
Abstract
Objectives
The aim of the study was to evaluate the biomechanical properties of the combination of circumferential and Krackow sutures using FiberWire compared with the conventional methods in feline transverse patellar fractures.
Methods
A total of 24 feline cadaveric pelvic limbs (mean body weight 3.74 kg) were harvested, and the patella of each limb was osteotomised transversely to simulate a fracture. The limbs were then randomly assigned to 1/3 stabilisation methods (n = 8 per group): group 1 (PFW) was stabilised with a modified tension band wire with a 0.9 mm Kirschner wire and No 2 FiberWire; group 2 (CFS) was stabilised with a circumferential and figure-of-eight suture with No 2 FiberWire; and group 3 (CKS) was stabilised with a circumferential and Krackow suture with No 2 FiberWire. All knee joints were fixed at a 135° neutral standing angle and tested by applying tensile force. Loads at 1, 2 and 3 mm gap formation, the maximum failure load and failure modes were recorded.
Results
At 1 mm displacement, group 3 (mean tension 96.1 ± 18.6 N) was significantly stronger than group 1 (P <0.017). At 2 mm and 3 mm displacements, group 3 (mean tension 162.4 ± 12.2 N and 238.6 ± 25.4 N) was significantly stronger than both groups 1 and 2 (P <0.017). The maximum failure load of group 3 (mean tension 352.3 ± 31.0 N) was significantly higher than groups 1 and 2 (P <0.017). The primary failure mode was pin pull-out (group 1), suture pull-out (group 2) and tendon rupture (group 3).
Conclusions and relevance
The combination of circumferential and Krackow suture technique provides greater resistance to fragment displacement and construct failure than conventional methods in this ex vivo feline patella fracture model.
Introduction
Patellar fractures in cats are a relatively infrequent, but increasingly documented, clinical problem. Although patellar fractures are reported to constitute approximately 1% of all skeletal injuries in humans and up to 0.1% of all bone fractures in dogs, the true prevalence of this condition in cats remains poorly defined. 1 However, to date, clinical surveys and reviews have characterised the condition, while various biomechanical studies have investigated strategies for surgical repair.2 –5 Unlike in dogs, where fractures are often linked to direct trauma or complications from procedures like tibial plateau-levelling osteotomies, patellar fractures in cats are frequently pathological in nature. 6 This pathology is strongly linked to patellar fracture and dental anomaly syndrome (PADS), a condition characterised by non-traumatic, bilateral and transverse stress fractures.2,7 The patella’s function as a lever arm for the stifle extensor mechanism is critical.8,9 Therefore, any surgical repair must be robust enough to neutralise the significant distractive forces generated by the quadriceps mechanism to restore proper hindlimb function.
The pin and tension band wire (PTBW) method has been the predominant surgical technique for treating patellar fractures. 2 However, this technique is associated with high complication rates in cats, reported as high as 64–86%, including pin migration, soft tissue irritation and construct failure.2,10 Furthermore, in cases where the fracture is presumed to be associated with PADS, the PTBW technique is considered largely contraindicated, given the substantial risk of iatrogenic fractures and subsequent postoperative implant failure. 2 In addition, many repair techniques documented in humans are not possible in cats because of the small size of the patella. These limitations have spurred investigations into alternative repair strategies for the fixation of feline patellar fractures. An initial study established that among several wire-based constructs, a combined circumferential and figure-of-eight wire was biomechanically superior to the conventional PTBW method. 4 A more recent biomechanical study in feline patellar fracture models highlighted the potential of suture-only repairs, concluding that a combination of circumferential and figure-of-eight sutures was significantly more resistant to displacement than the previously described wire construct. 5
As such, the exploration of alternative soft tissue repairs continues. The Krackow suture is a well-established technique widely utilised in human orthopaedics for major tendon and ligament reconstruction, such as the Achilles, patellar ligament and quadriceps tendon.11,12 The utility of the Krackow suture in veterinary medicine has been demonstrated by clinical applications and biomechanical studies.13 –16 The biomechanical principle relies on a series of locking loops designed to grasp the longitudinal fibres of the tissue, which then tighten and stabilise their hold as the construct is placed under tension.2,17 In human medicine, biomechanical and clinical evaluations of the Krackow suture technique for patellar fracture repair have already been reported.18,19
Thus, the aim of this study was to evaluate the biomechanical properties of a novel combination of circumferential and Krackow sutures (CKS), compared with pin and tension band suture technique using FiberWire (PFW) and the combination of circumferential and figure-of-eight sutures (CFS).
