
Abstract
Practical relevance:
Periarticular stifle fractures are uncommon but challenging injuries to treat. There may be concurrent damage to the ligaments and stabilising structures of the stifle joint itself, which should also be evaluated (see Part 1 of this article series). Improved knowledge of the fixation options and biomechanical challenges of these injuries will aid clinical decision-making and effective repair.
Clinical challenges:
Due to their nature, periarticular fractures may have small juxta-articular fragments, which require additional thought to address during stabilisation. In juvenile animals, these fractures typically involve the physis and often can be managed with cross pin fixation. In adult cats, locking fixation, specialised plates or external skeletal fixators can be utilised to address the juxta-articular fragments. Readers should also be aware of patellar fracture and dental anomaly syndrome (PADS), where cats develop insufficiency fractures affecting the patella and proximal tibia. A careful oral examination should be performed in affected patients, as these cats may have persistent deciduous teeth. Close attention should be paid to preoperative radiographs for evidence of chronicity of the injury including sclerosis of the patella, remodelling and blunting of the fracture lines.
Aims:
The aims of the article are to review the current literature surrounding periarticular fractures of the stifle joint and to summarise the diagnosis, treatment, outcome and complications of each fracture type. As well as discussing general fracture fixation and biomechanical principles applicable to both dogs and cats, information is provided on specific issues facing cats, such as PADS.
Evidence base:
Published data is limited, with reports including only a small number of cats. The information and recommendations in this article have therefore been drawn from a combination of the available literature and the authors’ clinical experience.
Keywords
Distal femoral fractures
Fractures of the distal femur are most commonly Salter–Harris type I or II fractures affecting the distal femoral physis (see box on page 634). 1 In adult cats, fractures may occur in the supracondylar or condylar regions and may be simple or comminuted. Due to proximity with the stifle joint, it can be difficult to distinguish between distal femoral fractures and stifle joint instability. Careful palpation of the patella, patellar tendon and stifle, alongside radiographs of the stifle and femur, will aid characterisation of the specific injury. Importantly, fractures in this area may be complicated by concurrent ligament and tendon injury, especially bicondylar fractures. 2
Physeal fractures
Closure of the distal femoral physis occurs at between 54 and 76 weeks in intact cats. 3 Early neutering delays physeal closure in males and open physes can be seen as late as 24 months of age; 4 therefore, young adult male neutered cats can also sustain distal femoral physeal fractures.
As the distal physis is located within the stifle joint capsule an arthrotomy is required for repair of these fractures. 1 The distal metaphysis has four bony protuberances, which interdigitate with corresponding depressions in the epiphyseal surface. This anatomical feature is useful when reducing and aligning the fracture intra-operatively, and also contributes an element of rotational stability.1,5

The most common injuries, as mentioned above, are Salter–Harris type I (Figure 1) and II fractures, and the average age of those affected is 9.5 months and 6.5 months, respectively. 6 The hamstrings and gastrocnemius muscles usually pull the distal fragment caudally. 1 In order to achieve accurate fracture alignment, this caudal displacement must be overcome: it is, therefore, advisable to almost ‘over-reduce’ the distal fragment to prevent the caudal ‘pulling effect’ caused by the muscular tension. This will avoid the development of a cranial step postreduction, which would potentially interfere with the movement of the patella. Correct fracture alignment also maximises possible physeal growth and reduces the risk of extensive callus formation; the latter could lead to incorporation and contracture of the quadriceps muscle, 5 which would subsequently prevent stifle flexion.


Lateral (a) and caudocranial (b) radiographs of a Salter–Harris type I distal femoral fracture in a 7-month-old female cat. Note that image (b) is slightly rotated, but there is no injury to the tibial physes
Implants that cause compression across the physis should be avoided as they may reduce the growth potential of the physis. 7 Reported repair techniques include cross pinning and dynamic intramedullary pinning (ie, use of a Rush pin) (see box on page 635), as well as conventional intramedullary pinning. Cross pin fixation is most commonly utilised and experimentally this has been shown to sustain higher loads than the other techniques when a torsional load is applied. 9 In comparison with cross pinning, conventional intramedullary pinning resisted less than two-thirds of the torsional force. Stabilisation involving intramedullary pinning alone is only possible due to the inherent rotational stability of the distal femoral physis; it, therefore, should only be used if there is no loss of integrity of the metaphyseal bony protuberances (ie, for Salter–Harris type I fractures). 9
Other types of Salter–Harris fractures of the distal femoral physis are rare. Type IV fractures are treated like simple condylar fractures (see later).

