
Abstract
Background:
Antimicrobial resistance (AMR) is one of the top 10 public health threats. One approach to tackling the AMR menace could involve expanding the range of AMR surveillance domains to include hospital wastewater (HWW), a domain that has largely been overlooked by researchers.
Aim:
To evaluate the occurrence of multidrug-resistant bacteria in hospital wastewater of the Korle Bu Teaching Hospital (KBTH).
Methodology:
This was a longitudinal study involving 288 HWW samples consecutively collected across 12 weeks from the pool of wastewater emanating from 2 critical care units of KBTH—The Child Health Unit and the Maternity Unit—on Mondays and Thursdays, each week. The samples were cultured for bacteria, which were identified using the Matrix-Assisted Laser Desorption/Ionization-Time of Flight (MALDI-TOF) technique and subjected to antimicrobial susceptibility testing via the Kirby-Bauer method.
Results:
In total, 294 bacteria of 23 different types, all being Gram-negative, were isolated from the 288 samples. The predominant ones were Escherichia coli (30.6%, n = 90), Klebsiella pneumoniae (11.2%, n = 33), Citrobacter freundii (10.9%, n = 32), Alcaligenes faecalis (5.8%, n = 17), and Pseudomonas mendocina (5.4%, n = 16). The prevalence of multidrug resistance among the isolates was 55.4% (n = 163). Moreover, the prevalence of extended-spectrum beta-lactamase (ESBL) producers was 15.6% (n = 46). E. coli accounted for the most ESBL-producing organisms (28.9%, n = 26).
Conclusion:
The wastewater generated by the Maternity and Child Health Units of KBTH harbored a wide range of multidrug resistant bacteria, with a good proportion of these being ESBL producers, and the predominant one being E. coli. The study thus identifies the wastewater of KBTH as an important source of multidrug resistant organisms, and underscores the significance of appropriate treatment of wastewater of the hospital and other clinical, and related settings prior to its discharge.
Keywords
Introduction
The World Health Organization (WHO) has listed antimicrobial resistance (AMR) as one of the top ten public health threats facing humanity. 1 The cost of AMR to the economy is significant, spanning across prolonged illness and longer hospital stays, the need for more high-priced medicines (thereby, causing financial challenges for those impacted), as well as disability and death.2 -4 One recent systematic analysis estimated 4.95 million deaths to have occurred in 2019 from bacterial AMR. 5 According to another estimate, not less than 700 000 lives are lost each year from drug-resistant diseases. 1 By 2030, AMR could force up to 24 million people into extreme poverty, and by 2050, it could result in the loss of 10 million lives each year. 1
The high public health threat posed by AMR demands that efforts aimed at curbing the menace are done holistically. One approach could involve expanding the range of AMR surveillance domains, such as expanding them to include hospital wastewater (HWW), a significant source of multidrug-resistant pathogens.6 -14 That notwithstanding, the majority of AMR surveillance efforts in sub-Saharan Africa have focused on human and animal populations,15 -26 with little attention paid to the environment27 -31 (In this context, the environment refers to ambient air, soil, water, and other locations that are neither on or within the bodies of humans and animals, as conceptualized by Huijbers et al. 32 ). Elsewhere, AMR surveillance in the environment has spanned a variety of domains, including hospital wastewater, domestic wastewater, surface water, and sewage.33 -42 The little attention paid to the environment presents a major setback to having robust AMR surveillance data, a key that is critical to unlocking the AMR conundrum, and may explain some of the bottlenecks regarding the effective management of the AMR menace.
As filling the identified knowledge gaps is important, this study aimed to evaluate the occurrence of multidrug-resistant bacteria in wastewater of the Korle Bu Teaching Hospital (KBTH). Specifically, the prevalence of different bacteria present in the hospital wastewater, the spatio-temporal distribution of the predominant wastewater-contained bacteria, and the prevalence of antimicrobial resistance and multidrug-resistant organisms, especially, extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae among the hospital wastewater isolates, were investigated. Such insights, particularly, the distribution of HWW bacteria spatially and temporally, are limited in sub-Saharan Africa.27 -31
Methods
Study site, design and sampling
This was a longitudinal study conducted in the Greater Accra Region of Ghana. Being a tertiary referral hospital and a premier health facility that caters to an estimated population of 15 million people within southern Ghana, the Korle Bu Teaching Hospital (KBTH) was selected for this study. KBTH is equipped with 2000 beds and a central laboratory with several departments, including Microbiology to which all microbiological specimens from patients are brought for processing. Hospital wastewater sampling was done at the Maternity and Child Health units of the hospital, specifically, at the outlets where wastewater exit the wards after being contaminated with microorganisms (prior to discharge into surface waters). These 2 units were selected owing to their being critical care units and the relatively easier accessibility of their wastewater effluents.
Sterile bottles were used for the collection of the untreated wastewater samples. A total of 288 grab samples of 100 ml volumes each (144 from each Unit) were systematically collected. The sampling was done across 12 weeks, on 2 days—Mondays and Thursdays—each week, twice each sampling day (morning and evening), to ensure that the sampling was consistent and well-spaced. Three samples were collected per sampling site at each sampling time (at intervals of 20 minutes), in the months of October to December 2021 at ambient temperatures, ranging from 24°C to 31°C. Hence 24 samples were collected each week from both units. In the mornings, samples were collected between 7:00 a.m. and 8:00 a.m., and in the evenings, between 5:00 p.m. and 6:00 p.m. The samples were kept on ice and conveyed to the research laboratory (within 2 hours) of the Department of Medical Microbiology, University of Ghana Medical School, which is located on the hospital compound, for microbiological analysis.
