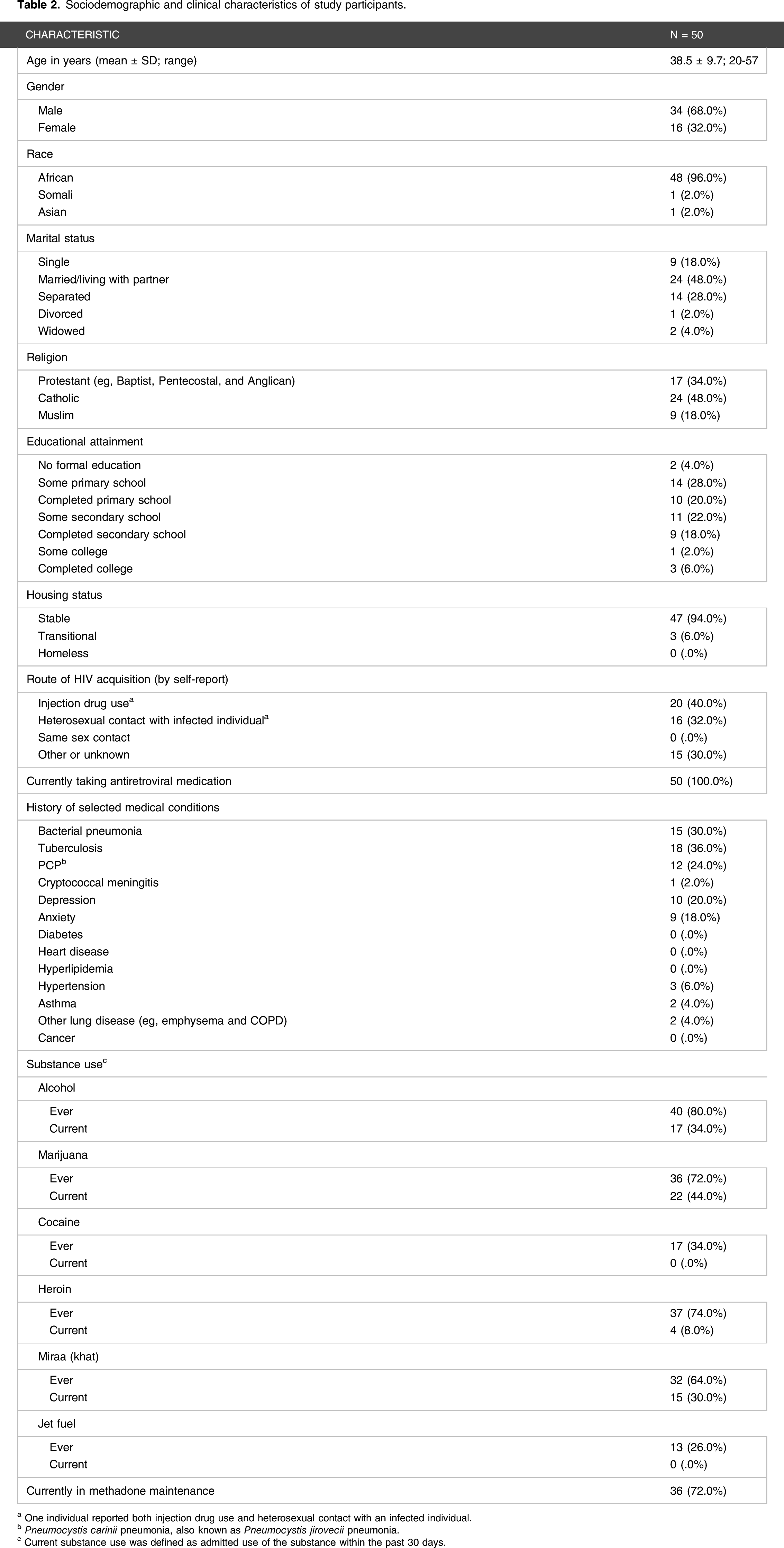
a One individual reported both injection drug use and heterosexual contact with an infected individual.
b Pneumocystis carinii pneumonia, also known as Pneumocystis jirovecii pneumonia.
c Current substance use was defined as admitted use of the substance within the past 30 days.
Tobacco use behaviors of study participants.

