
Abstract
Practical relevance:
While feline patellar fractures are not commonly encountered in practice, they tend to be found more often in younger cats; no breed or sex predispositions are recognised. If there is no evidence of a traumatic aetiology, the cat may be suspected of having patellar fracture and dental anomaly syndrome (PADS). Patellar fractures are easy to diagnose on lateral radiographs and there are several different fracture types. The type of fracture, the age of the cat at fracture occurrence and whether there is suspicion of a pathological aetiology are all relevant when considering treatment technique.
Clinical challenges:
While some cats with patellar fractures will do well with conservative management, surgical treatment is often indicated and decision-making can be challenging.
Evidence base:
Information and recommendations provided in this review are based on the literature and the author’s own clinical experience. There are several publications on PADS, but there is limited evidence as to what the underlying cause of this condition is, and the best method for managing patellar fractures is still an area where more research is needed.
Aim:
This review aims to gather the papers, case series and case reports published over the past few decades in order to discuss how best to manage different types of patellar fractures.
Keywords
Anatomy
The patella is the largest sesamoid bone in the body. 1 In the cat, the patella is proportionately wider and larger when compared with the size of the animal than in the dog. The patella has a convex articular surface and is seated in the trochlear sulcus of the femur. The function of the patella is to protect the tendon of the quadriceps during weight-bearing and energetic activity such as jumping. The feline patella has to withstand the very high forces that the cat generates when landing with a flexed hindlimb after jumping from heights.
The anatomy of the feline stifle and patella is shown in Figure 1. The quadriceps muscle is composed of the vastus lateralis, vastus medialis, vastus intermedius and rectus femoris, which unite to form the quadriceps tendon that attaches to the proximal patella. 1 The tendon continues over the cranial surface of the patella to merge with the patellar ligament. The patellar ligament is a strong band of fibrous connective tissue that connects the patella to the tibial tuberosity. The patella is held in place by the parapatellar fibrocartilage, which connects the medial and lateral surfaces of the patella with the joint capsule. 1 The fibrocartilage also functions to articulate with the trochlear ridges, increase surface area and disperse forces of the quadriceps muscles. 1 As the quadriceps muscles contract, the patella is pulled proximally and the stifle is extended. 1

(a) Craniocaudal and (b) mediolateral feline stifle and patella anatomy
The patella plays a vitally important role in the extensor mechanism of the stifle. 1 If the patella is fractured then stifle extension is affected.
Nature of patellar fracture
There have been many papers, short case series and case reports published on feline patellar fractures in the past few decades.2–14 Reported types and orientations of fractures include simple, transverse, comminuted, longitudinal, longitudinal oblique, marginal and polar.2–14 Patellar fractures can also be divided into traumatic or pathological fractures.7,9
The specific type of fracture not only guides the decision about which treatment to select, but also whether to be vigilant for the underlying condition of patellar fracture and dental anomaly syndrome (PADS).
Patellar fractures can occur in any breed and both sexes of cat, but are more common in younger cats. 9 Age at fracture occurrence is also relevant when considering treatment technique.7,14
History and aetiology of patellar fracture
Cats may present with a history of significant trauma, or may be suspected of sustaining such trauma, for example from a road traffic accident, and there may be concurrent injuries including other traumatic fractures. 7 Cats may also present with sudden-onset lameness affecting one leg, and, as is sometimes the case in these cats, with no observed trauma.
Lower energy trauma, such as a fall or jump, can result in a simple patellar fracture if the cat lands heavily on its feet and there is a sudden forceful contraction of the quadriceps muscle against a fixed flexed stifle; this is known as an indirect fracture. If a cat lands directly on its patella, or there is direct trauma to the patella, this could also result in a fracture; in such cases there would likely be soft tissue trauma to the region of the patella and bruising of the skin and tissues over the patella. Alternatively, patellar fracture (usually transverse avulsion fracture) may be caused by a combination of forces from a jump and direct trauma to the patella (ie, the two types of force acting simultaneously could result in the fracture injury). With longitudinal, oblique or marginal fractures it may be more difficult to determine the aetiopathogenesis but a fall, landing awkwardly or a direct blow to the bone are likely to be implicated either alone or in combination.
