
Abstract
Objectives
The aims of the study was to assess the placement of the V-gel Advanced (V-gel-A) and to evaluate tracheal selectivity during controlled mechanical ventilation, using CT.
Methods
In this prospective clinical study, 20 healthy cats undergoing general anaesthesia for an elective procedure underwent four successive CT scans from the nose to the mid-abdomen: at baseline (no device); after the placement of the V-gel-A, after a controlled mechanical ventilation (CMV) period of 5 mins; and after the placement of an endotracheal tube (ETT). Using both a purpose designed position score and a gas score estimating the quantity of gas in different digestive regions, the position of the V-gel-A and presence of gas in the digestive tract at each step were evaluated. Number of attempts and times required to place the V-gel-A and ETT were recorded and compared.
Results
The V-gel-A was found to be correctly placed, with position scores of 3/5 in six cats, 4/5 in 13 cats and 5/5 in one cat. Imperfect positioning was due to minor axial rotation or incomplete occlusion of the oesophagus by the tip of the device. The gas scores significantly increased after placement of the V-gel-A compared with baseline and after CMV was initiated. Correct positioning of the device was mostly achieved at the first attempt; no significant difference was found in the time required to place V-gel-A vs ETT, nor in the number of attempts (P >0.05).
Conclusions and relevance
The V-gel-A was clinically easy to place and use in both spontaneous and controlled ventilation. The device properly fitted the larynx and was never observed to occlude the airway. However, incomplete occlusion of the oesophagus was frequently observed and may lead to a lack of complete tracheal selectivity.
Keywords
Introduction
Orotracheal intubation is considered the standard of care for airway management in human and veterinary anaesthesia. In cats, this technique is associated with risks ranging from post-anaesthetic discomfort to tracheal laceration. Orotracheal intubation has been identified as a factor of morbidity and mortality in cats.1–4
Laryngeal mask airways (LMAs) have been developed in rabbits, cats and dogs as an alternative to orotracheal intubation. They allegedly reduce risks associated with intubation and facilitate airway management. The first version of the feline specific LMA, the V-gel,1–3,5 was recently replaced by a newer design: the V-gel Advanced (V-gel-A). This latest version is thinner, lacks the dorsal soft cushion and displays a wide ‘bowl’ that takes in the whole larynx, allowing the epiglottis to move freely. 6
The original V-gel has been described as a safe device for feline anaesthesia, and is easier and quicker to place compared with an endotracheal tube (ETT), especially for untrained operators.1–3 It also induces less respiratory discomfort after anaesthesia.2,3 Controlled mechanical ventilation (CMV) has been shown to be effective without leaks at peak inspiratory pressures up to 16 cmH2O. 1 Some clinical complications have been reported, such as upper airway obstruction or desaturation in cats 1 and rabbits, 7 which could be possibly related to the misplacement of the V-gel.
CT has been used in rabbits to assess the placement of the V-gel in the oropharynx7,8 and to monitor secondary gas distension of the stomach after CMV as a sign of poor tracheal selectivity. 7 Incorrect placement of the device was reported in 70–85% of rabbits (ie, misplacement of the device tip in the laryngeal vestibule, lateral deviation, cranially misplaced device sometimes associated with laryngeal compression). 8 This resulted in a decreased airway diameter. In rabbits, an increase in the amount of gas in the stomach was seen after CMV. 7 To date, no tomodensitometric study assessing the placement of V-gel has been published in cats.
The primary aims of this study were to assess the placement of the feline V-gel-A using CT and to evaluate the accumulation of oesophageal and gastric gas before and after CMV. The secondary aim of the study was to compare the duration and number of attempts required to place the V-gel-A and the ETT.
The authors hypothesised that the duration required to place the V-gel-A, as well as the number of attempts, would be significantly shorter than with the ETT, and that the amount of digestive gas would not be significantly affected by V-gel-A placement or CMV.
Material and methods
The Clinical Research and Ethical Committee of the Veterinary School of Nantes approved the study protocol (CERVO-2020-14-V), and the owners gave written consent for inclusion of their cat in the study.
Animals
Healthy cats, American Society of Anesthesiologists (ASA) classification I or II, presented at the Centre Hospitalier Vétérinaire Atlantia (Nantes) for an elective procedure under general anaesthesia were considered for inclusion, until 20 cats completed the study protocol.
