
Abstract
Objectives
This study aimed to compare the biomechanical properties of three stabilisation techniques in feline patella transverse fractures and select the strongest method with potentially minimal complications.
Methods
Patella fracture was simulated in 27 feline cadaveric pelvic limbs (mean weight of the cadavers 3.78 kg), and the limbs were randomly grouped to be stabilised with one of the three stabilisation methods. The modified tension band wiring technique with a single Kirschner wire (0.9 mm) and figure-of-eight wiring (20 G) was applied to group 1 (n = 9). Group 2 (n = 9) was stabilised with a combination of circumferential and figure-of-eight wiring techniques with orthopaedic wire (20 G). Group 3 (n = 9) was stabilised with the same technique as group 2, but with #2 FiberWire. The knee joints were positioned and fixed in the neutral standing angle (135°) and tested by applying tensile force. The loads at gap formations of 1, 2 and 3 mm were recorded, and the maximum failure load was measured in each group.
Results
In all the loads at displacement (1, 2 and 3 mm), group 3 was significantly stronger than groups 1 and 2, respectively (P <0.017). Group 3 (261.0 ± 52.8 N) showed significantly stronger fixation in the maximum load compared with group 1 (172.9 ± 45.6 N) (P <0.017). No significant difference was observed between groups 1 and 2 (204.9 ± 68.4 N) or between groups 2 and 3.
Conclusions and relevance
This study shows that the combination of circumferential and figure-of-eight techniques with FiberWire is more resistant to displacement than metal wire in this ex vivo feline patella fracture model.
Introduction
Patella fractures infrequently occur but have increasingly been reported during the past few decades. A report has dealt with 52 fractures in 34 cats, and a clinical review of feline patella fracture has been published more recently.1,2
In humans, the incidence of patella fractures is about 1% of all skeletal injuries, and in dogs, the incidence is reported to be up to 0.1% of all bone fractures; however, in cats, limited information is available on its prevalence.3,4 Apart from humans and dogs, in cats, pathological patella fractures have been reported, related to patella fracture and dental anomaly syndrome (PADS).5,6 The aetiology of such a syndrome is unknown, but PADS must be suspected when non-traumatic or stressed unilateral or, more often, bilateral transverse patellar fracture is presented.2,5
In human medicine, surgery is indicated when displacement is >1–4 mm, but there is no consensus on the indications for surgical intervention in feline medicine. 7 A retrospective study showed good clinical results with conservative treatment in feline transverse patella fractures; however, it provides weak evidence, dealing with only three cases. 8 When surgically treated, patella fractures have predominantly been treated with a pin and tension band wire (PTBW) method. 2 However, in cats, such treatment has been reported to have notoriously high complication rates (64–86%).2,9 Particularly when the fracture is suspected to be related to PADS, PTBW repair is almost contraindicated due to the high risk of additional fracture and postoperative implant failure. 2 Therefore, a few attempts to find an alternative method to fix patella fractures in cats have been made. A recent biomechanical study reported that the circumferential wiring combined with figure-of-eight wiring (CFEW) method has the strongest properties over the single circumferential wiring, single figure-of-eight wiring, and modified PTBW techniques. 10
Similarly, in human medicine, when using wires to repair patella fractures, complications related to hardware discomfort and infection occur, in which up to 60% of the patients required removal of the wires or experienced implant failure.11–14 Therefore, in humans, various novel fixation methods have been introduced, including numerous modifications in tension band wiring methods, cerclage wiring, tension band sutures, screw fixation, cannulated screws with sutures, and plate and screw fixation.7,14 A clinical comparison of steel wire with braided polyester sutures using a tension band technique has been made in human transverse patella fractures, and the reoperation rate was 6% in the braided polyester group, due to fracture displacement, while that of the steel wire group was 38%, mostly due to hardware discomfort and infection. 15 In dogs, a biomechanical study introduced the use of a locking plate and screws in fixation of a patella fracture and reported it to be more stable than tension band wiring, and a recent clinical case report in which such a method was applied showed a successful outcome.16,17 However, due to the small size of the patella in cats, screw placement is almost impossible, and in a feline-specific pathological condition such as PADS, drilling into the patella can cause disastrous results, such as additional fracture or implant failure. 2
To date, there is no biomechanical study of the repair methods using sutures in feline patella fractures. The high complication rates using the PTBW technique in feline patella fractures indicate that an alternative surgical option is required to potentially increase the success rate. This study aimed to biomechanically evaluate and compare the PTBW technique, the CFEW method, and circumferential suturing combined with the figure-of-eight suture (CFES) using FiberWire.