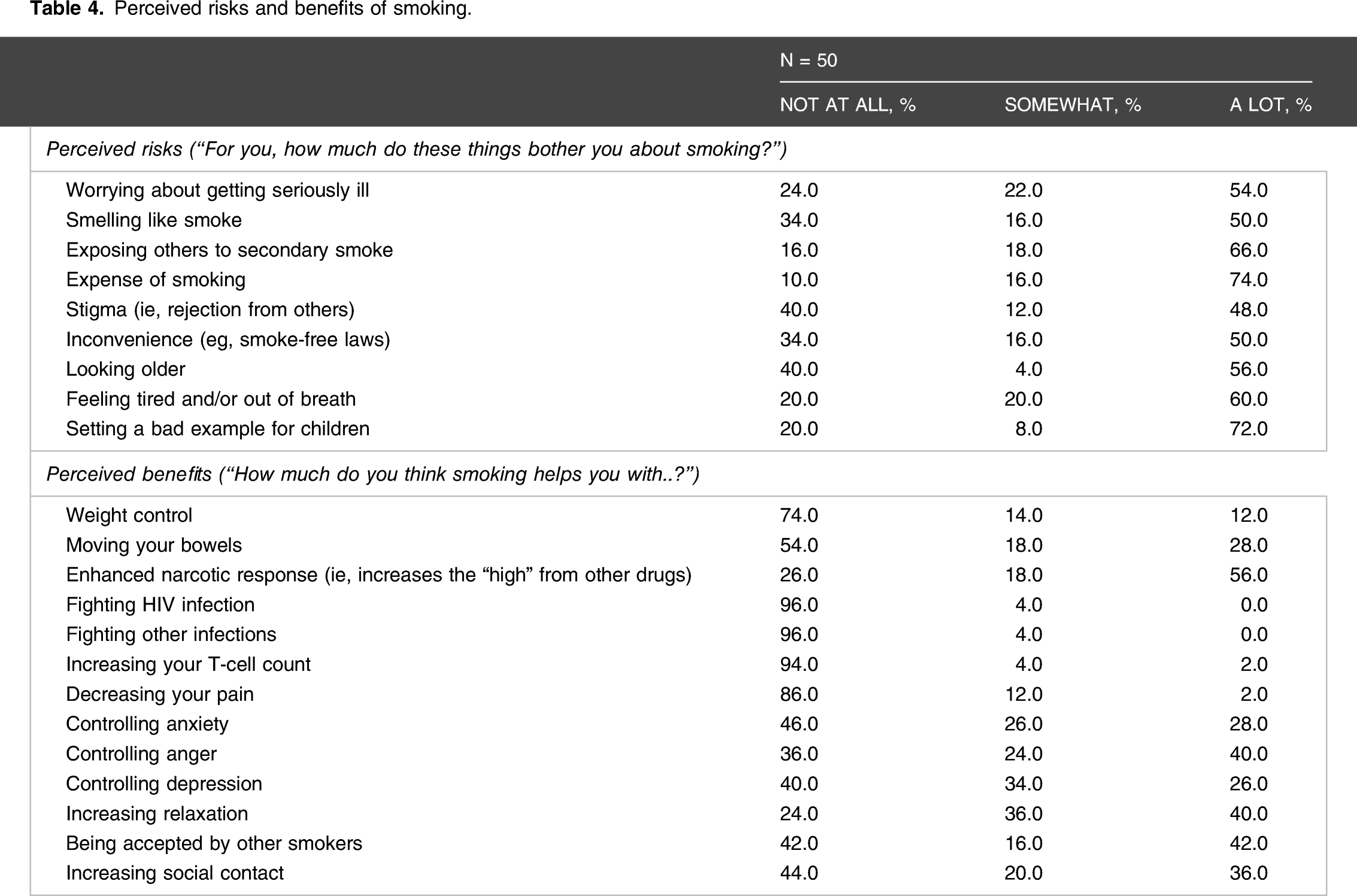
Perceived risks and benefits of smoking
Perceived risks and benefits of smoking.
Comparative risk
The investigators developed a 10-item questionnaire asking participants to estimate their own risk compared to other people attending their clinics of dying from a range of medical (eg, HIV and cancer) and non-medical (eg, random violence and motor vehicle accident) causes. The majority (67-77%) rated themselves at higher risk for deaths from HIV infection, cancer, and heart disease, and at lower risk for deaths from violent or traumatic causes. Only 6.0% thought themselves more likely to die of old age than the other patients in their clinics.