Materials and methods
Specimen preparation
A total of 24 pelvic limbs from 12 adult cats were collected and utilised, all of which had been euthanased or died for reasons unrelated to hindlimb orthopaedic pathologies. The mean body weight of the cadavers was 3.76 kg (range 2.0–5.4). All cadavers were frozen at –70°C and subsequently thawed at room temperature for sample collection. The muscles, except for the quadriceps muscles, were excised from the femur, and then the quadriceps muscles were separated from the femur. The quadriceps muscles were trimmed to remove the muscle mass, leaving only the tendon and fascia. The femur was osteotomised at the level immediately proximal to the patellar groove. The patella was osteotomised transversely in the middle with an osteotome and mallet; this is where transverse fractures are known to occur most often. 20 The samples were wrapped in gauze soaked with 0.9% saline solution and frozen at –70°C.21 –23 Before mechanical testing, the frozen specimens were thawed to room temperature over 24 h.
Group 1: pin and FiberWire
A pin and FiberWire (PFW) technique was applied to group 1 (Figure 1a). After reduction of the bone fragments, a single 0.9 mm Kirschner wire (K-wire) (Top Medical) was drilled in a normograde manner. A figure-of-eight tension band suture was then applied using a single strand of No 2 FiberWire (Arthrex). This suture was passed behind the proximal and distal ends of the K-wire and subsequently tightened and secured with a surgeon’s knot. The K-wire size was selected based on previous biomechanical studies and a clinical report.2,4,5
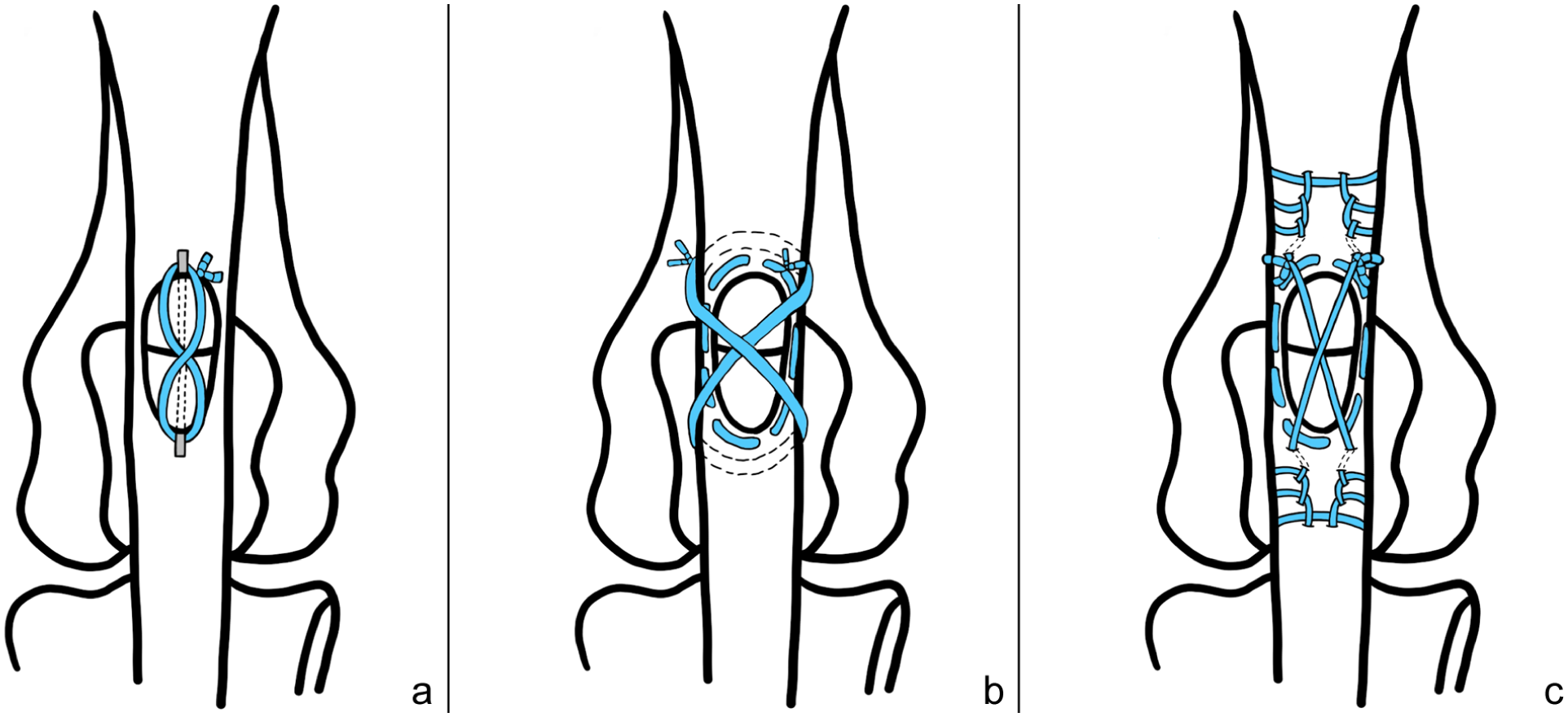
Illustrations of three fixation methods for transverse patellar fracture models. (a) Group 1 (pin and FiberWire [PFW]), (b) group 2 (combination of circumferential and figure-of-eight sutures [CFS]) and (c) group 3 (combination of circumferential and Krackow sutures [CKS])
Group 2: combination of circumferential and figure-of-eight sutures