The shape of the head was noted as either ‘European’ (eg, domestic shorthair), ‘triangle-shaped’ (eg, oriental cats) or ‘round-shaped’ (eg, British Shorthair). The exclusion criteria consisted of brachycephalic cats (as described in the LOOF [Livre Officiel des Origines Félines] list), history of respiratory or gastrointestinal disease (including gastro-oesophageal reflux or signs of megaoesophagus), body condition score above 7/9, and laryngeal or oropharyngeal abnormality detected during laryngoscopy.
Study design and anaesthetic technique
The study process is presented in Figure 1. After premedication and before undergoing the planned surgical procedure, cats underwent four CT scans to evaluate the positioning and tracheal selectivity of the LMA. Four CT scans of the head, thorax and cranial abdomen were performed: (1) at baseline (CT-0); (2) after placement of the V-gel-A (CT-V-gel-A); (3) after a CMV period of 5 mins (CT-CMV); and (4) after orotracheal intubation (CT-ETT).

Study process and timing of CT scan acquisition: CT-0 = baseline CT without airway device; CT-V-gel-A = CT after V-gel-A placement; CT-CMV = CT after controlled mechanical ventilation with V-gel-A; CT-ETT = CT after ETT placement. CMV = controlled mechanical ventilation; ETCO2 = end-tidal carbon dioxide; ETT = endotracheal tube; IM = intramuscular; IT = inspiratory time; IV = intravenous; PIP = peak inspiratory pressure; V-gel-A = V-gel Advanced
Sedation and CT-0
Food, but not water, was withheld for 12 h before anaesthesia. Cats were sedated with medetomidine 15 µg/kg (Sedator; Dechra), methadone 0.2 mg/kg (Comfortan; Dechra) and ketamine 1 mg/kg (Ketamine 1000; Virbac) administered intramuscularly. When sedated, an intravenous catheter was placed in a cephalic vein. Animals were positioned in sternal recumbency and provided oxygen flow-by (2 l/min) during CT-0 acquisition.
Induction and CT-V-gel-A
General anaesthesia was then induced with alfaxalone 0.1–2 mg/kg IV (Alfaxan; Dechra) and laryngeal desensitisation was performed using lidocaine 2% 0.1 ml (Lurocaine; Vetoquinol). A lubricated (Vet Lube; Docsinnovent) sterile V-gel-A attached to a mainstream capnograph (paediatric sample chamber, BSM-3500; Nihon Koden) was placed according to the manufacturer’s recommendations. 6 When two sizes were appropriate, the larger device was selected. All insertions were performed by the same trained operator (MD, ECVAA resident with previous V-gel insertion experience). The position of the device was considered correct if typical capnography waveforms were observed on the capnogram and end-tidal carbon dioxide (ETCO2) values in the normal range (35–45 mmHg). The V-gel-A was connected to the T-piece of the small animal ventilator (SAV03; Vetronics) breathing system, set in spontaneous ventilation mode. Anaesthesia was maintained with isoflurane (adjusted according to the operating anaesthetist evaluation) in oxygen (1 l/min). The criteria for rescue intubation were as follows: more than five attempts to replace the device; desaturation observed on pulse oximetry (SpO2 <94%) for more than 30 s; severe or sudden tachy- or bradycardia.
The CT-V-gel-A scan was performed on the V-gel-A intubated patient.
Ventilation and CT-CMV
CMV was initiated using the SAV03 ventilator (Vetronics), set at a peak inspiratory pressure (PIP) of 8 cmH2O. Fresh gas flow (FGF) and expiratory time were adjusted to achieve an inspiratory time (IT) of 1–1.5 s and a respiratory frequency ( fR) of approximately 8 breaths/min. If air leakage was heard during inspiration, it was noted and PIP was reduced by 1 cmH2O. Respiratory rate and PIP were adjusted to maintain ETCO2 in the range of 35–45 mmHg. After 5 mins, CMV was stopped and the CT-CMV was performed when spontaneous ventilation had returned.