Knowledge about the direct risks of smoking and of second-hand smoke
The investigators developed a 13-item True/False questionnaire asking participants whether cigarette smoking (via direct inhalation or second-hand exposure) caused or increased the risk of a variety of medical conditions, all of them known to be tobacco-related. The great majority answered, correctly, that cigarette smoking increased the risk for a variety of cancers and cardiovascular and pulmonary diseases. Of note, 98% believed that smoking increased the risk of tuberculosis, whereas only 40% believed that it increased the risk of bacterial pneumonia. The great majority also endorsed the belief that second-hand smoke increases the risk of neoplastic, cardiac, and pulmonary diseases.
Importance of quitting and interest in specific smoking cessation interventions
The investigators developed a 1-item scale to assess the importance of quitting: 1 = not important to 10 = extremely important. Quitting smoking was rated as extremely important by 94% of participants.
Asked which cessation strategies they would be interested in using (Yes/No), participants reported interest in the following non-mutually exclusive categories: individual counseling 100.0%, nicotine replacement therapy 92.0%, oral medications 82.0%, buddy support 74.0%, and group counseling 72.0%.
Advice from general practitioner/primary care providers about smoking cessation
Fifty-six percent of participants stated that their general practitioners (GP) had discussed smoking cessation with them, 2.0% reported that their GPs recommended or prescribed pharmacotherapy to assist them to quit, 18.0% reported having received brochures about quitting from their GPs, and 12.0% reported having been referred to a smoking cessation program. None of the participants expressed the belief that their providers smoked cigarettes. Sixty-four percent indicated their belief that their cigarette smoking was a very important health issue to their GP, and 14% indicated their belief that it was unimportant.
Current life stressors
The investigators developed a 6-item questionnaire asking participants to rate the severity of a range of life stressors on a 4-point Likert scale: 0 = ”None” to 3 = ”Major.” The percentages of participants who rated the severity of stress as either moderate or major for the various stress domains follow: financial 88.0%, safety 26.0%, relationships 26.0%, sexual abuse 6.0%, and job-related 68%.
Discussion
Similar to the experience in Western countries 10 years ago, with the advent of effective and accessible ART in Kenya, 7 cigarette smoking in Kenyan PLWH is poised to emerge as a leading killer in this group. Developing effective smoking cessation interventions for PLWH has been a challenge, 31 and it is reasonable to expect that getting established PLWH smokers to quit in Kenya will be difficult as well. In order to create a culturally appropriate cessation strategy in a new target population, one must begin by understanding the social and behavioral milieus of their tobacco use and how they may differ from those of other smoking populations. Accomplishing this task often relies upon the examination of aggregate statistics, for example, national reports, and the performance of thoughtfully constructed structured interviews and focus groups in subsets of the target population. In the process of developing a cessation intervention for PLWH smokers in Kenya, we have done both. Herein we report the results of a structured interview on cigarette smoking behaviors and beliefs conducted in a group of 50 PLWH smokers in Kenya.
Our participant sample had a mean age of 38.5 and was predominantly male, similar to the gender pattern of smoking in the nation as a whole.2,9,10 The mean daily cigarette consumption of 14.9 is higher than the national average of 8 cigarettes per day. 2 It is notable that all of our participants purchased their cigarettes as single sticks and not as packs. This may be a strategy to lessen the financial burden of smoking (a pack of cigarettes costs approximately 140 KES/1.20 USD, and the cost of a single stick ranges from 5-25 KES/0.05-.23 USD), and it may reduce the impact of package-based tobacco warnings. It is likely that the heavy representation of persons in methadone maintenance contributed to the relatively high cigarette consumption rate and the cigarette purchasing behaviors of our sample. Both nicotine dependence levels and motivation to quit were high in our sample. Similar to the national surveys, dual tobacco use was uncommon, and there was little use of medications to assist quit attempts.2,9,10 Our participants had relatively low educational attainment and high levels of past or present alcohol and drug use. They reported low levels of smoking-related comorbidities, although 36% of them had had tuberculosis.