A combination of circumferential and figure-of-eight sutures (CFS) was applied to group 2 (Figure 1b). After reduction of the bone fragments, a circumferential purse-string suture was placed around the patella using No 2 FiberWire with a tapered needle. The suture was tightened with a surgeon’s knot followed by a square knot (four throws in total), while maintaining consistent tension. Subsequently, a second suture was passed through the proximal and distal tendons, deep to the initial circumferential suture, in a figure-of-eight pattern. This suture was secured in an identical manner. All knots were positioned at the proximal aspect of the patella. The size of implant was selected based on a previous biomechanical study. 5
Group 3: combination of circumferential and Krackow sutures
A combination of circumferential and Krackow sutures (CKS) was applied to group 3 (Figure 1c). A circumferential suture was initially applied in the same manner as in group 2. Subsequently, a Krackow suture was applied to both the proximal and distal segments using independent strands of No 2 FiberWire with a tapered needle. For each segment, the suture was initiated adjacent to the fracture line and progressed away from the fracture line through three locking passes, placed at intervals of 2.5 mm along one border (medial or lateral) of the quadriceps tendon for the proximal fragment and the patellar ligament for the distal fragment. The suture then returned towards the fracture line via three locking passes along the opposite border. The resulting four free ends were then crossed cranially over the patellar surface and secured with a surgeon’s knot.
Biomechanical test
All limbs were fixed laterally to a wooden plate, positioning the stifle joint at its normal standing angle of 135°. This wooden plate was mounted onto the lower tensile grip of the universal testing machine (ISG Minos-100S; MTDI). The quadriceps tendon was wrapped in gauze and then gripped by the upper side tensile grip (Figure 2). A tensile force with a crosshead speed of 10 mm/min was applied. Simultaneously, a ruler was positioned adjacent to the patella. Two synchronised cameras were utilised for data recording: one recorded the fracture gap changes and the second recorded the load-displacement curve displayed on the monitor. The recorded videos were analysed post hoc to determine the loads corresponding to displacements of 1, 2 and 3 mm. Failure was defined as the point at which the recorded load exhibited an abrupt decrease, and the specific modes of failure for each sample were documented. Raw data were extracted to identify the maximum failure load for every sample.