Laboratory investigations
Isolation and identification of bacteria
Each sample was cultured for bacteria by direct streaking of 0.5 ml of it on 5% sheep blood agar and chocolate agar (Oxoid Ltd., Basingstoke, Hants, UK) (the resultant plates of which were incubated at 37°C in 5% CO2), as well as mannitol salt agar and MacConkey agar (Oxoid Ltd., Basingstoke, Hants, UK) (the resultant plates were aerobically incubated at 37°C). After 18 to 24 hours of incubation, each of the plates was examined for growth, and subcultures done (including for 6 of the plates that had mixed bacterial growth) until pure cultures were obtained. The pure bacterial cultures were subsequently identified using a combination of colonial morphologies, motility, biochemical tests (including catalase, oxidase, urease, indole, citrate, sugar fermentation [triple sugar iron test]), and the Matrix-Assisted Laser Desorption/Ionization-Time of Flight (MALDI-TOF) biotypher, and stocked.
Antimicrobial susceptibility testing
Following the directives of the Clinical and Laboratory Standards Institute (CLSI), 43 disk diffusion assay on Mueller-Hinton agar plates (Oxoid Ltd., Basingstoke, Hants, UK) were used; the antimicrobials used were amikacin (30 µg), ampicillin (10 µg), cefuroxime (30 µg), ceftriaxone (30 µg), ceftazidime (30 µg), cefepime (30 µg), ciprofloxacin (10 µg), trimethoprim-sulfamethoxazole (1.25/23.75 µg), imipenem (10 µg), ertapenem (10 µg), gentamicin (10 µg), and amoxicillin-clavulanate (20/10 µg). Using a nephelometer, a suspension similar in turbidity to that of 0.5 McFarland standard was achieved by emulsifying the test isolate in normal saline. A sterile cotton swab was dipped into the suspension and swabbed evenly across the entire surface of a Mueller Hinton agar plate (Oxoid Ltd., Basingstoke, Hants, UK), in 3 different dimensions. This was done to obtain a semi-confluent growth following incubation. The plates were incubated at 37°C for 18 to 24 hours, after which the zones of inhibition around the antimicrobial disks were measured and interpreted according to the breakpoints of the CLSI. 43 Escherichia coli ATCC 25922 was used as control strain. The CLSI 43 guidelines were used for the interpretation of the bacterial isolates being resistant, susceptible or intermediate. A bacterial isolate was regarded as multidrug-resistant when they showed resistance to 3 or more classes of antimicrobial drugs.
Phenotypic screening for extended-spectrum beta-lactamase in enterobacteriaceae
A standard inoculum (0.5 McFarland) of test isolate was streaked on Mueller Hinton agar and tested for ceftazidime (30 µg) and cefotaxime-clavulanic acid (30 µg/10 µg) using the double-disk synergy test (DDST). A disk of clavulanic acid was placed in the center of Mueller Hinton agar plates (90 mm) at 20 mm distance to ceftazidime and cefotaxime. ESBL production was detected by the appearance of keyhole effect due to the enhanced activity of ceftazidime and cefotaxime with clavulanic acid. E. coli ATCC 25922 and Klebsiella pneumoniae ATCC 700603 were used as negative and positive control strains, respectively.
Data analysis
Data were entered into and analyzed with Microsoft Excel, 2019, and Statistical Products and Services Solutions (SPSS), version 25. The data on the types of bacteria and their spatio-temporal distribution, as well as antimicrobial resistance data were summarized using descriptive statistics. Chi square tests were used to compare the 2 critical care units with regard to the proportions of the bacteria isolated from their wastewater effluents, at an alpha level of .05.
Results
Prevalence and types of bacteria present in the hospital wastewater
The 288 samples collected from the wastewater pools of the 2 critical care units selected for this study—Maternity and Child Health—yielded 294 bacterial isolates, with all being Gram-negative. The Maternity Unit accounted for 48.0% (n = 141) of these, whereas the Child Health Unit accounted for 52.0% (n = 153).
The bacteria were of 23 different types, with the predominant ones being Escherichia coli (30.6%, n = 90), Klebsiella pneumoniae (11.2%, n = 33), Citrobacter freundii (10.9%, n = 32), Alcaligenes faecalis (5.8%, n = 17), and Pseudomonas mendocina (5.4%, n = 16). Besides Escherichia coli recording the highest prevalence (30.6%, n = 90), it was the only organism whose proportion significantly differed between the 2 units studied [Maternity Unit = 23.8%, n = 37; Child Health Unit = 38.0%, n = 53, p = .02]. The distribution of the organisms isolated from the wastewater samples is presented in Table 1.
Prevalence of the bacteria in the hospital wastewater samples.