Materials and methods
Fracture model preparation
A total of 28 pelvic limbs from 14 adult cat cadavers were collected and 27 of them were utilised. The mean weight of the cadavers was 3.78 kg (range 1.5–5.9 kg) and the cats had been euthanased or died of reasons unrelated to orthopaedic pathologies. The cadavers were stored at –20°C and then thawed at room temperature only when they were to be harvested and tested. After collection, the limbs promptly underwent the sampling and surgical process. Then, individually covered in saline-soaked gauze, the samples were refrigerated at 0°C until they were tested on the same day.
For the sampling process, the muscles, except for the quadriceps muscles, were removed from the femur, and then the quadriceps muscles were separated from the femoral bone. The quadriceps muscles were trimmed to remove the muscle mass, leaving only the tendon and fascia. The femoral bone was cut at the level immediately proximal to the patella groove. The soft tissue around the patella was preserved, but the synovium was opened to approach the articular surface of the patella. The patella was cut transversely in the middle with an osteotome and mallet; this is where transverse fractures are known to occur most often. 18
Surgical procedure
Group 1: pin and tension band wire
The PTWB technique was applied to the first group (Figure 1a). A single 0.9 mm Kirschner wire (K-wire) (Top Medical Co.) was drilled in a normograde manner, to reduce the fracture. Then, with a 20 G orthopaedic wire (Imedicom Co.), figure-of-eight wiring was applied, passing behind the proximal and distal ends of the K-wire. The wire was tightened at a proximal corner of the patella and the ends were cut, leaving 3–4 twists. The ends of the K-wire were bent caudally. The synovium and retinacula were left open in all the samples. The sizes of the implants were selected based on a previous biomechanical study and a clinical report.2,10

An illustration of the methods of repairing patella fracture. (a) Group 1: pin and tension band wire; (b) group 2: combination of circumferential and figure-of-eight wires; (c) group 3: combination of circumferential and figure-of-eight sutures with FiberWire
Group 2: combination of circumferential and figure-of-eight wires
A combination of CFEW techniques was applied to the second group (Figure 1b). A 20 G orthopaedic wire was inserted into the proximal and distal tendon of the patella. First, a circumferential wire was positioned and tightened to reduce the fragments. Then, a second wire of the same size was inserted deeper to the circumferential wire, and a figure-of-eight pattern was formed and tightened. Care was taken not to overtighten the wires and the wire twists were placed at the corners of the patella to minimise prominence.
Group 3: combination of circumferential and figure-of-eight sutures
In group 3, a combination of CFES with FiberWire (Arthrex Inc.) was applied (Figure 1c). The #2 FiberWire with a tapered needle was used to make a circumferential suture around the patella in a purse-string suture pattern. The suture was tightened with a surgeon’s knot followed by a square knot (total four throws), while taking extreme care not to lose tension while tying. A second suture was inserted into the proximal and distal tendon, deeper to the first one, and after forming a figure-of-eight pattern, was tightened with a surgeon’s knot and a square knot. The suture knots were placed at a proximal corner of the patella. Care was taken to put the suture around the equator of the patella, because if not, the fracture was seen to displace at the articular surface.
Biomechanical test
All the limbs were fixed laterally to a wooden plate with the knee joint in its normal standing angle (135°). The wooden plate was mounted on the lower side tensile grip of the Universal Testing Machine (Instron 4467; Instron) and the quadriceps tendon, covered in gauze to prevent slippage, was gripped by the upper side tensile grip (Figure 2). Care was taken to keep the patella on the trochlea throughout the test in order not to interfere with the tension band mechanism. Then a tensile force with a crosshead speed of 10 mm/min was applied. Meanwhile, a ruler was placed next to the patella and two cameras were synchronised to film the monitor showing the load differences and the marked fracture gap. The camera filming the sample was located at the left-caudal side of the sample, viewing the ruler and the fragment gap. The videos were analysed afterwards and the loads at displacements of 1, 2 and 3 mm were measured and recorded. Failure was defined as the point where the load showed an abrupt decrease, and the modes of failure were specified. Raw data were extracted to identify the maximum failure load of each sample.