Tracheal intubation and CT-ETT
The V-gel-A was then removed and orotracheal intubation performed (MD) under direct laryngoscopy, after application of lidocaine 2% 0.1 ml (total dose 4 mg). If necessary, alfaxalone was injected to effect to obtain sufficient relaxation to allow tracheal intubation. Endotracheal tube sizes (2.5–4.5 mm) were chosen at the operator/anaesthetist’s discretion, based on the size of the tracheal inlet. Tracheal placement was confirmed with capnography and the cuff inflated to a pressure of 20 cmH2O. Then the CT-ETT scan was performed.
After completion of the CT-ETT scan, the ETT was left in place and cats were prepared for the planned surgery. No further data were collected.
Monitoring
Capnography, electrocardiogram, pulse oximetry on the ear or on the digits (multiparameter monitor BSM-3500; Nihon Kohden) and oscillometric blood pressure (PetMAP graphic II) were monitored throughout the whole procedure. During CMV, ventilator and capnometry parameters (ie, PIP, fR, ETCO2, IT, FGF) were recorded every minute and audible leaks were recorded.
Data collection
Placement of V-gel-A and ETT
The number of attempts to successfully place the V-gel-A or the ETT was recorded. An attempt was successful if the device appeared symmetrically placed and if a typical rectangular capnogram was observed. A new attempt was counted each time the device required withdrawal and subsequent reinsertion. The time to placement was recorded from the start of insertion until verbal confirmation of successful placement. Occurrence of lingual cyanosis or airway obstruction (ie, audible wheeze or abnormal capnography waves) were noted.
Evaluation of the CT images
The four CT scans ranged from the rostral margin of the nose to the cranial abdomen (including the stomach). A board-certified radiologist evaluated all CT images with a dedicated software (Horos v3.3.6).