Clinical and orthopaedic examination
It is very important to perform a full physical and orthopaedic examination to ascertain whether there are other traumatic injuries that may be more significant than the patellar fracture itself; for example, injuries resulting from a road traffic accident. If there is no evidence of a traumatic aetiology, the cat may have suffered a pathological patellar fracture, as in cats with suspected PADS (see box). In these cases, the cat’s mouth should be checked carefully for persistent deciduous teeth or unerupted adult teeth,9,15 and a physical orthopaedic examination performed to assess for any evidence of joint or bone pain that might indicate concurrent fractures. 16 Obtaining radiographs of the pelvis at the same time as the stifles is a useful screening tool for the presence of some of the most common preceding fractures. 16 The patient’s clinical history should be carefully reviewed for evidence of these abnormalities and may reveal, for example, that the cat had persistent deciduous teeth removed at the time of neutering, or perhaps had an unexplained and uninvestigated bout of lameness previously.
Cats with minimally displaced patellar fractures may walk normally or show only mild lameness. If the patellar fracture is completely displaced and the quadriceps mechanism disrupted, then the cat will walk with a flexed (dropped) stifle -in other words, on weightbearing, the stifle will flex, as the cat will have an inability to keep the stifle extended (see video in the supplementary material). There may be pain and swelling around the stifle joint, and some bruising or wounds adjacent to the patella. If the patellar fracture is not disrupting the quadriceps mechanism - for example with a longitudinal patellar fracture - then concurrent problems such as patellar luxation may be contributing to pain and instability and thus be the main cause of the lameness.



In this cat with suspected patellar fracture and dental anomaly syndrome (PADS), a chronic patellar fracture was only noted when the cat was presented with a transverse fracture of the proximal tibia
The cat’s stifle should be examined carefully for any instability caused by a cruciate ligament rupture (cranial or caudal), by performing cranial draw and cranial tibial thrust tests, and for patellar luxation (medial or lateral). Both cranial and caudal cruciate ligament ruptures have been reported in association with patellar fractures. 7

Diagnostic imaging
Imaging is essential to gain more information on the fracture and to assess for preceding or concurrent injuries. Cruciate ligament rupture, for example, can be indicated by evidence of joint effusion and/or periarticular osteophytosis on radiographs. In addition, dental radiography or a CT scan will be useful if there is any suspicion of PADS, particularly when looking for unerupted adult teeth.


(a) Mediolateral and (b) ventrodorsal radiographic views of a cat with hindlimb lameness (and a history of one previous episode of similar lameness). (a) A transverse patellar fracture, with significant fragment distraction, is clearly visible (white arrow and inset image). There is increased bone density of the patella, with the trabecular pattern partly obscured, particularly just adjacent to the fracture line. (a,b) There is also a healing acetabular fracture visible (black arrows), shown to be on the right in (b). In addition, the cat had persistent deciduous teeth, which were removed at the time of neutering. These findings suggest that this cat had PADS
Good quality radiographs alone are usually sufficient to show a fracture, and orthogonal views should be taken in all cases, although certain other projections will tend to be more useful depending on the fracture configuration (see box below). A skyline view (cranioproximal to craniodistal oblique view of the patella and trochlear groove) can be a useful addition when identifying longitudinal fractures.7,8 Stressed views can assist in decision-making for treatment. By taking views with the stifle in both a neutral and then flexed position, the gap between the patellar fracture fragments can be measured, giving an indication of the degree of instability of the fracture (Figure 4).