A photograph of the biomechanical testing set-up. The limb with the femur cut proximal to the patellar trochlea (asterisk) is fixed laterally to a wooden plate. During the test procedure, a camera was set on the left-caudal side of the sample, filming the fragment and a ruler (dashed line) in a diagonal perspective
Statistical analysis
Using a statistical software program (Statistical Program for the Social Sciences v.28.0.1.1, SPSS Inc.; IBM), the Kruskal–Wallis test was applied to find the statistical significance between the groups, and when the P value was <0.05, it was considered to be significant. If there was significance among the groups, the significant differences noted between the groups were determined with a Mann–Whitney test. In this test, a P value <0.017 was considered significant.
Results
Loads at displacements of 1, 2 and 3 mm
Groups 1 (PTBW) and 3 (CFES), and groups 2 (CFEW) and 3 (CFES), were significantly different, respectively (P <0.017). On the other hand, there was no significant difference between groups 1 (PTBW) and 2 (CFEW) (Table 1, Figure 3).
Loads at displacements of 1, 2 and 3 mm
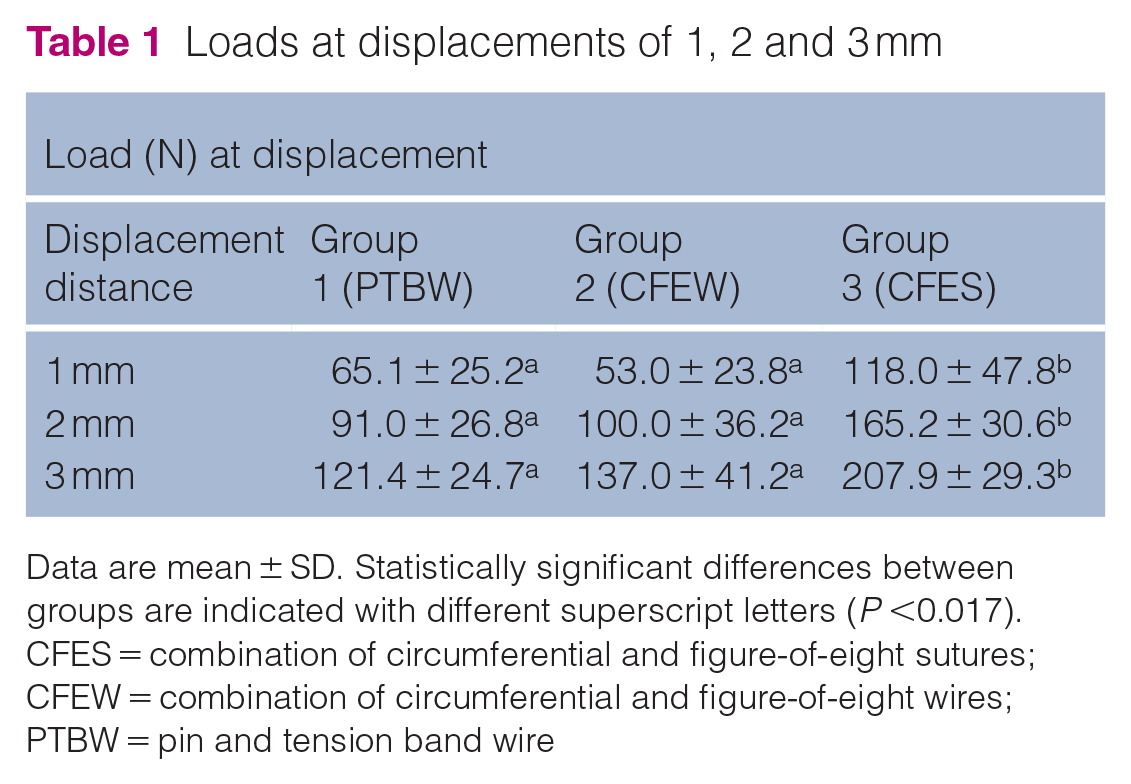
Data are mean ± SD. Statistically significant differences between groups are indicated with different superscript letters (P <0.017).