Supracondylar fractures
Supracondylar fractures are anatomically and biomechanically challenging to repair (Figure 2). They have no inherent stability and the distal nature of the fracture adjacent to the stifle joint subjects the fracture repair to significant bending forces. 10 There is also limited space in the distal fragment for implant placement. For these reasons, a variety of implants may need to be used in order to provide adequate stability, especially if the fracture is comminuted (see box on page 636).


Lateral (a) and caudocranial (b) radiographs of a comminuted supracondylar femoral fracture. Images courtesy of Sandra Corr
Condylar fractures
Fractures of the distal femoral condyle can be unicondylar, bicondylar or affect the femoral trochlea. As these fractures are articular by definition, accurate anatomic reconstruction, internal fixation and interfragmentary compression are required to limit degenerative joint disease and maintain a functional joint.
Unicondylar fractures
Unicondylar fractures affect either the medial (most commonly) or lateral aspect of the condyle. Usually, there is minimal displacement of the medial condyle if the medial collateral and caudal cruciate ligaments remain intact.1,8 A medial or lateral parapatellar approach is performed depending on which aspect of the femoral condyle has fractured. The fracture is anatomically reduced and can be temporarily stabilised using large pointed reduction forceps. A transcondylar lag screw (2.0 or 2.7 mm) is placed, inserting the screw from the medial or lateral epicondyle. An anti-rotational Kirschner wire (0.8–1.1 mm) is placed from the same epicondyle into the transcortex of the femoral metaphysis. 1
Bicondylar fractures
Bicondylar fractures, or those with a ‘Y’ or ‘T’ configuration, affect both aspects of the condyle and extend into the supracondylar region (Figure 3). Repair of these fractures is complex, especially when comminuted, and preoperative CT and three-dimensional reconstruction may be useful during the surgical planning.

Comminuted bicondylar fracture. This was repaired with Kirschner wires and screws. A type I transarticular external skeletal fixator was used to support the repair for 6 weeks
Usually, both a medial and lateral approach to the stifle joint is required to reduce and stabilise these fractures. The joint should be thoroughly inspected for ligament and meniscal damage, which usually occurs concurrently with this injury.2,8 If reduction of the condylar fragments is challenging, osteotomy of the tibial tuberosity and reflection of the patellar tendon can enhance visualisation of the articular surface. This can be stabilised after fracture repair with two 0.8–1.1 mm Kirschner wires and a 0.8 mm tension band wire. The intra-articular fragments of the bicondylar fracture should be stabilised first with a transcondylar lag screw (usually 2.0 or 2.4 mm) to prioritise accurate anatomic reconstruction of the articular surface. The supracondylar region can be stabilised as described earlier. Good stability is gained when using bilateral 2.0 mm locking plates. Alternatively, reconstruction plates or supracondylar plates can be used. Cross pinning and dynamic intramedullary pinning have also been described; however, these techniques provide less stability and so should only be considered in young cats with simple reducible fractures. 1
Condylar trochlear fractures
These fractures differ from the standard condylar fracture patterns described above and involve the femoral trochlea. In most cases they are comminuted, with one or several fracture lines crossing the trochlea in transverse or oblique directions. 16 The articular surface of the trochlea must be restored to adequately support the stifle extensor mechanism. Repair is typically challenging and may require a combination of screws, pins and plates, depending on the size of the fragments.1,14 Large fragments can be reduced and secured to the condyle using pinning; however, attempting the same with small fragments would be very challenging and it is usually worth removing them instead.
As an alternative, a patellar groove replacement (PGR) prosthesis has been used in dogs to treat severe femoropatellar osteoarthritis secondary to patellar luxation, by substituting the whole femoral trochlea. 17 Although 10 different sizes of PGR prosthesis are available, no studies have yet investigated the feasibility of this surgical treatment in cats.