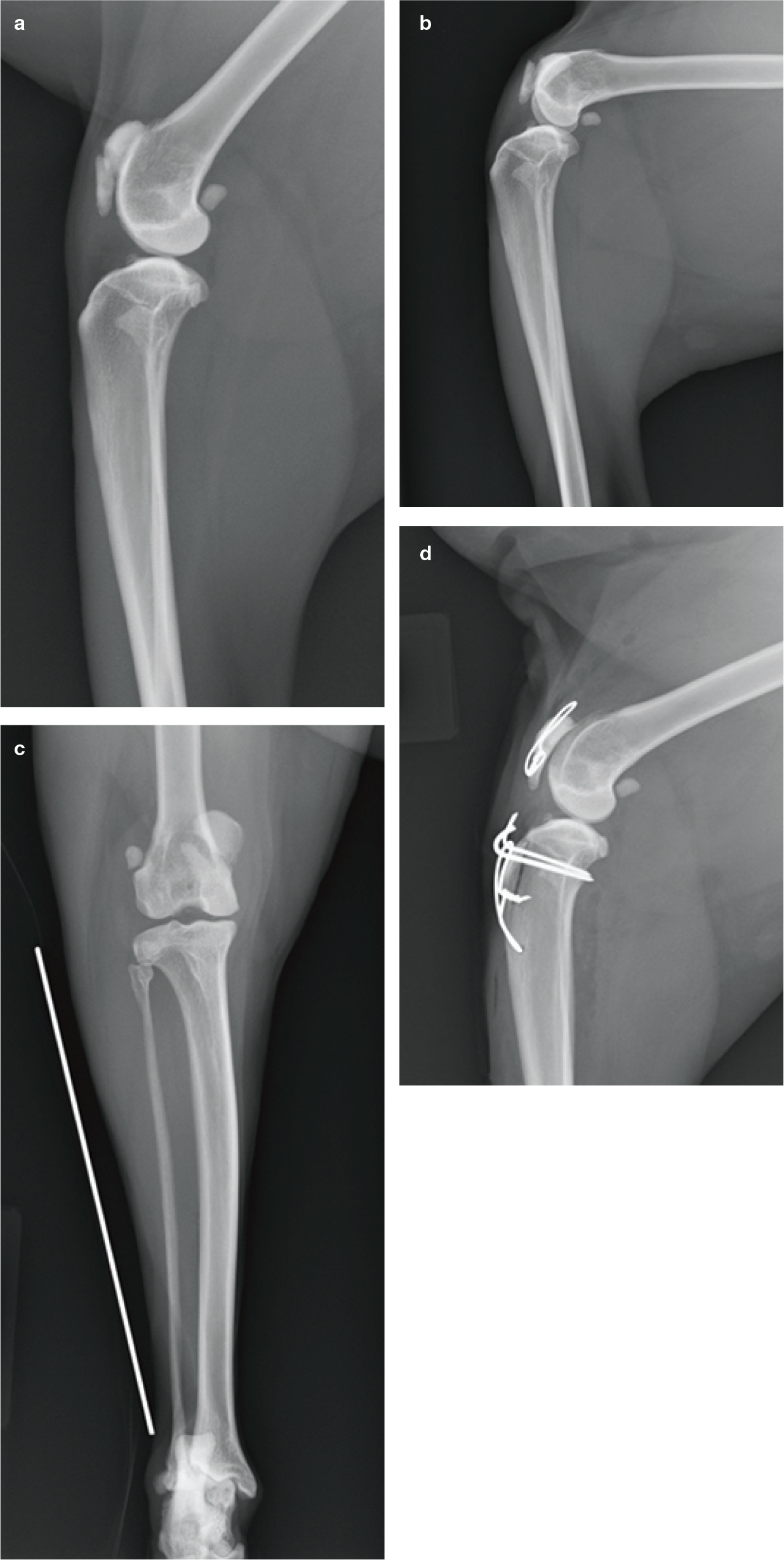
Radiographic examination of a cat presenting with chronic lameness and medial patellar luxation. (a) Neutral and (b) stressed flexed mediolateral views showing a chronic longitudinal oblique fracture (note the blunt edges of the fracture, indicating the chronic nature of this injury). On the flexed view there is no displacement of the proximal fragment further proximally, suggesting that the quadriceps mechanism is intact in this cat. (c) Craniocaudal view showing the displacement of the patella medially. (d) The fracture was reapposed using a piece of 22 G orthopaedic wire placed in a cerclage fashion. The patellar luxation was addressed by tibial tuberosity transposition and a block recession sulcoplasty
CT or MRI are not usually necessary but could be considered, particularly for (very early) non-displaced fractures, where the fracture line may otherwise be difficult to identify.
Options for managing patellar fractures in cats
Conservative management
Conservative management, whereby the patient is rested and prevented from jumping for a period of time, has resulted in a successful return to function in many cats with patellar fracture.9,11 In humans, stable non-displaced fractures (less than 2 mm of dislocation) are considered suitable for a conservative approach. 21 Before conservative treatment is instigated in humans, it is recommended that cases are tested (using fluoroscopic imaging) under 60° of knee flexion in order to confirm a stable situation with no tendency for displacement. 21
In cats, both fractures that are non-displaced and those that are significantly displaced have been treated conservatively, with animals regaining good function in both scenarios.9,11 However, no study has been performed in cats with patellar fractures to compare conservative management with reconstruction of the quadriceps mechanism, and to explore the outcome of these two management approaches in terms of time to return to function and long-term outcome. It is the author’s belief that when the fragments are widely displaced, the cat may experience a quicker return to function if an attempt is made to restore the quadriceps mechanism.