A photograph of the biomechanical tensile testing on a repaired patellar fracture model. Both the distal femur and the proximal tibia were fixed to a wooden plate. A tensile force was applied to the quadriceps tendon using the universal testing machine to simulate the pull of the extensor mechanism
Statistical analysis
SPSS version 31.0.0.0 (IBM) was utilised for statistical analysis. As a result of the small sample size in each group, the Kruskal–Wallis test was used to evaluate the statistical significance between the groups. P <0.05 was considered statistically significant. If there was significance among the groups, the significant differences noted between the groups were determined with a Mann–Whitney test with Bonferroni correction. In this test, P <0.017 was considered significant.
Results
Loads at displacements of 1, 2 and 3 mm
At 1 mm displacement, a significant difference was observed between groups 1 and 3 (P <0.017), whereas groups 1 and 2, and groups 2 and 3 were not statistically different (Table 1, Figure 3).
Loads at 1, 2 and 3 mm displacement of repaired patellar fracture models under tensile force during the biomechanical testing

Data are median (interquartile range/2).a,b Values with different superscript letters are significantly (P <0.017) different. Group 1: pin and FiberWire; group 2: combination of circumferential and figure-of-eight sutures; group 3: combination of circumferential and Krackow sutures

Box and whisker plots of loads at 1, 2 and 3 mm displacement. Groups sharing the same letter indicate no statistically significant difference between them. At 1 mm displacement, there was a significant difference between groups 1 and 3 (P <0.017). At 2 and 3 mm displacement, there were significant differences between groups 1 and 3, as well as between groups 2 and 3 (P <0.017). Group 1: pin and FiberWire; group 2: combination of circumferential and figure-of-eight sutures; group 3: combination of circumferential and Krackow sutures. N = Newton
At 2 mm displacement, a significant difference was observed between groups 1 and 3, as well as between groups 2 and 3 (P <0.017), whereas groups 1 and 2 were not statistically different (Table 1, Figure 3).
At 3 mm displacement, a significant difference was observed between groups 1 and 3, as well as between groups 2 and 3 (P <0.017), whereas groups 1 and 2 were not statistically different (Table 1, Figure 3).
Maximum failure load
Significant differences were observed between groups 1 and 3, as well as between groups 2 and 3 (P <0.017), whereas groups 1 and 2 were not statistically different (Table 2, Figure 4).
Load at maximum failure point of repaired patellar fracture models under tensile force during biomechanical testing

Data are median (interquartile range/2). Values with different superscript letters are significantly (P <0.017) different. Group 1: pin and FiberWire; group 2: combination of circumferential and figure-of-eight sutures; group 3: combination of circumferential and Krackow sutures

Box and whisker plots of maximum failure load. Groups sharing the same letter indicate no statistically significant difference between them. There were significant differences between groups 1 and 3, as well as between groups 2 and 3 (P <0.017) at maximum failure load. Group 1: pin and FiberWire; group 2: combination of circumferential and figure-of-eight sutures; group 3: combination of circumferential and Krackow sutures. N = Newton
Modes of failure
The modes of failure differed between groups (Table 3). In group 1, failure consistently occurred via pin pull-out in all eight samples. In group 2, the most frequent failure type was the suture pulled out from the tendon at the suture–tendon interface (n = 6), followed by tendon rupture (n = 2). In group 3, all eight samples failed exclusively because of tendon rupture. This rupture occurred at the tendon mid-substance, distinct from the implant or suture fixation sites.