CFES = combination of circumferential and figure-of-eight sutures; CFEW = combination of circumferential and figure-of-eight wires; PTBW = pin and tension band wire

Box-and-whisker plot of loads at displacements of 1, 2 and 3 mm in each group. Groups that do not share the same letter are significantly different. There were significant differences between groups 1 and 3, and between groups 2 and 3, at each displacement distance. Group 1: pin and tension band wire; group 2: combination of circumferential and figure-of-eight wires; group 3: combination of circumferential and figure-of-eight sutures
Maximum failure load
In terms of maximum failure loads, there was a significant difference between groups 1 (PTBW) and 3 (CFES) (P <0.017) (Table 2, Figure 4).
Maximum failure load

Data are mean ± SD. Statistically significant differences between groups are indicated with different superscript letters (P <0.017).
CFES = combination of circumferential and figure-of-eight sutures; CFEW = combination of circumferential and figure-of-eight wires; PTBW = pin and tension band wire

Box-and-whisker plot of maximum failure load in each group. Groups that do not share the same letter are significantly different. There was a significant difference between groups 1 and 3. Group 1: pin and tension band wire; group 2: combination of circumferential and figure-of-eight wires; group 3: combination of circumferential and figure-of-eight sutures
Types of failure
At the end of the biomechanical test, all the samples arrived at failure after 3 mm displacement (Table 3). Here, tendon rupture implies breaking of the tendon tensile structure unrelated to the implant and suture insertion sites.
Types of failure

CFES = combination of circumferential and figure-of-eight sutures; CFEW = combination of circumferential and figure-of-eight wires; PTBW = pin and tension band wire
Discussion
The results of the present study suggest that a CFES combination is more resistant to displacement than a PTBW in this ex vivo feline patella fracture model.
In feline patella fracture surgery this is the first attempt to compare the biomechanical properties of metal implants and suture materials. In human medicine, there have been various attempts to evaluate whether the tension band suturing methods are comparable to tension band wiring with metallic implants. In most of the biomechanical studies, the results showed that the suture method is comparable to the wire method. Patel et al 19 suggested that Ethibond suture provides as sufficient support as metal wires, with no significant difference in the mean maximum fracture gaps. A study by Wright et al 20 compared FiberWire with wire and showed that a double-strand FiberWire with a modified wagoner’s hitch had the largest failure strength. In terms of clinical studies, a systematic review of non-metallic implants for patella fracture fixation found that among all studies, good clinical outcomes were reported, with complication rates up to 10.5% and removal surgery requirement up to 3.2%. 21 Several other clinical comparisons of suture repair vs wire fixation have reported satisfactory clinical outcomes but with fewer postoperative complications in suture methods.23–28
The results of the present study show consistency with those of a previous study comparing the different wiring methods in a feline patella fracture cadaveric model, in that the CFEW group was stronger than the PTBW group. 10 In this previous study, the CFEW group showed a 1.31-fold greater mean maximum failure load than that of the PTBW group, while in the present study, it was approximately 1.19-fold greater. This difference may be because, unlike the previous study, the retinaculum and synovium were not closed in this study, with the intention to measure the displacement of the fragments more accurately. This difference implies that adding soft-tissue sutures provides more stability to the joint, which has been emphasised in surgical repair of patellar luxation and cranial cruciate ligament rupture.29,30
Groups 2 (CFEW) and 3 (CFES) had significant differences in all displacement loads, but there was no significant difference between them in the maximum failure load. This may be due to group 3 (CFES), in which there was little difference between the mean load at 3 mm displacement and the mean maximum failure load. Correspondingly, there was only a little difference between groups 2 and 3 in their mean maximum failure load, thereby resulting in no significant difference between them. According to the types of failure in each group, tendon rupture unrelated to the implant site occurred in every group, and in group 3 (CFES), the number of samples in which tendon rupture occurred was double that of the other groups. In a previous study, the maximum load to failure of the #2 FiberWire was shown to be approximately 1.3 times greater than that in the present study. 31 This indicates that in the present study, the tendon was ruptured before the FiberWire itself reached its maximum failure load. Such a phenomenon is one of the limitations of the present study; since it was designed as an ex vivo study, the freshness of the soft tissue of the cadavers may have affected the results. 32