Pin and tension band wire
Fracture of the patella will usually result in disruption of the extensor mechanism and an avulsion injury. According to orthopaedic principles, avulsion fractures are generally best repaired with a pin and tension band wire. This has been shown to be the optimum technique for a transverse fracture of a normal patella in humans,21,22 with fractures commonly stabilised with two 1.6 mm Kirschner wires (K-wires) and 20 G or 18 G orthopaedic wire or suture in a figure-of-eight pattern. In cats, the small size of the patella would generally preclude the use of more than one small K-wire (0.6–0.9 mm); orthopaedic wire of 22-24 G is then used for the figure-of-eight tension band.
Pin and tension band wires have been used successfully to stabilise traumatic fractures of the patella in cats (Figure 5). 7 This technique is not, however, recommended if the fracture is thought to be pathological, as in cats with suspected PADS, due to the high risk of creating additional fracture fragments in the brittle bone and subsequent failure of the stabilisation (Figure 6). The failure rate of pin and tension band fixation of patellar fractures in cats suspected of having PADS is extremely high (75–86%).9,11
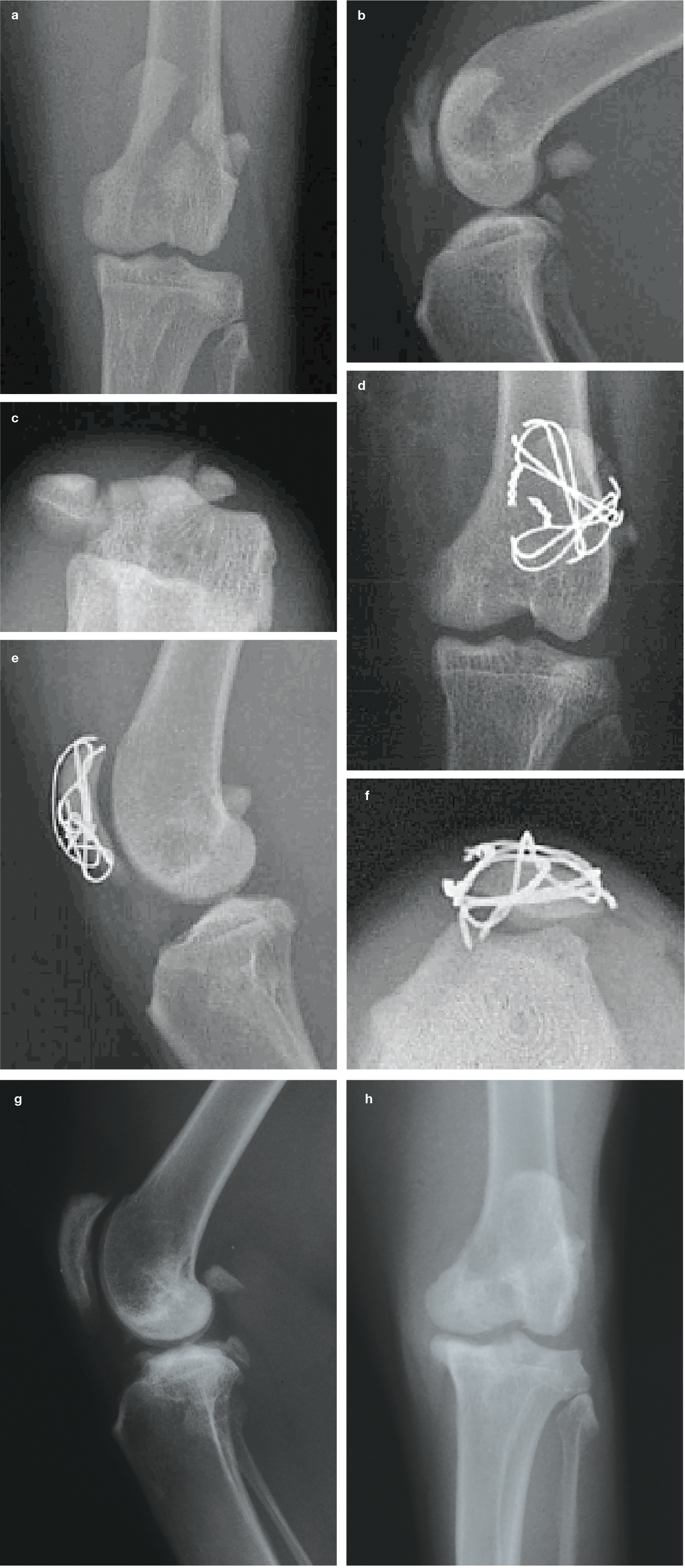
(a) Neutral and (b) stressed flexed views of a traumatic comminuted patellar fracture. Note the minimal displacement of fragments proximally, even on the flexed stifle radiograph (b). (c) Skyline view demonstrates medial displacement of the main fracture fragment. (d-f) The fracture was repaired in this instance with two 0.8 mm K-wires and several tension band wires as there were multiple fragments. (g,h) The implants were removed after 4 months, at which time the fracture had healed. Reprinted from Langley-Hobbs SJ, et al, 7 with permission of Georg Thieme Verlag KG

Attempted surgical fixation of a tranverse patellar fracture in a cat suspected of having PADS, with subsequent breakdown of the repair. (a,b) A pin, figure-of-eight tension band wire and tibiopatellar suture with nylon leader line and a metal tube crimp (see box on page 656) were placed; the drill hole through the proximal tibia, which the suture passes through, is visible. (c) Failure of the pin and tension band wire stabilisation. This repair technique is not recommended in cats suspected of having PADS
Circumferential wiring/suture