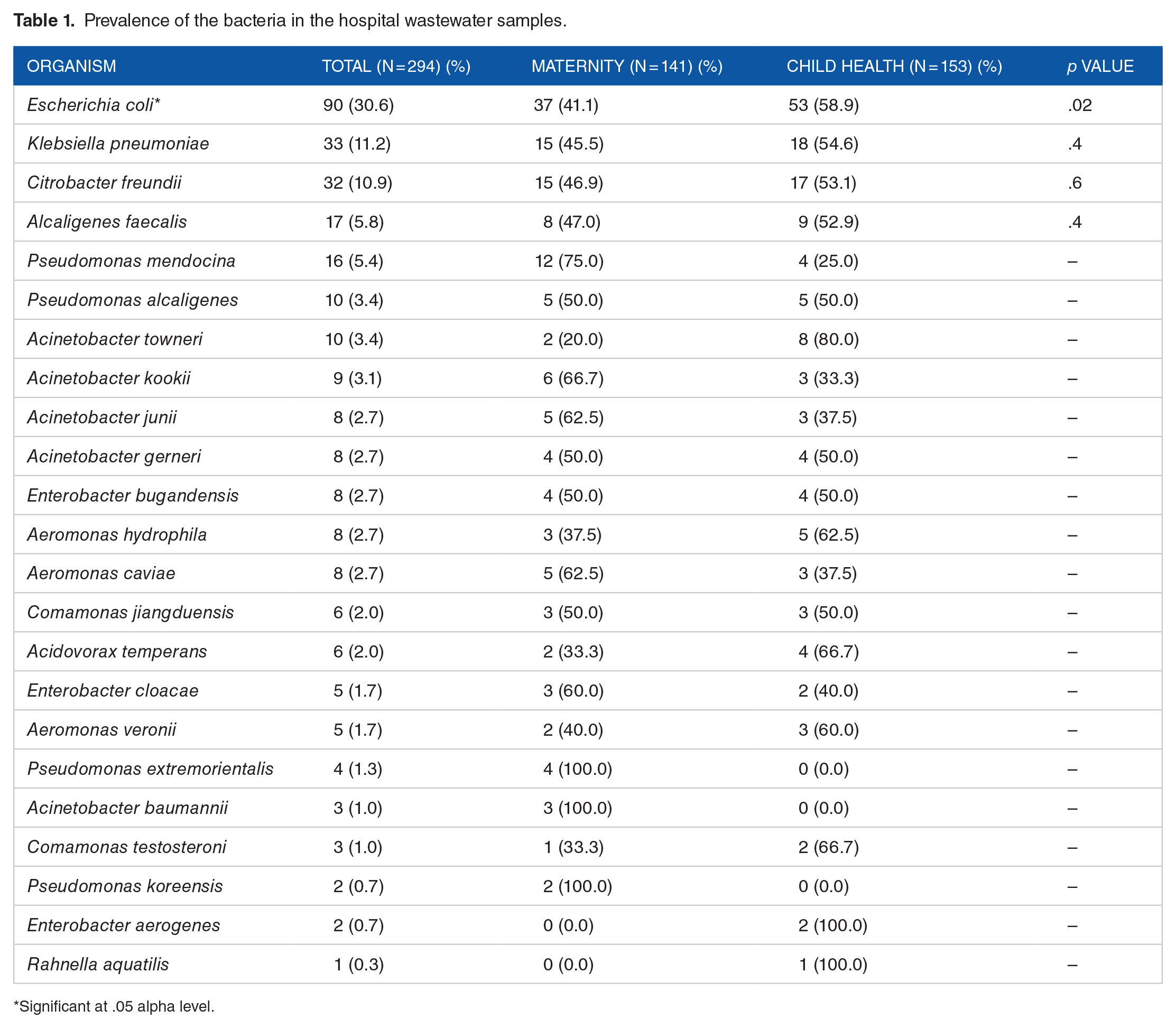
Significant at .05 alpha level.
Spatio-temporal distribution of the predominant bacteria isolated from the hospital wastewater samples across the 12 weeks of sampling
As observed in Figure 1, Escherichia coli was present in the wastewater samples collected from the Maternity Unit throughout Weeks 1 to 6 for the first days of sampling of those weeks. The organism, however, demonstrated an intermittent occurrence (Weeks 1 to 3, Weeks 5 and 6, Week 9, and Weeks 11 and 12) on the second days of sampling (Figure 1).