Patellar fractures
Patellar fractures secondary to trauma are rare in cats. They are usually found concurrently with distal femoral fractures, proximal tibial fractures, cruciate ligament rupture or patellar luxation.18,19 Surgery is challenging and large tensile forces from the quadriceps muscle must be counteracted by small implants. Importantly, traumatic fractures need to be differentiated from spontaneous patellar fractures, which are thought to be insufficiency fractures secondary to pathological bone disease and internal stresses (see Table 1). 20

y = years; m = months
Spontaneous patellar fractures
Young adults are commonly affected, with a mean age of 28 months. 18 Lameness can be acute or chronic, or cats may be asymptomatic. Spontaneous fractures are usually simple transverse fractures affecting the proximal third to mid-body of the bone (Figure 4). Often, both stifles are affected, with a median delay of 3 months between each fracture. 21

Lateral (a) and caudocranial (b) radiographs of a spontaneous fracture of the patella. Note the sclerosis and transverse configuration of the fracture in the proximal third of the bone. Images courtesy of Matteo Cantatore
Radiographically the patella may be sclerotic, with blunting of the fracture line providing evidence of chronicity. Peri- or intra-articular mineralisation is frequently reported. Importantly, the contralateral patella should always be radiographed in any cat presenting with a patellar fracture. This allows detection of fractures or early signs of fatigue in the contralateral side (ie, sclerosis and remodelling), and aids differentiation from traumatic fractures. A careful oral examination should also be performed in affected patients as these cats may have persistent deciduous teeth. 18 In particular, they may be suffering from a pathological bone disease, recently termed patellar fracture and dental anomaly syndrome (PADS), and many cats will go on to sustain insufficiency fractures of other bones (eg, proximal tibia) at a later date.18,22,23
Treatment options for spontaneous patellar fractures vary, depending mainly on clinical signs but also fracture displacement. Minimally displaced fractures, and cats with chronic mild lameness, should be managed conservatively. 20 Conservative management has also been reported to be successful in cases with lameness on presentation and mild-to-moderate fragment displacement. 24 However, surgery should be considered in cases with moderate-to-marked lameness and significant displacement of fragments. 20
Biomechanically, the use of a pin and tension band wire, placed perpendicularly to the fracture line, is the superior option to counteract the large tensile force of the quadriceps muscle. However, a complication rate of 86% is reported and so this approach is not recommended. The sclerotic patella is brittle and prone to further fragmentation on implant placement. 21 Instead, a circumferential wire (from 0.20 mm/32 G to 0.5 mm/25 G in diameter, depending on the size of the cat) can be placed without risk of causing further iatrogenic damage to the patella. Although this option provides great stability initially, the encircling wire around the patella will eventually break, producing irritation in the surrounding soft tissues; thus a second surgery is usually required to remove the implant. An alternative is to use an encircling suture of non-absorbable material (nylon or polypropylene). 24 A tibial-quadriceps wire can also be placed; this relieves the tension on the quadriceps mechanism and theoretically may increase the likelihood of patellar healing. The wire is placed through a drill hole in the proximal tibial tuberosity and through the quadriceps tendon around the proximal part of the patella. Orthopaedic wire or FiberWire (Arthrex) can be used. It typically breaks 6–10 weeks postoperatively. 18
As a salvage procedure, partial patellectomy can be performed if internal fixation fails or is not possible, or if there is persistent lameness despite conservative management. 20 Total patellectomy is absolutely contraindicated in cats due to their propensity for jumping. This procedure will lead to persistent lameness and atrophy of the quadriceps muscle. 25 Amputation is also contraindicated due to the high incidence of bilateral patellar fractures. 21
Traumatic patellar fractures
About 20% of patellar fractures are traumatic. 18 While significant inciting trauma is required for them to occur, this is rarely witnessed due to the cat’s independent lifestyle, usually with outdoor access. In comparison with spontaneous fractures, lameness is acute in onset and associated with wounds around the stifle joint, long bone fractures or ligament/tendon injuries. 20 Radiographically, fracture lines will be sharp and there should be no sclerosis of the patella.
Treatment options depend on the fracture configuration. Small polar fragments can be managed conservatively or excised. These small fragments have little effect on the extensor mechanism or on the femoropatellar articulation; therefore, removal should not reduce function. 18 Importantly, the integrity of the patellar tendon must be preserved and primary surgical repair of ruptured soft tissue performed.
Large fragments require surgical treatment in order to restore function of the quadriceps mechanism. Anatomic repair is also required to restore congruity. Longitudinal fractures can be repaired with a skewer pin and tension band wire or an encircling wire.18,20,26 Again, a tibial-quadriceps wire can be placed to relieve tension on the repair. 20 However, forces acting on longitudinal fractures are likely to be less than those on transverse fractures because the strong tensile forces run parallel to the fracture line, rather than perpendicular to it. 26 Tensile forces leading to fragment distraction would instead come from the femoropatellar ligaments; therefore, there may be some rationale for medial/lateral desmotomy to relieve tension with this fracture configuration. 26