A less invasive technique for stabilising a patellar fracture (and thereby reconstructing the quadriceps mechanism) involves placing a suture or wire around the patella in a circumferential or ‘purse string’-type pattern (Figure 7). This approach not only restores the quadriceps mechanism, but decreases the fracture gap and does not interfere with the patella or cause further damage. It appears to be one of the most satisfactory options for pathological fractures (cats with suspected PADS), or where fragments are too small to place a K-wire. Malleable orthopaedic wire is commonly used, which will fatigue and break, but has good stiffness in the early phases. Use of suture material, rather than wire, seems to offer some advantages, and has been associated with decreased complication rates and similar success rates in human studies.21,22

(a) CT image of a distracted transverse patellar fracture in a cat with suspected PADS. As the lameness was marked, the option of trying to reconstruct the quadriceps mechanism to re-establish the ability to extend the stifle during weightbearing was chosen. (b,c)This was achieved with a suture using 40 lb nylon leader line in a figure-of-eight pattern and a metal tube crimp. The reduction of the patellar fracture is imperfect, and this is not unusual, but the gap between the two fragments has been reduced significantly. The cat recovered rapidly from surgery, showing an improved gait immediately postoperatively. At follow-up after 6 weeks, the gait improvement had been maintained

Patellectomy
The patella plays an intricate role in the extensor mechanism of the stifle and removal of the patella will result in degenerative lesions; hence the patella should be preserved whenever possible. Total patellectomy is not recommended in cats as they will have reduced function of their quadriceps mechanism, affecting their ability to jump; it has, though, been performed as a salvage procedure in cases where reconstruction is not possible (ie, the patella is so completely destroyed that there are no fragments large enough to contribute to the extensor mechanism). 4 The author would advise that conservative management be considered in these cases prior to patellectomy.
Partial patellectomy for small fragments that are not reconstructable can be considered. 2
Treatment decision-making and outcomes
When considering how to manage patellar fractures in cats, it is useful to subdivide them according to the cause, nature and type of fracture, and age of the cat, as summarised in Table 1.