Modes of failure in repaired patellar fracture models under tensile force during the biomechanical testing

Group 1: pin and FiberWire; group 2: combination of circumferential and figure-of-eight sutures; group 3: combination of circumferential and Krackow sutures
Discussion
The results of this study suggest that the CKS method exhibits greater resistance to displacement than the CFS method in this ex vivo feline transverse patellar fracture model. In both the CKS and CFS methods, a circumferential suture was employed to facilitate initial anatomic apposition and to provide hoop strength against rotational or shear stresses through a purse-string-like mechanism. The application of the Krackow suture for feline patellar fracture repair in this study was inspired by the fact that it can be used for quadriceps and patellar ligament repairs. The patella, having the characteristics of a sesamoid bone, shares the common goal of gap prevention with other tendon repairs. 18 Although the circumferential suture provides a baseline for structural alignment, the Krackow suture places suture anchors in the robust supporting structures proximal and distal to the patella – namely, the tendons – instead of directly fixing to the bone. This provides stable support to the fractured patellar fragments, resists longitudinal gap formation and enhances overall fixation strength. Indeed, the application of the Krackow suture for patellar fracture repair has already demonstrated clinical efficacy in human medicine. 19
The greatest clinical significance of this bone-sparing approach is its applicability to cases with poor bone quality, and feline PADS corresponds precisely to this pathological condition. PADS is characterised by fatigue fractures from repetitive jumping stress and presents radiographically as sclerotic but possesses extremely fragile bone quality.3,17 The traditional PTBW method of inserting a K-wire into the patella of cats with PADS is technically very difficult, carries a high risk of iatrogenic fracture and has a reported clinical complication (refracture or fixation failure) rate as high as 86%.2,3 A study by Magister and Yarboro 18 in human medicine also suggested that Krackow augmentation for patellar fractures may be most useful in the setting of poor bone quality where conventional repair techniques are limited. The CKS method, by anchoring directly to the tendon itself, not the bone, fundamentally circumvents the inherent failure risk of pin-based fixation. Therefore, the CKS method is not only applicable for cases where low bone density (such as in PADS) makes metallic fixation difficult, but it can also be a viable surgical alternative when the bone is extremely small, or in cases of longitudinal or comminuted fractures where pin insertion is not feasible.
A comparison of the experimental results for the CFS group with those reported by Lee et al 5 revealed slight differences in experimental values, despite using the same fixation method and materials. This discrepancy is likely attributable to experimental variables that are difficult to control in ex vivo studies rather than inherent differences in construct strength. Variations in initial tension during knot tying, or the degree of knot settling and suture creep occurring during the initial loading phase, can influence the measurement of initial stiffness.24 –26 Furthermore, biological variability among cadaveric samples, particularly differences in tendon tissue properties, may also have affected the results. It is also noteworthy that no statistically significant difference was observed between the PFW group and the CFS group, in terms of load at 1, 2 and 3 mm displacement and maximum failure load. This contrasts with the findings of Lee et al. 5 This difference can be interpreted as resulting from the variation in tension band materials. The findings are consistent with those from Park et al 27 in canine models, where the FiberWire tension band group demonstrated consistently higher mean loads at displacements of 1, 2 and 3 mm and maximum failure load compared with the orthopaedic wire group. Therefore, using FiberWire in the PFW group may have provided a stronger tension band than orthopaedic wire.
In the 1, 2 and 3 mm displacement measurement, the CKS group demonstrated significantly greater strength to displacement resistance than the PFW group. It also demonstrated significantly greater strength to displacement resistance than the CFS group at 2 and 3 mm. Although studies in humans have suggested that a displacement of 2–3 mm or a shift of 1–4 mm indicates the need for surgical correction, such guidelines have not been established for cats. 28 The patella, as a sesamoid bone, primarily undergoes fibrous union rather than osseous union in the majority of feline patellar fractures. Based on this biological healing characteristic, the surgical goal for feline patellar fractures should focus on restoring the quadriceps mechanism and maintaining close apposition of the fragments, rather than achieving complete osseous union.2,3,10,29,30
Accordingly, previous studies have defined the failure of stabilisation as 3 mm of displacement, and the same criterion was applied in this study.4,5,30 According to biomechanical studies on humans, the joint reaction force applied to the knee during walking is estimated to be approximately 2–3 times body weight. 31 In cats, the peak vertical force applied to the hindlimbs during walking is approximately 38% of body weight, and upon landing after a jump from a height of 1 m, it is reported to be approximately 141% of body weight.32,33 Based on the average body weight in this study, this translates to an estimated load of approximately 13.8 N during walking and approximately 51.1 N upon landing after a jump. At these physiological load levels, none of the specimens in this study showed displacement during walking. According to the results in Table 1, only the PFW group showed a potential for micro displacement at approximately 1 mm. This suggests that both the CFS and CKS groups can maintain sufficient strength under initial weightbearing conditions. Furthermore, the CKS group showed significantly higher values at maximum failure load compared with the other two groups, demonstrating superior results not only in simple initial displacement resistance but also in overall structural strength. These characteristics suggest that the CKS method has the potential to maintain stability even under relatively larger load conditions. Therefore, it can provide stable fixation not only for cats of average weight but also for large breed cats like Maine Coons or obese individuals where the tensile force from the quadriceps is relatively high. Moreover, it can be evaluated as a potentially applicable technique for larger feline species with similar anatomical structures of the quadriceps mechanism.