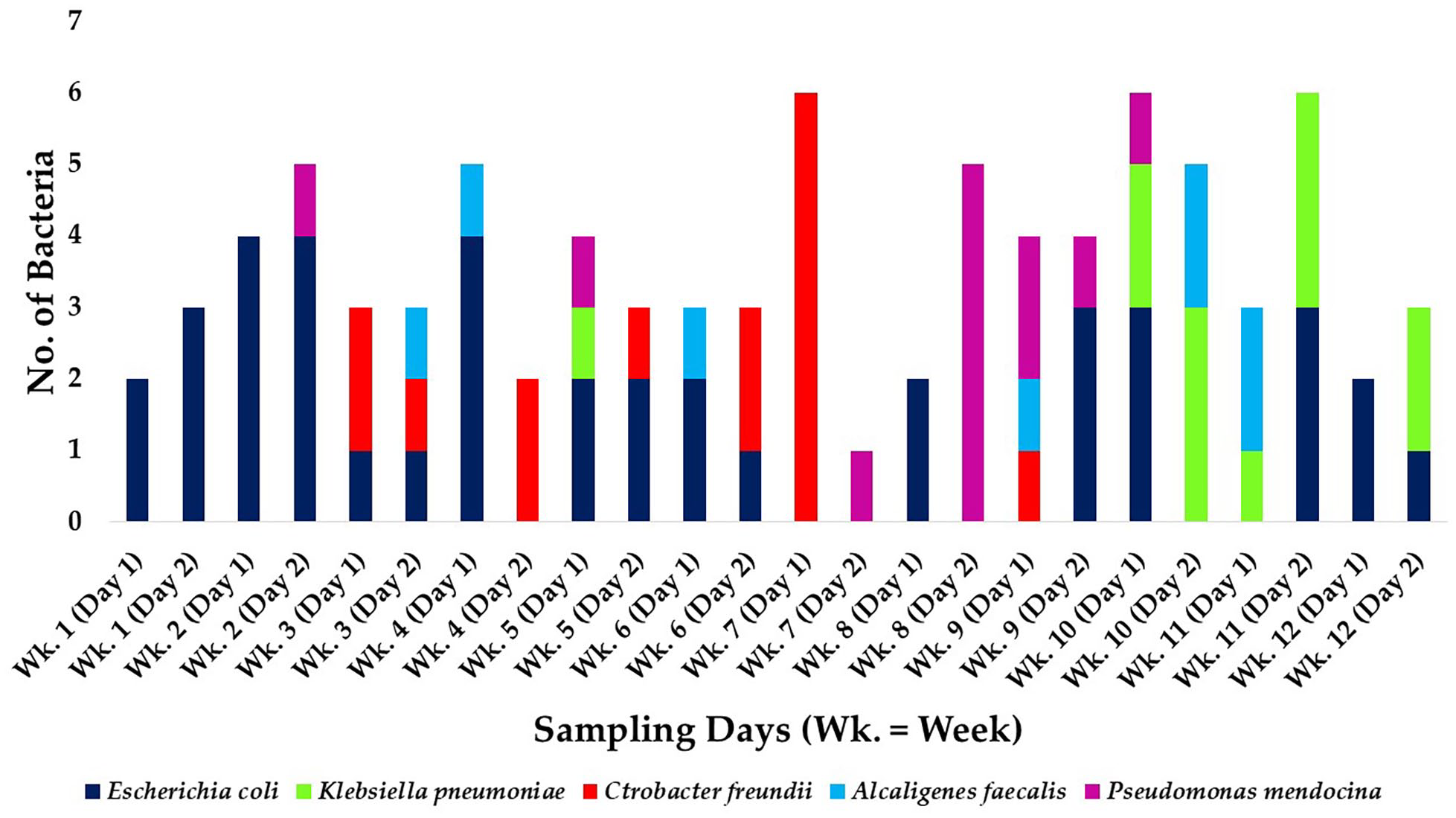
Spatio-temporal distribution of the predominant bacteria recovered from hospital wastewater collected from the Maternity Unit.
The other hospital wastewater-contained organisms that recorded a high prevalence—Klebsiella pneumoniae, Citrobacter freundii, Alcaligenes faecalis, and Pseudomonas mendocina—occurred sporadically during the sampling period. Citrobacter freundii was additionally present from Weeks 3 through to 6, and Klebsiella pneumoniae, Weeks 10 to 12, on the second days of sampling.
Similar to the case of the wastewater samples collected from the Maternity Unit, in the wastewater collected from the Child Health Unit, Escherichia coli was observed to have persisted, particularly, during Weeks 1 to 4 and 6 to 11 of the first days of sampling and Weeks 3 to 7 and 9 and 10 of the second days of sampling (Figure 2). Similarly, the occurrence of each of the other organisms was intermittent, with Klebsiella pneumoniae additionally occurring repeatedly during Weeks 2 to 4 of the second days of sampling.