Summary of patellar fracture types seen in cats
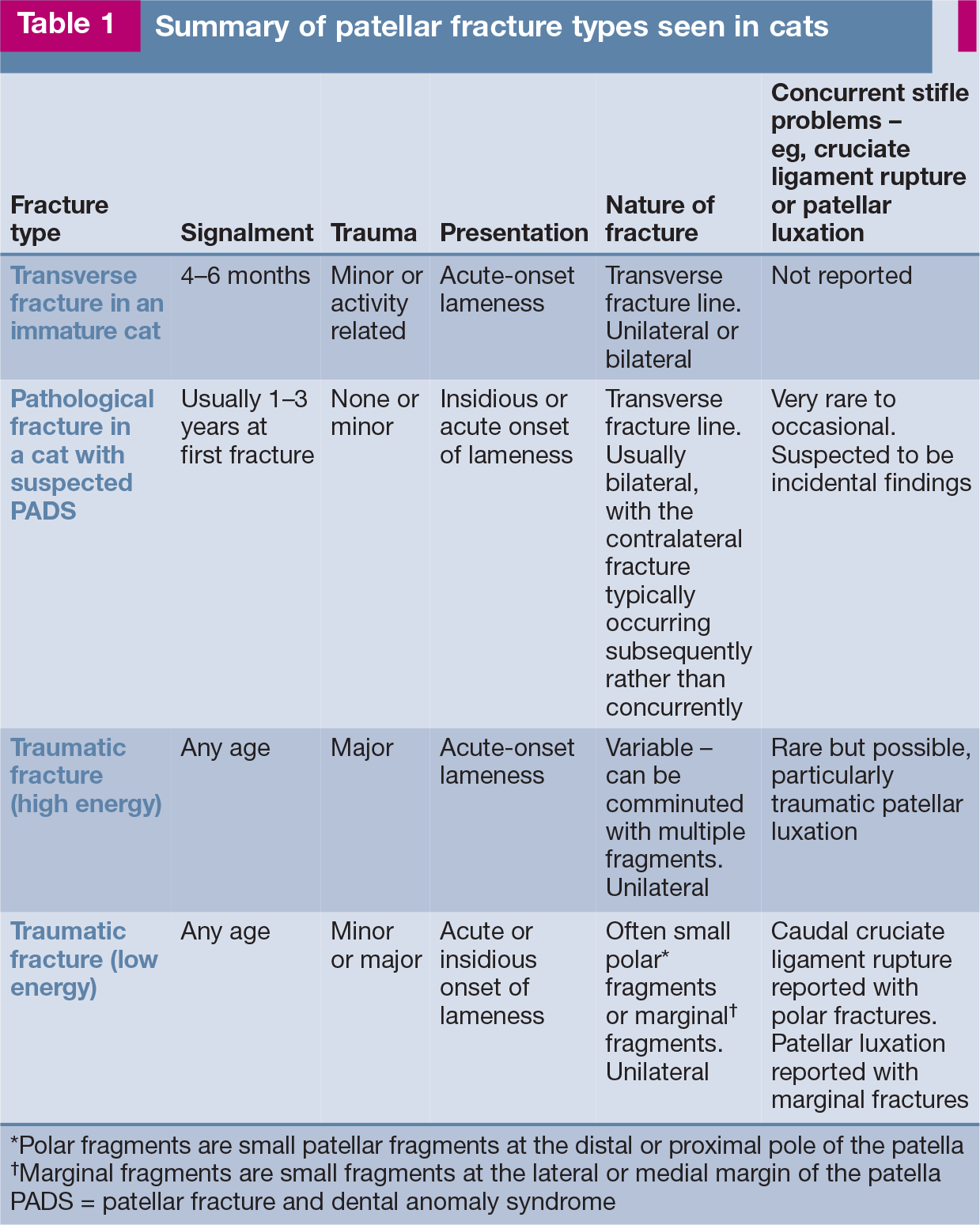
Polar fragments are small patellar fragments at the distal or proximal pole of the patella
Marginal fragments are small fragments at the lateral or medial margin of the patella
PADS = patellar fracture and dental anomaly syndrome
Kittens with transverse patellar fractures
Kittens usually sustain patellar fractures at 4–6 months of age and present with acute-onset lameness. The fracture is usually unilateral 8 and transverse in origin. These fractures may be traumatic due to excessive contraction of the quadriceps (indirect fracture) but there is often a history of vigorous activity or a fall. If the cat does not have dental anomalies, such as persistent deciduous teeth, then PADS is less likely.