Distinct differences in failure modes were observed among the groups (Table 3). In the PFW group, all samples failed because of pin pull-out. Although the intentional omission of bending the inserted K-wire ends to avoid clinical concerns, such as iatrogenic fragmentation, may have influenced the results, this clearly demonstrates that the pin–bone interface itself is an inherent structural vulnerability in feline patellar fracture repair. This finding supports the fundamental limitation of conventional pin fixation methods in the small and often fragile feline patella. The CFS group failed via suture pull-out from the tendon in six samples, suggesting that the figure-of-eight suture created a stress concentration at the suture–tendon interface, leading to the suture cutting through the tissue before the tendon itself ruptured. In contrast, all samples in the CKS group failed because of tendon rupture of the quadriceps muscle, independent of the construct site. This indicates that the construct provided a fixation strength exceeding the biomechanical threshold of the tendon itself, which is considered the ideal failure mode in repair. 34 The core principle of the Krackow suture is that its locking loops distribute forces evenly over a larger area of the tendon, thereby preventing stress concentration and effectively resisting suture pull-out at the suture–tendon interface.11,35
This study has several limitations. First, the small sample size may weaken the statistical power. Second, the biomechanical evaluation was limited to a tensile test at a fixed angle and did not incorporate repetitive cyclic loading. Future cyclic loading tests are essential to evaluate the long-term durability and resistance to gap formation of each fixation method. Third, as this was an ex vivo study using frozen-thawed cadavers, the material properties may not fully replicate those of in vivo tissue, and biological variability among samples may also have influenced the results. Fourth, the intervals of the Krackow suture were determined by referencing established parameters from canine tenorrhaphy literature because of the lack of species-specific biomechanical data in cats for the quadriceps or patellar tendon. The 2.5 mm spacing was adopted from the methodology described for canine gastrocnemius tendon repair.14,15 However, studies in human medicine have demonstrated that using wider intervals significantly enhances the construct’s ultimate tensile strength and resistance to gap formation. 36 Therefore, the performance reported may not represent the maximum biomechanical potential of the CKS construct, and future studies are warranted to systematically evaluate the optimal spacing in the feline model. Fifth, the use of an osteotome and mallet to create fractures may have introduced irregularities at the fracture margins, potentially leading to imperfect reduction. 37 Finally, the knot-tying method and the location of the knots were not specifically considered in this study. Although the inherent bulk of FiberWire knots constitutes a limitation of the constructs, clinically, it can be mitigated by burying the knots within surrounding soft tissues and avoiding overlapping placement. Furthermore, various knot-tying techniques tested in human medicine have been shown to possess significantly greater strength than the conventional surgeon’s knot.38,39
Nevertheless, to the best of our knowledge, there is no biomechanical comparison study to date on repair methods using the combination of circumferential and Krackow suture in feline transverse patellar fracture models. This study indicates that the CKS method offers a biomechanically superior, bone-sparing solution, particularly for compromised bone quality.
Conclusions
In conclusion, this study demonstrates that the combination of circumferential and Krackow sutures provides superior biomechanical stability in feline patellar fracture models compared with conventional methods and may serve as a viable clinical alternative, especially as a valuable technique for pathological fractures like PADS.
Footnotes
Acknowledgements
Thanks to Min-Yeong Lee, Jae-Won Do, Sang-Kun Jang, Yoo-Keong Lee, In-Ho Kim, In-Seong Jeong, JJang-A Kim, Cooper Kim and Yang-Yang Kim for all their support and contributions.
Author note
Data supporting this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.