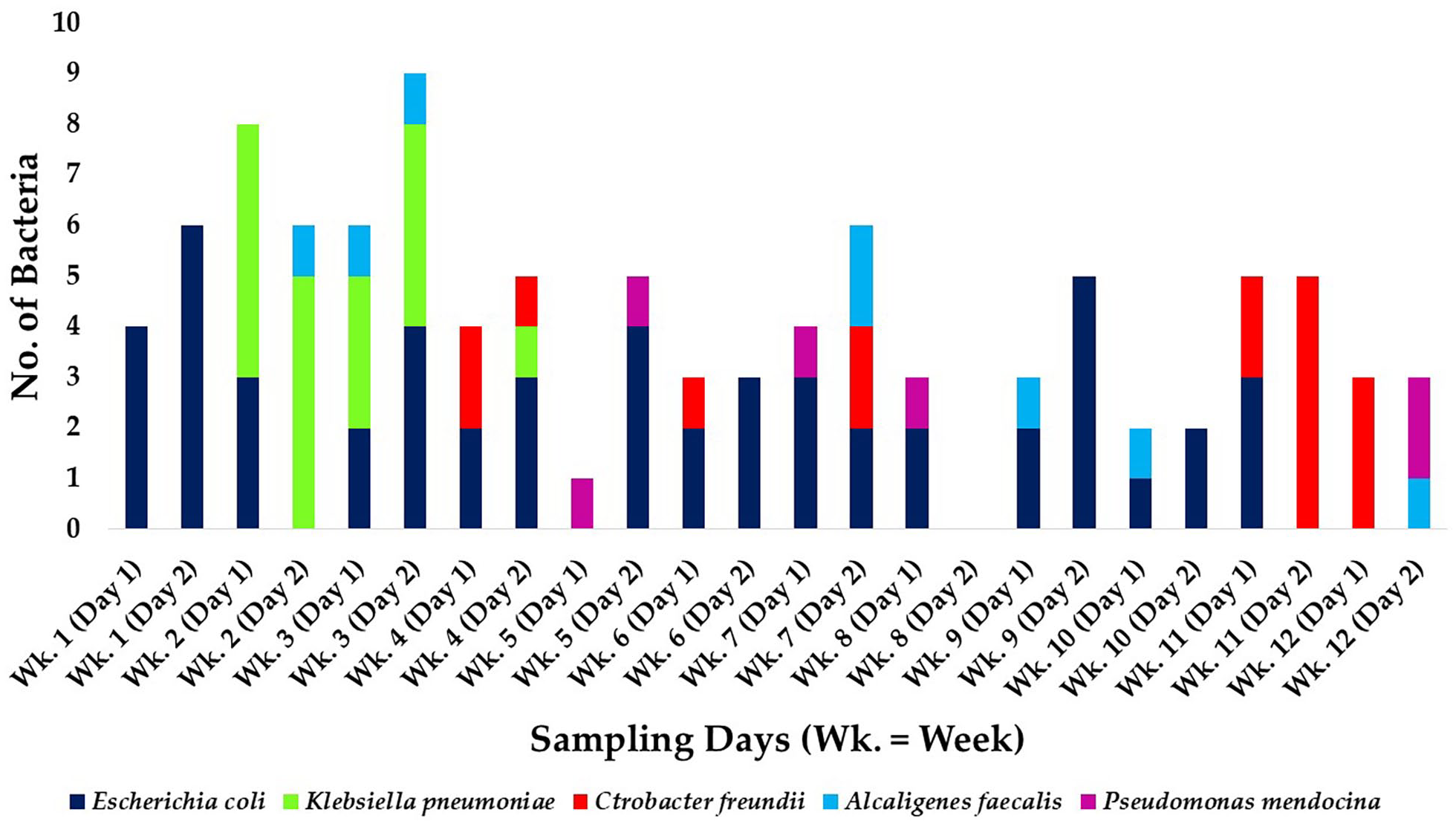
Spatio-temporal distribution of the predominant bacteria recovered from hospital wastewater collected from the Child Health Unit.
Prevalence of multidrug resistance among the hospital wastewater isolates
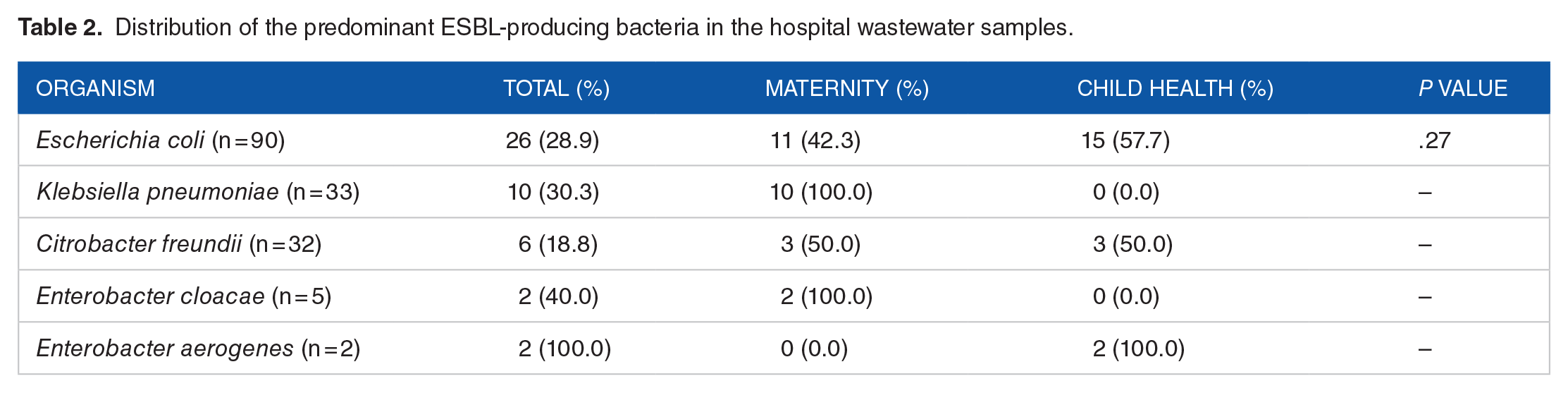
The prevalence of multidrug resistance among the hospital wastewater isolates was 55.4% (n = 163) [Maternity Unit = 53.4%, n = 87; Child Health Unit = 46.6%, n = 76, p = .22]. Moreover, the prevalence of ESBL producers among the hospital wastewater isolates was 15.6% (n = 46) [Maternity Unit = 18.4%, n = 26; Child Health Unit = 13.1%, n = 20, p = .21]. E. coli accounted for the highest proportion of ESBL-producing organisms (28.9%, n = 26). The distribution of the predominant ESBL-producing bacteria is presented in Table 2.