The V-gel-A placement was evaluated on CT-V-gel-A. Five qualitative desirable criterions were noted as present (score 1) or absent (score 0). These five criteria were as follows: (1) the adequate position of the distal extremity of the V-gel-A in the oesophageal sphincter; (2) the full occlusion of the oesophagus by the distal extremity of the V-gel-A (ie, the absence of gas between the device and the oesophageal sphincter) (Figure 2); (3) the epiglottis lying freely within the V-gel-A bowl; (4) the absence of axial rotation of the device (ie, preserved symmetry of the device in relation to the sagittal plane assessed in transverse section) (Figure 3); and (5) the preservation of the right to left symmetry of the larynx. These five criteria were summed to generate a V-gel-A position score, with 0 indicating total mispositioning and 5 denoting perfect positioning.
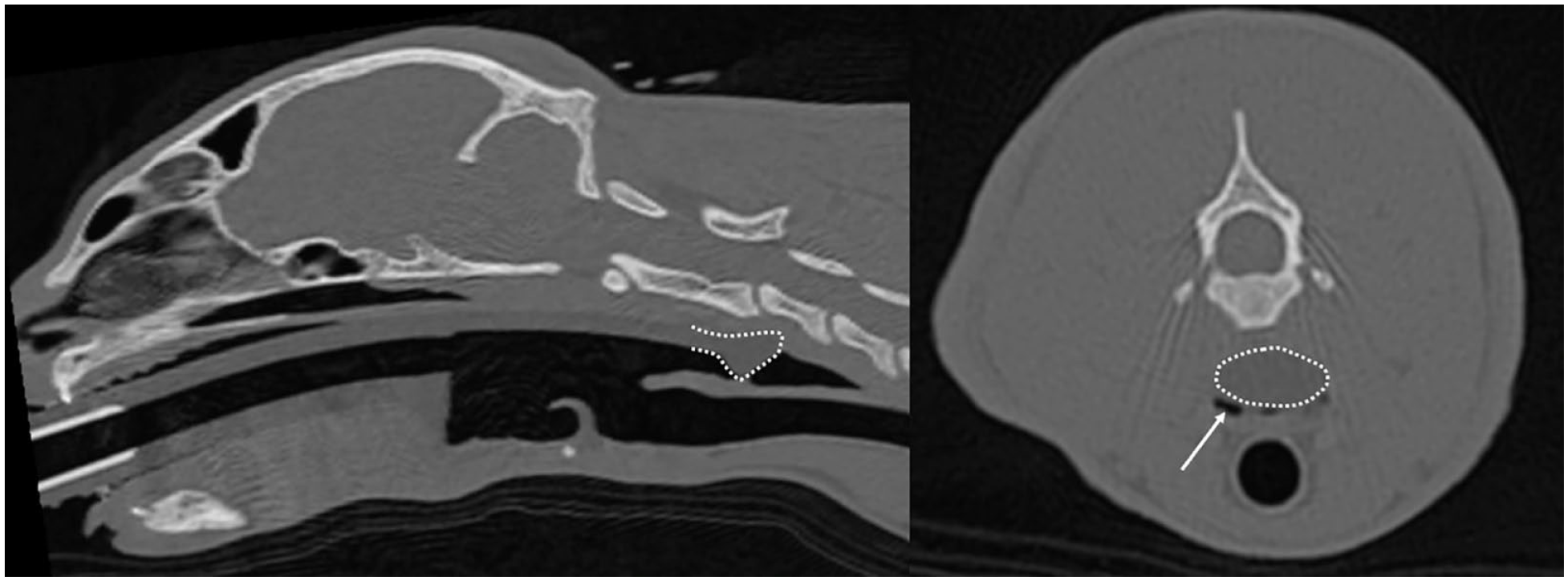
Sagittal and transverse tomodensitometric views of a cat intubated with a V-gel Advanced (CT-V-gel-A). The white dots represent the tip of the device. The tip is seen in the oesophagus, but incompletely occluding it (white arrow)
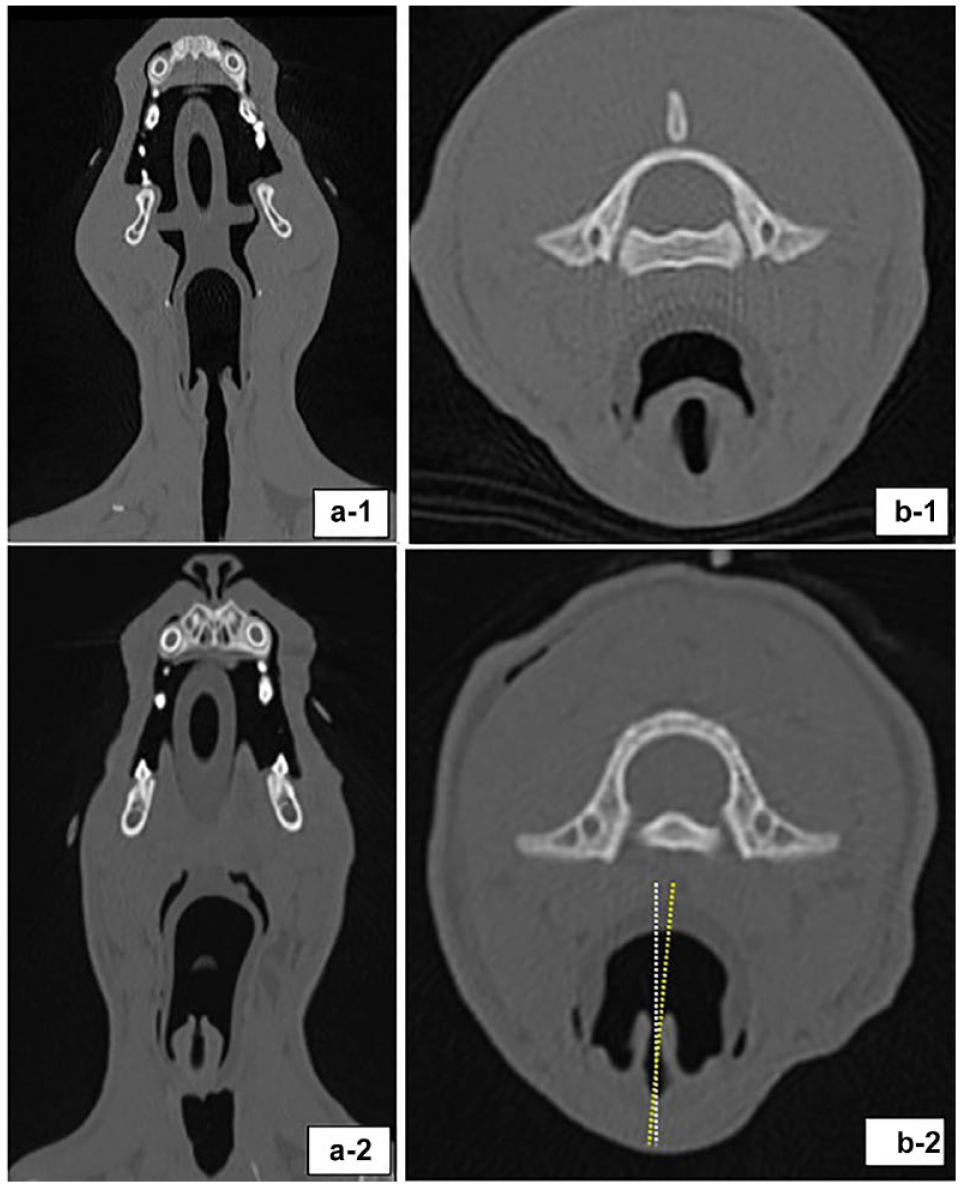
(a) Dorsal and (b) transverse tomographic reconstructions in two cats with a V-gel Advanced: in the first cat (1), the larynx is symmetrical and V-gel-A is not rotated; in the second cat (2), the larynx is rotated in relation to the sagittal axis of the larynx (5.8° on the left)
The degree of axial rotation of the device in relation to the sagittal plane of the larynx was measured. The maximal horizontal distance between the arytenoids, at the cranial edge of the larynx (the width of laryngeal opening), was measured on the CT-0 and CT-V-gel-A scans.
The position of the V-gel-A between the CT-V-gel-A and CT-CMV scans was compared subjectively to ensure that the device did not move during CMV.
For each CT scan, the presence of gas in and degree of distension in both the oesophagus (cervical, cranial and caudal thoracic portions) and the stomach (pylorus and fundus) was subjectively scored from 0 to 3 as follows: 0 = absent; 1 = mild; 2 = moderate; or (3) = marked. A regional gas score was obtained for each of these anatomical regions. The total gas score (0–15) was the sum of the regional gas scores.
The presence of fluid or ingesta within the oesophagus was recorded.
Statistics