The locus of control measure assessed our participants’ perception of factors contributing to their involvement with smoking. The scale permits the separate evaluation of intrapersonal (control resides within the participant), interpersonal (control resides with other individuals), and fate (smoking and quitting are outside of human control). Higher intrapersonal locus of control beliefs predicts better health-related behavior outcomes. 32 Our observation that locus of control scores were equivalent across the intrapersonal, interpersonal, and fate domains suggests that a counseling intervention should try to strengthen the belief that a smoker is the ultimate decisor of his/her tobacco use, and not others or fate. Intrinsic and extrinsic motivations to quit are important predictors of successful cessation, and higher levels of intrinsic vs extrinsic motivation are predictive of better cessation outcomes. 21 Our participants’ significant tilt toward intrinsic motivation suggests that they may be more amenable to cessation interventions. Their significant self-conceptual identification with the abstainer persona over the smoker persona is also a favorable predictor of successful quitting. 22
Anxiety and depression both play important roles in cigarette smoking. 33 The rates of anxiety and depression that we observed were much lower than the 61.7% and 73.3% rates reported in a US sample of PLWH smokers. 34 The interactions of psychiatric illness with HIV, tobacco use, other substance use, and poverty are complex and multilayered, and assumptions about anxiety and depression derived from data in the US are not necessarily applicable to sub-Saharan Africa 35 or other areas of the world. The relationship of anxiety and depression to tobacco use in Kenya is beyond the scope of this project, but it is a worthy topic for future research. Although coping with chronic pain is an important driver of tobacco use in certain populations, 36 only about a quarter of our sample reported severe pain in the past 7 days.
In accordance with the national sample surveyed by the International Tobacco Control (ITC) Project, 2 we observed near universal recognition of the health harms of cigarette smoking and significant concern over the damage that smoking could do to themselves and to those around them. In contrast to the ITC report, a large majority of our participants were concerned with the financial costs of their smoking. The leading causes of stress identified by our participants were financial and job-related. In comparison to other groups that we have studied in the United States, 37 our participants did not minimize their risk of suffering serious health consequences of smoking, including death, when they compared themselves to other patients in their clinics.
Slightly more than half of participants reported that their primary health care providers had discussed smoking cessation with them, but few offered them any sort of cessation assistance. The government of Kenya has been a leader in promoting tobacco control throughout the nation. Further measures may be indicated to better recruit health care professionals into this effort and to put more cessation resources at their disposal.
Finally, we found high levels of spiritual well-being in our participants. Despite the enormous socioeconomic and health challenges that they faced, they scored high on self-assessments of meaning, peace, and faith. For those who are counseling such individuals to quit, this may provide a source of strength and resolve to smokers trying to overcome their addiction to cigarettes.
Our study had several weaknesses that require mention. The sample size was small and inferences from a group of this size should be interpreted with caution. Participants were recruited from several care centers, but all within Nairobi. They may not be representative of Kenyan PLWH from other locales or from non-urban areas. The majority of our sample was in methadone maintenance. This likely contributed to the larger proportion of women in the group than would be expected from national cigarette smoking statistics. Although substance use is common in cigarette smokers and vice versa, our findings may not be fully generalizable to a non-substance-using PLWH population. Finally, the data collection methodology, that is, direct questioning by study staff, introduces concern for social desirability bias and likely accounts, in part, for the extremely high interest in quitting reported by our participants.
Conclusions
A significant proportion of Kenyan PLWH, especially the men, are current cigarette smokers. The health implications of their tobacco use are destined to increase as the wide availability of effective antiretroviral therapy puts control of their HIV infection within reach. Leading concerns among PLWH smokers are the potential effects of second-hand smoke on those around them, setting a bad example for children, and the financial costs associated with cigarette smoking. Along with the direct health effects of cigarettes on their smokers, smoking cessation counseling should emphasize some of these ancillary harms and explain the benefits of quitting in a similarly expansive manner. Studies such as this one will be vital in elucidating the social and behavioral underpinnings of tobacco use in this very vulnerable group so that culturally appropriate smoking cessation strategies may be devised and implemented.
Footnotes
Acknowledgments
The authors acknowledge with gratitude the cooperation of the study participants in permitting us to complete this research.
Authors’ Contributions
J.S., S.A.O., E.K., and S.S.H. planned the study, oversaw its conduct, and prepared the manuscript. P.O., M.O., and L.K. performed the research. A.O.A., T.W.M., W.P., M.E.B., and A.H.W. contributed within their areas of expertise (pharmacy, clinical trial management, and behavioral psychology) to data interpretation and to the review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by award 1R01CA225419 (S.S.H., PI, J.S. and S.A.O., MPI) from the National Institutes of Health (NIH)/National Cancer Institute (NCI) and by the Einstein-Rockefeller-CUNY Center for AIDS Research (P30-AI124414) which is supported by the following NIH co-funding and participating institutes and centers: NIAID, NCI, NICHD, NHBL, NIDA, NIMH, NIA, FIC, and OAR. None of these sources were involved in the design, analysis, data interpretation, writing, or decision to publish the completed manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.
Authors’ Note
This research was presented in part at the 23rd annual International AIDS Conference [virtual], July 6-10, 2020, Poster PED1274.