Pin and wire placement will help to reduce the shear forces, allowing patellar healing. 26 There is also a case report documenting use of horizontal mattress sutures (0 polydioxanone) for longitudinal fracture reduction and repair; specifically, the horizontal mattress suture was placed so as to encircle the whole patella through the surrounding soft tissue, holding the two fragments in reduction. 19 Reported advantages include easier application, greater resistance to failure secondary to repetitive loading and possibly increased patient comfort. In the same case report, arthroscopy was used for full assessment of the patellar injury and it allowed minimally invasive assessment of damage to the surrounding soft tissue. 19
Treatment of comminuted patellar fractures must be tailored to the specifics of the case. A combination of multiple pins, orthopaedic wire and partial patellectomy may need to be considered. In some cases, only partial reconstruction of the patella may be possible, but, as discussed earlier, total patellectomy should not be performed in cats. 20
Most traumatic patellar fracture cases will also require management of concurrent fractures, cruciate ligament rupture and/or patellar luxation under the same anaesthetic.
Proximal tibial fractures
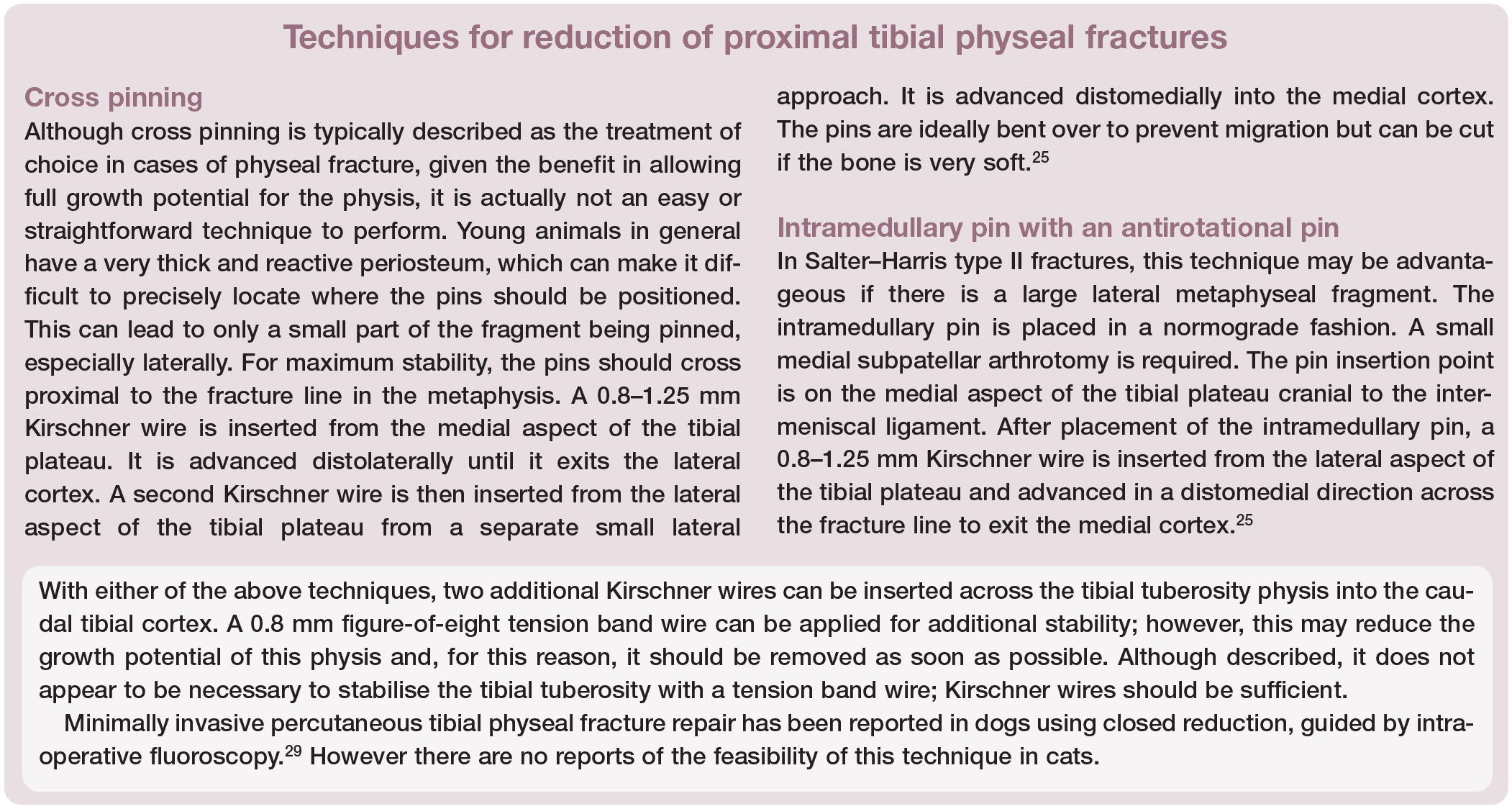
Fractures involving the proximal tibia are rare in cats. Usually the fibula is also fractured. In immature cats physeal fractures can occur, which are typically Salter–Harris types I and II (see page 634). 27 In adult cats, fractures affecting the proximal tibial metaphysis may be traumatic or may be secondary to fatigue stress. 28 Other fracture types that can occur, but are even more rare, are avulsion fractures of the tibial tuberosity or metaphyseal fractures extending into the stifle joint. 27
Physeal fractures
Physeal tibial fractures are very rare in cats. The proximal tibia has two separate physes, one for the growth of the proximal epiphysis and one for the tibial tuberosity apophysis. When open, these physes can fracture individually, as either a Salter–Harris type I or II fracture of the proximal epiphysis or as an avulsion of the tibial tuberosity. Between 36 and 44 weeks of age, these two physes fuse, leading to a single cap above the metaphysis. Fractures can still occur at this time, usually as Salter–Harris types I and II. From 50–76 weeks of age this combined physis then fuses with the metaphysis. 27 Neutering has been shown to delay the closure of the tibial tuberosity physis in males, but not that of the proximal epiphysis. 4
On fracturing, the proximal tibial epiphysis tends to displace caudolaterally in relation to the tibia. If left untreated, it would lead to a very steep tibial plateau angle, affecting the function of the stifle joint. Unless there is no displacement, open reduction and internal fixation is indicated. Typically surgical intervention (see box on page 641) should be prompt (within 3 or 4 days of the traumatic event), as physeal fractures heal and stabilise very quickly, and reduction is especially challenging when this occurs. Fracture reduction is most easily performed with the stifle joint in extension. Care must be taken not to cause iatrogenic damage to this fragment as it is small and soft. 27 Postoperatively, the limb should be radiographed in different positions, such as flexed and extended, in order to evaluate the overall mobility of the stifle joint and identify any uncorrected fracture displacement.
Metaphyseal fractures
Metaphyseal fractures in adult cats are more common than physeal fractures. Importantly, this is an area where stress insufficiency fractures have been reported secondarily to repeated/cyclic low-grade trauma. For this reason, they must be differentiated from traumatic fractures, which typically result from acute severe trauma. The tension exerted by the patellar tendon causes the proximal fragment to tilt in a proximocranial direction. These fractures can be challenging due to the small proximal fragment with limited bone stock for implant placement. 27
Transverse stress fractures
Transverse stress fractures of the proximal tibia (Figure 5a) have been reported in a group of 10 cats that also had concurrent bilateral non-union spontaneous patellar fractures, 28 and are likely to be cats with PADS. The mean age of the affected cats was 8 years 5 months. Nine of these cats had additional fractures elsewhere and, in four, both tibiae were affected. Radiographic evidence of chronicity was identified, with thickening and sclerosis of the cranial cortex at the level of the fracture site. 28