Given the small size of the patella in cats, it is worth comparing the technical feasibility of each surgical method. First, in group 1 (PTBW), it was extremely challenging to drill into the patella fragments while achieving correct apposition. Moreover, under the assumption that the cadaveric samples were of normal bone density, the friability of pathological fractures can increase the risk of further fracture when drilling.1,10 At this point, the frozen and thawed cadaveric bone samples were expected to have similar implant-holding power to that of fresh bone.33,34 Second, in group 2 (CFEW), tightening of the circumferential wire while preventing slippage of the wires from the equator of the patella was technically demanding. When overtightened, the articular surface of the fragments was displaced. In addition, double wire twists tended to be prominent, which can cause irritation, infection and reduction in the range of motion.10,13,21 Third, in group 3 (CFES), relatively less time and fewer techniques were required to achieve stable reduction, and the suture materials were much easier to handle than the metal wires. Such technical characteristics have been mentioned in the human literature several times, in which easier handling of the suture materials could shorten the operation time.15,18,19,22,35 On the other hand, the knot of the FiberWire can also cause a foreign body reaction and the braided materials have the potential risk of infection.36,37 However, according to numerous human clinical reports, repairing patella fractures with FiberWire has had a significantly lower rate of implant-related complications than that with wires.21,23 –25,27,28 The suture method may also provide an advantage in that it may avoid potential complications associated with drilling into the pathologically fractured patella.
The failure of stabilisation was defined as 3 mm displacement in this study. Sesamoid bones are known to mostly produce fibrous union instead of osseous union, and hence patella fractures may never show radiographic evidence of healing or require a considerably long period of time to do so.2,38 In cats, it has been reported that only 1/52 patella fractures showed radiographic evidence of healing 3 years after surgery, and in two young kittens it took 3–11 months.1,39 There is no established agreement on the failure criteria after feline patella repair surgery so far, but the clinical results are reported to be satisfying without complete osseous union.1,2,8 Accordingly, the aim of repairing patella fracture is more focused on reconstructing the quadriceps mechanism and holding the bone fragments close together.2,9 Therefore, it seems reasonable to establish the failure criterion as 3 mm displacement. The same criterion of failure has been used in previous studies, both in cats and in humans.7,8,10,14,20,40
There are a few limitations to this study. First, the sample size is relatively small, which could weaken the statistical power. Second, the biomechanical study design is limited to tensile force and does not include repetitive cyclic loading. Third, as this was an ex vivo study, the individual conditions of the cadaveric samples may have affected the results. Fourth, an osteotome and mallet were used to simulate patella fractures. This selection of instruments was made due to the extreme mobility of the patella when an oscillating saw was applied, resulting in inaccurate cutting. The osteotomy margins are reported to be more irregular and to have cortical fissures when cut with an osteotome and mallet rather than with a saw. 41 This variable may have caused irregularity at the fracture margins, which might result in the imperfect reduction of the fragments. Finally, the knot methods and the site of the wire twists were not specifically taken into consideration in this study. The various knot methods tested in human medicine revealed some knots with significant strength over the surgeon’s knot.19,20 The site of the wire twists was also reported to affect the biomechanical results in a human study. 42 Such variations may need to be compared in future studies.
Conclusions
This study demonstrates that in this ex vivo model, the use of CFES provides greater resistance to fragment displacement and construct failure than the techniques utilising orthopaedic wires. Further studies to compare the techniques in clinical cases are necessary.
Footnotes
Acknowledgements
Thanks to Hyun-Jong Choi, Kyung-Ah Yu, Min-Seok Park, Min-Gyu Shin, Seung-Chan Lee, Dong-Hwi Yu and Tae-Hyung Kim for all their support and contributions.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.