Distribution of the predominant ESBL-producing bacteria in the hospital wastewater samples.
Antimicrobial resistance among the hospital wastewater bacteria
All the Escherichia coli isolates recovered were resistant to trimethoprim-sulfamethoxazole and ampicillin, but not gentamicin, amikacin, imipenem, and ertapenem, and the resistance rates recorded for amoxicillin-clavulanate, cefuroxime, ceftriaxone, ceftazidime, and cefepime ranged between 24% and 30%. Klebsiella pneumoniae resistance rates against amoxicillin-clavulanate, cefuroxime, ceftazidime, and cefepime ranged between 10% and 67%. Also, Citrobacter freundii resistance rates against cefuroxime, ceftazidime, and cefepime ranged between 20% and 30%. In addition, all the Alcaligenes faecalis isolates recovered were resistant to ampicillin and amoxicillin-clavulanate, but showed no resistance to the other antibiotics tested. Moreover, all the Pseudomonas mendocina isolates were resistant to trimethoprim-sulfamethoxazole, ampicillin, ceftriaxone, ciprofloxacin, imipenem, and ertapenem. Details of the antimicrobial resistance patterns of the predominant bacteria are presented in Table 3.
Antmicrobial resistance patterns of the wastewater bacteria.
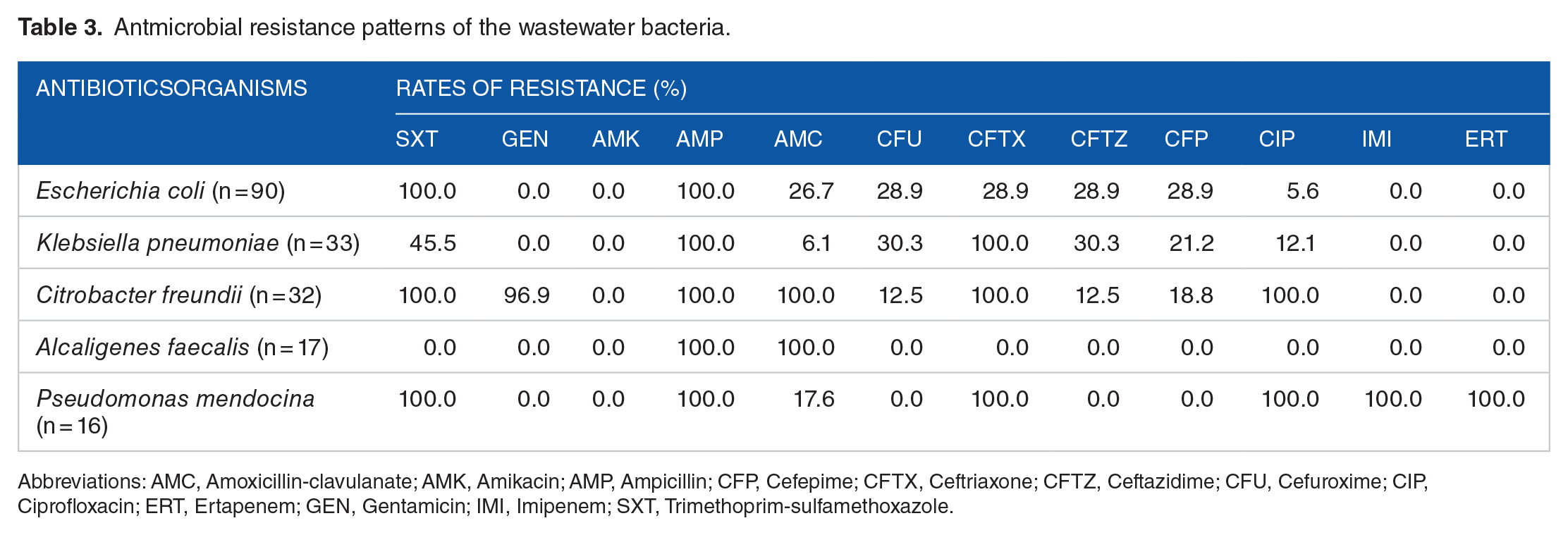
Abbreviations: AMC, Amoxicillin-clavulanate; AMK, Amikacin; AMP, Ampicillin; CFP, Cefepime; CFTX, Ceftriaxone; CFTZ, Ceftazidime; CFU, Cefuroxime; CIP, Ciprofloxacin; ERT, Ertapenem; GEN, Gentamicin; IMI, Imipenem; SXT, Trimethoprim-sulfamethoxazole.
Discussion
This study evaluated the occurrence of multidrug-resistant bacteria in hospital wastewater of the Korle Bu Teaching Hospital. One aspect of this study investigated the prevalence and types of bacteria isolated from the Korle Bu Teaching Hospital wastewater. The bacterial organisms present in the hospital wastewater sampled from both the Maternity and the Child Health Units comprised 23 different species of Gram negatives, with the predominant ones being Escherichia coli, Klebsiella pneumoniae, Citrobacter freundii, Alcaligenes faecalis, and Pseudomonas mendocina.