(a) Lateral radiograph of a transverse stress fracture of the proximal tibial metaphysis. (b) Postoperative radiograph following repair with an intramedullary pin, type I external skeletal fixator and a cranial tension band wire. Note also the concurrent spontaneous patellar fracture. Images courtesy of Sorrel Langley-Hobbs
Surgical treatment is recommended for these fractures. Options include an intramedullary pin and type Ia external skeletal fixator, or a medial plate. T- or L-plates may be advantageous to allow insertion of more screws in the proximal fragment. Locking fixation can also be considered due to its superior stability when only two screws are possible in one fragment. 13 Marked distraction of the cranial aspect of the fracture is common, so tension band fixation is advised (Figure 5b). This can be achieved either with a figure-of-eight tension band wire or a cranial plate.27,28
Traumatic fractures
Traumatic fractures can be very challenging to repair, especially when comminuted or when the proximal fragment is very small (Figure 6). Multiple implants may need to be considered. Often comminuted fractures extend into the tibial diaphysis and are treated as comminuted diaphyseal fractures. In this scenario, plates will be used in bridging mode given that it is not possible to perfectly reduce the fracture. Locking fixation is again particularly useful because of the increased stability obtained, in comparison with conventional plates, when it is only possible to place two screws in one fragment. 13 Other options include 2.7 mm dynamic compression plates, 2.4 mm limited-contact dynamic compression plates, stacked 2.0/2.7 mm veterinary cuttable plates, T- or L-plates and supracondylar plates. The addition of an intramedullary pin will increase stability by reducing the bending moment on the plate. 30