The prognosis for healing may be better for these very young cats (<6 months), with healing of the fractured patella documented in two cats in one report. 14 In one of the cats, with a minimally displaced fracture treated conservatively, a radiograph that was taken 11 months after initial presentation showed complete healing of the fracture. The second case, with a displaced fracture, was treated surgically with a circumferential wire; radiographs taken 5 weeks postoperatively showed some narrowing of the fracture gap, and healing of the fracture was demonstrated radiographically 12 weeks postoperatively. These two cases demonstrate that bony union of patellar fractures can be achieved and documented, given a long enough duration of radiographic follow-up. 14
In another report, involving a 6-month-old cat with a unilateral transverse fracture treated with a tension band wire (without a pin), radiographic healing was not apparent at 4 weeks, but the cat’s lameness resolved, and it was considered normal 1 year postoperatively. 8 Pin and tension band wire fixation can also be considered in kittens (Figure 8) and seems to have a lower complication rate than in older cats with pathological stress fractures. 14

Radiographic and intraoperative images of a 4-month-old cat with a transverse patellar fracture. (a) Mediolateral and (b) craniocaudal radiographic views showing a minimally displaced transverse fracture. (c) The intact patellar ligament and (d) the articular surface of the patella exposed during surgery; the cartilage appears to be intact with a small indentation at the site of the fracture (arrow). (e) The fracture was repaired with a small pin and tension band wire. (f) The articular surface following fracture stabilisation. (g) Mediolateral and (h) craniocaudal radiographic views showing the fracture repair with pin and tension band wire. (i,j) Follow-up radiographs at 1 month. The fracture line is still apparent, but the implants are unchanged in position and fracture reduction has been maintained
Healing is slow, even in kittens, and radiographs taken at least 12 weeks postoperatively are recommended to assess for healing.
Transverse patellar fractures
Many cats with simple transverse fractures are thought to be affected by PADS (see box on page 651).9,15,16
As discussed earlier, pin and tension band fracture repair of transverse fractures in cats suspected of having PADS is notoriously unsuccessful (Figure 6),9,11 usually due to further fracturing of the brittle bone and implant pull-out. 9 This technique is therefore contraindicated in these cats. Circumferential sutures or wiring have been reported as having a better success rate. 9 In a biomechanical study looking at patellar fracture repairs in normal (ie, non-PADS) cats, a combination of circumferential and figure-of-eight wires (without a pin) had the overall best performance of the techniques compared, which also included single figure-of-eight wire sutures, single circumferential wires, and conventional pin and tension band wiring. 25
One retrospective study compared the outcome of treatment of nine transverse fractures in a group of six cats. 11 Six fractures were treated surgically and three conservatively. There was breakdown of the surgical repair in4/6 fractures treated surgically. Pin and tension band wire fixation was used for 4/6 surgical repairs, and additional fractures developed and implant failure occurred following fixation in three of these. All six cats, regardless of whether they had conservative or surgical treatment, and despite the failures of surgical fixation, went on to achieve full recovery with normal activity and gait. 11
Because many transverse fractures in cats may be spontaneous and not associated with trauma, 9 the soft tissue, such as the parapatellar fibrocartilage, may be intact and this may help in counteracting the forces exerted by the quadriceps muscles, thereby preventing further displacement. 7 As mentioned earlier, stressed-view radiographs can be used to assess instability and displacement between the fracture fragments (Figures 4 and 5). If fracture fragments are not widely displaced and are stable, and lameness is mild, then conservative management may be the treatment of choice.
For displaced or unstable fractures, the author now recommends treating with the mindset that they are disruptions of the quadriceps tendon. As such, non-metallic sutures are placed in a figure-of-eight or circumferential pattern around the patella (Figure 7), alone or in combination with tibiopatellar sutures. The aim is not to achieve bony fracture union, but to re-establish the quadriceps mechanism. This should enable the cat to weightbear on the affected leg without collapse and to maintain stifle extension. By avoiding the use of pins, the complication rate noted in previous studies should be reduced.9,11

Comminuted fractures
The aims, if possible, with comminuted fractures are to stabilise the fragments against distractive forces such as tension and to restore the articular surface to a smooth contact layer. Very small fragments may need to be removed. The main fragments need stabilising with pin and tension band wire fixation. Very small K-wires (eg, 0.6-0.9 mm) and fine wire that still has some stiffness (eg, 22 or 24 G), but is malleable enough to place without disruption of the fracture fragments, are required (Figure 5). A mini-arthrotomy should be performed to check the reduction of the articular surface.