The range of bacteria recovered from the wastewater emanating from the 2 KBTH units could be a reflection of the bacterial infections managed at the units during the study period, and compares well with many of the hospital wastewater evaluation studies conducted previously. For instance, Daoud et al. 33 who conducted their study in a hospital in Lebanon reported the range of organisms they found to be E. coli, Enterobacter cloacae, and K. pneumoniae (all of which were isolated in the current study), as well as Klebsiella oxytoca and Serratia odorifera (which were not isolated in the current study). Le et al. 44 also reported Acinetobacter junii, Comamonas testosteroni, Enterobacter spp., and Pseudomonas spp. as the organisms they recovered from the wastewater of a hospital in Singapore. Although these 5 organisms were also isolated in the current study, none of the 18 other bacterial species isolated in the current study were recovered in the study of Le et al. 44 Similarly, Anssour et al. 29 recovered E. coli, K. pneumoniae, and Citrobacter freundii (all of which were isolated in the current study), as well as Klebsiella oxytoca, Escherichia vulneris, and Citrobacter koseri/farmer (which were not isolated in the current study) from the wastewater of an Algerian hospital. Likewise, Moges et al. 27 also recovered 13 different types of bacterial species—E. coli, Enterobacter spp., Pseudomonas spp., Citrobacter spp., K. pneumoniae, Klebsiella oxytoca, Klebsiella ozaenae, Shigella spp., S. aureus, Providencia spp., Edwardsiella spp., Serratia spp., and Morganella spp., from the wastewater of Gondar University Hospital in Ethiopia. Only the first 5 of the bacteria listed, however, overlapped with those isolated from the current study. The findings of these studies, along with those of the current study, confirm that hospital wastewater is an important reservoir of a wide variety of potentially pathogenic bacteria. Accordingly, individuals who rely on water bodies contaminated with hospital wastewater for domestic use, without appropriate prior treatment, may put themselves at risk of a wide range of microbial infections.
The subtle disparities between the range of organisms reported in the current study and those of the other studies highlighted could be accounted for by differences in the bacterial identification methods employed. Most of these other studies used manual methods of bacterial identification, compared to the MALDI-TOF technique used in the current study which is more specific, and hence would identify a wider range of organisms following their isolation. 45 Also plausible is the potential role that differences in the content and brands of agar used may have played in the growth of the target bacteria.46 -48
Moreover, in the current study, 5 bacterial species dominated in both units, with Escherichia coli being the frequently isolated organism, at a prevalence of 30.6%, followed by Klebsiella pneumoniae (11.2%), Citrobacter freudii (10.9%), Alcaligenes faecalis (5.8%), and Pseudomonas mendocina (5.4%). Similar to these findings, Daoud et al., 33 in a study on Lebanese hospital wastewater, isolated Escherichia coli as the predominant organism (accounting for 56.3% of the isolated bacteria). Anssour et al. 29 likewise recovered Escherichia coli as the predominant bacteria, with a prevalence of 85%, alongside Klebsiella pneumoniae (6.7%) and Citrobacter freundii (3.3%) from hospital wastewater in Algeria. Again, Sakkas et al. 13 also recorded Escherichia coli and Klebsiella pneumoniae as the predominant bacteria with a prevalence of 34.1% each, followed by Pseudomonas spp. (12.8%). Contrarily, Moges et al. 27 recorded Klebsiella pneumoniae as the frequently isolated organism accounting for 23.5%, followed by Pseudomonas spp. (16.8%), Escherichia coli (11.5%), and Citrobacter spp. (11.5%). Asfaw et al., 30 in a study on antibiotic resistant bacteria in a North Ethiopia hospital wastewater, also isolated Klebsiella pneumoniae, Escherichia coli, and Citrobacter freundii, with prevalence of 17.9%, 12.7%, and 6.7%, respectively.
One other key objective of this study was to determine the spatio-temporal distribution of the hospital wastewater-contained bacteria. This study is one of the few in sub-Saharan Africa to go beyond determining the prevalence of different bacteria in hospital wastewater to use a design that allows for gaining insights into the dynamics in bacterial composition of hospital wastewater effluents overtime. As observed, Escherichia coli persisted for several of the weeks in the wastewater from the 2 critical care units. Some of these E. coli isolates may not necessarily have originated from the critical care units studied, as it is conceivable that the wastewater system may host environmental E. coli contaminants. While it is difficult to explain the intermittent absence of E. coli, changes in environmental conditions within the wastewater system, the wastewater system configuration, such as biofilms, and other environmental factors may have played a role in the E. coli transiency. As E. coli is a known indicator of fecal contamination, its persistence during those periods could also have been influenced by shedding of the organism by patients and hospital staff alike into the lavatory wastewater of the 2 KBTH units during those periods. 49 Possibly, too, it could reflect a prevalence of E. coli-associated diarrhea, E. coli UTI, some other E. coli infections like neonatal meningitis, cholangitis, or pneumonia, or a mixture thereof, during those weeks at the units studied. In like manner, the sporadic occurrence of the other organisms could be a reflection of sporadic cases of infection involving those bacteria at the units during the specified periods. The absence of a distinction between facultative and obligate pathogenic E. coli, however, minimizes the conclusiveness of this infection hypothesis. Future studies on microbiological evaluation of hospital wastewater could include an investigation of cases managed at the units of the hospitals from which the effluents emanate to add to the robustness of the data generated.