Proximal articular tibial fracture in a 22-month-old cat. These types of fractures are challenging to repair due to the small size of the fragment. This fracture was stabilised with two positional screws. The medial collateral ligament was also partially torn; therefore, a ligament prosthesis was placed (see Part 1)
If there is limited bone stock proximally for implant placement, biaxial plating can be considered, with plates placed medially and cranially. The cranial aspect of the tibia should be accessible from a medial approach to the tibia and stifle joint. Bone grafting (either autogenous cancellous bone graft or feline demineralised bone matrix) is recommended in cases with large fracture gaps or moderate-to-severe comminution. An alternative is the use of an external skeletal fixator: 2.0 mm transosseous pins can be placed proximally; however, smaller 1.6 mm pins should be placed in the distal tibia. Ideally, three pins should be placed in the proximal and distal fragments; if only one to two pins can be placed proximally, a type II or III external skeletal fixator is advised. 27 Circular external skeletal fixators are also useful when there are small juxta-articular fragments but their placement requires a high level of surgical skill.
Postoperative care
Strict rest is imperative after fracture repair, usually 6 weeks for adult cats and 3–4 weeks for immature cats. At the end of this period, patients should be reassessed and radiographs taken to evaluate bony healing and implant integrity. Complications include impant failure, infection, delayed/non-union and quadriceps contracture in cases of femoral fracture.1,5,7,27 Physical rehabilitation is paramount when there is limited limb use in the early postoperative period, in order to minimise the risk of quadriceps contracture. In cases where external skeletal fixators have been used, cats will require more frequent check-ups, usually every 2 weeks. Also owners should be educated regarding pin tract cleaning and daily assessment, as well as the clinical signs of infection and pin migration (ie, lameness, soft tissue swelling, erythema, pain, pin tract discharge).

Key Points
Periarticular fractures can occur alongside damage to the ligaments and stabilising structures of the stifle joint; therefore, stifle stability should always be assessed in these cases.
Most periarticular fractures in immature cats are Salter–Harris type I or II fractures. Implants causing interfragmentary compression should be avoided.
Locking fixation, biaxial plating, circular external skeletal fixators and specialised plates (T-, L- and supracondylar plates) can be useful in cases with small juxta-articular fragments and limited bone stock.
Insufficiency fractures can involve the patella and proximal tibia. Fractures in these regions should be assessed for signs of chronicity and veterinarians should be aware of their typical configuration.
Patellar fracture and dental anomaly syndrome (PADS) is a recently described condition. It is important to diagnose because many cats will go on to sustain insufficiency fractures in other bones.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.