Longitudinal, longitudinal oblique and marginal patellar fractures
These fracture types are usually associated with patellar luxation and therefore both the fracture and the luxation may need addressing. As the patellar fracture is not under tension from the pull of the quadriceps tendon, the ability to maintain reduction of the fracture fragments is usually good and the prognosis for recovery positive. 13
A longitudinal patellar fracture with luxation of a large medial fragment in a 2.5-year-old cat was treated by reduction of the large medial fragment and lateral marginal patellectomy, with a good outcome. 8
In a separate report, lameness in a young Ocelot that had fallen from a window failed to improve after 3 weeks. 13 Radiographs showed a mid-body patellar fracture displaced laterally, with a radiopaque structure still in the trochlear groove and a small undisplaced chip fracture at the distal pole of the patella. The cat underwent surgery through a combined lateral and medial parapatellar approach. The fibrous tissue was debrided to reduce a laterally displaced fragment and medial and lateral patellar fragments were reduced and stabilised with a 1.4 mm transosseous pin and 22 G wire as a tension band. No surgery was performed on the undisplaced distal pole fracture as it was felt to be stable. The patellar luxation reduction was maintained by leaving the lateral retinaculum open and judiciously closing the medial retinaculum. Closure was initially too tight and repeat surgery was performed to remove some sutures. 13 The polar fracture had healed on follow-up radiography 8 weeks postoperatively, while the main patellar fracture was not healed but remained reduced.
Four further traumatic patellar fractures with simple longitudinal or mildly comminuted longitudinal fracture fragments all treated surgically,7,8,13 either by removal of small fragments or pin and tension band wire stabilisation of larger fracture fragments, 7 have been reported with good outcomes where follow-up was available. Patellar luxation may need to be addressed by specific techniques such as recession sulcoplasty or tibial tuberosity transposition (Figure 4), although this does not seem to have been necessary in the reported cases.
Polar fractures
Small, usually distal fragments are occasionally seen either alone or in combination with other larger fracture fragments.7,13 These have been reported with concomitant injuries such as femoral or tibial fractures or caudal cruciate ligament rupture, 7 and these concurrent injuries will usually need addressing and may be the main cause of lameness. Polar fracture fragments, as they may have little effect on the extensor mechanism or femoropatellar articulation, can safely be resected (Figure 9), although this may not be necessary as conservative management can give satisfactory functional results.7,13 Although non-union of the fragment often persists, this does not appear to cause lameness as long as the extensor apparatus is functional.

(a) Distal polar fracture in a cat with a caudal cruciate ligament rupture. The cat had also sustained a hip dislocation concurrently. (b) The distal polar fragment was removed and the caudal cruciate ligament rupture addressed by placing a lateral fabellopatellar ligament suture
Postoperative rehabilitation
Administering analgesia pre-, intra- and post-operatively and restricting activity in the early postoperative phase are both essential. External coaptation is probably best avoided due to the risk of complications associated with its use and its limited benefit in stabilising the stifle. It is particularly important that the cat is not allowed to jump postoperatively and so restriction for 4-6 weeks to a small crate that is low in height would be recommended. Physiotherapy and hydrotherapy can be useful ways to rehabilitate the cat as healing progresses. 26
Bone healing
In a previous study by the present author of 34 cats, only 1/52 patellar fractures showed radiographic evidence of fracture healing and this was seen on radiographs taken 3 years following surgery. 9 Radiographic evidence of fracture healing in two young kittens has been reported, but again in a slow time span (3–11 months after surgery). 14 This relative lack of radiographic union may be because sesamoid bones produce a fibrous rather than an osseous union. 6 Hence, clinical outcome may be more important than radiographic union in patellar fracture cases.
Key Points
The function of the patella is to protect the tendon of the quadriceps during weightbearing and energetic activity such as jumping. It also plays a vitally important role in the extensor mechanism of the stifle, such that if the patella is fractured, stifle extension is affected.
It is important to check for other traumatic injuries that may be more significant than the patellar fracture. If there is no evidence of a traumatic aetiology, the cat may have suffered a pathological fracture (such as in a cat suspected of having PADS) and should be checked for persistent deciduous teeth or unerupted adult teeth, as well as evidence of concurrent fractures.
Good quality radiographs are usually sufficient to show a fracture, and orthogonal views should be taken in all cases. Stressed views can also assist in decision-making for treatment.
The type and nature of a patellar fracture will guide the decision about which treatment to select. Pin and tension band wiring, for example, is contraindicated in cats suspected to have PADS.
Many patellar fractures in cats can be managed successfully, with the cat returning to good function, even if fracture non-union is the result.
Footnotes
Acknowledgements
Thanks go to the veterinarians and owners who keep the author informed about cats affected with patellar fractures, and to colleagues who have worked with the author, investigating patellar fractures in cats.
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
Supplementary material
The following file is available online:
• Video showing a 4-year-old neutered female domestic short-hair cat with marked lameness (a dropped stifle) associated with a transverse fracture of the right patella. The cat, suspected of having PADS, fractured both patellae at different times and also sustained a transverse tibial fracture.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.