This study additionally investigated the prevalence of multidrug resistance among the hospital wastewater isolates that were recovered. The prevalence of multidrug resistance among the hospital wastewater isolates was 55.4%, and that of ESBL producers was 15.6%, with the organisms generally demonstrating high resistance rates. The high antibiotic resistance rates, including multidrug resistance, is consistent with the high rates reported by various studies among clinical isolates emanating from the study hospital.16,18,23,24,50 -52 Several studies have also reported high prevalence of multidrug resistant bacteria in hospital wastewater. For example, Voigt et al. 53 found between 85.7% and 96.4% of hospital wastewater they sampled from different sites to contain ESBL E. coli, Citrobacter spp., Enterobacter spp., and Klebsiella spp. That in the current study, organisms with the identified resistance traits were recovered from the wastewater effluent of a leading referral hospital in the country is worrying, as the wastewater effluents could potentially end up in water bodies used in community settings. Previous studies have demonstrated a high potential for transmission of multidrug resistant organisms from such contaminated water bodies to humans, such as those involving IMI2-producing Enterobacterales and KPC3-producing K. pneumoniae in south of France and Frankfurt, Germany, respectively.54,55 Consequently, the pool of hospital wastewater evaluated in this study, and by extension, those generated in the hospital, could serve as a reservoir for dissemination of drug-resistant infections. In fact, previous studies in the country have demonstrated that fomites, as well as cockroaches, are important in harboring and disseminating multidrug resistant organisms and drug resistance determinants.18,56,57
The public health concerns raised by the findings of the current study may be accentuated by the fact that besides potentially providing a snapshot of the nature of the wastewater generated by other hospitals in the country, the hospital studied is a major referral healthcare facility, and by virtue of this status, may have more robust waste management strategies than would lower-tier hospitals in the country. It is also possible that the findings of the current study may be a reflection of the complexity of cases handled at the hospital, and not necessarily be a general reflection of the wastewater of the entire healthcare system of the country. To clarify this hypothesis and adequately quantify the aforementioned public health threat, it would be necessary to replicate this study at other hospitals in the country which belong to other tiers of healthcare classification, as well as in community settings. As an additional public health measure to safeguard antimicrobials, it is important that hospitals in the country routinely monitor the microbiological safety of their wastewater effluents and disinfect them. These monitorings could encompass evaluation of prevalence and types of antibiotic residues. Moreover, as noted earlier, the high rates of resistance recorded highlight the need to intensify antimicrobial stewardship efforts to help tackle the antimicrobial resistance menace efficiently.
One limitation this study has is that it was conducted in only one hospital, and focused on only 2 units of the hospital, and hence the results may not be representative of all the departments in the hospital or all the hospitals in the country. A study of the presence of antibiotic residue in the waste water and the pattern of microbial resistance in human specimens form these units would have provided further insights. Also, the source of contamination could have been exogenous.
Conclusion
The wastewater generated by the Maternity and Child Health Units of KBTH harbored a wide range of multidrug resistant bacteria, with a good proportion of these being ESBL producers, and the predominant and persistent one being E. coli. The study, thus, identifies the wastewater of KBTH as an important source of multidrug resistant organisms, and underscores the significance of appropriate treatment of wastewater of the hospital and other clinical and related settings prior to its discharge.
Findings from this study, particularly, the high prevalence of multidrug resistance, suggest that studies of this nature should be done routinely and expanded to other hospitals in the country. Also, education on the local treatment of water like boiling before usage is important, as this is likely to reduce the adverse effects these contaminated treated effluents have on inhabitants in the environment. Extensive research is to be conducted to identify efficient and cost-effective ways to remove antibiotic resistant organisms from hospital effluents. Again, hospitals should be built to include waste treatment plants, and the effectiveness and functioning of these plants should be regulated by the authorized bodies. In fact, it is recommended that wastewater from hospital settings is pre-treated, even prior to arrival in local treatment plants. 58
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization: ESD, FCNK, and NTKDD. Design: FCNK, ESD, EMAT, and NTKDD. Sampling: DSA-N and M-MO. Validation: NTKDD, FCNK, ESD, M-MO, and PD. Data curation: FCNK, DSA-N, and NTKDD. Formal analysis: FCNK, NTKDD, EMAT, and DSA-N. Investigation: DSA-N, M-MO, FCNK, NTKDD, and ESD. Resources: NTKDD, ESD, FCNK, DSA-N, PD, and M-MO. Visualization: FCNK, DSA-N, EMAT, and ESD. Software: FCNK and DSA-N. Supervision: NTKDD, ESD, and PD. Project administration: NTKDD, ESD, DSA-N, and FCNK. Writing—original draft preparation: FCNK, DSA-N, NTKDD, EMAT, and ESD. Writing—review and editing: FCNK, NTKDD, DSA-N, PD, EMAT, M-MO, and ESD. All authors have read and approved the final version of the manuscript.