This was a pilot study, as no tomodensitometric studies of the V-gel-A in cats had been published at the time of designing the protocol. The sample size was established based on results from previous tomodensitometric studies in rabbits showing misplacement in 8/10 cases 7 or 6/7 cases. 8 A sample of 20 cats was considered sufficient to identify gross mispositioning or lack of tracheal selectivity. This sample size and the study protocol were accepted by the ethical committee.
Statistical analysis was performed using a statistical software program (R Core Team 2019 software; R Foundation for Statistical Computing). Statistics were mainly descriptive. For quantitative data, the Wilcoxon signed-rank test was used, whereas Fisher’s exact test was used for qualitative data. P <0.05 was considered significant. The quantitative data are presented in Tables 3–5 as median (range).
Results
Animals, procedure and complications
A total of 24 cats were recruited for the study and 20 completed the study. Four cats were excluded as a result of inadequate CT scans. The demographic data are presented in Table 1.
Demographic data (sex, breed, age, body weight, BCS, ASA risk, head shape) and surgery performed on the 20 cats included in the study

Data are n or median (range)
ASA = American Society of Anesthesiologists; BCS = body condition score
The tongue appeared cyanotic and congested in four cats after CMV, despite normal SpO2 values and normal cardiovascular (blood pressure and heart rate) recordings.
One cat showed a mild amount of hyperattenuating content within the caudal oesophageal sphincter in all the CT acquisitions, consistent with a small and stable alimentary reflux. Another cat had a mild amount of fluid in the caudal thoracic oesophagus on the CT-0 and CT- V-gel-A only.
Tomographic assessment of position of V-gel-A and tracheal selectivity
Position of the V-gel-A, position scores
On the transverse images of CT-0 and CT-V-gel-A, no significant difference was observed between the maximal latero lateral opening of the larynx (P = 0.29). Position scores are presented in Table 2 and Figure 4.
Results of the evaluation of the V-gel Advanced (V-gel-A) position assessed by CT in 20 anaesthetised cats

Data are n. Five desirable positioning features were assessed as present or absent. Regarding rotation of the device, 12 were rotated in the sagittal plane
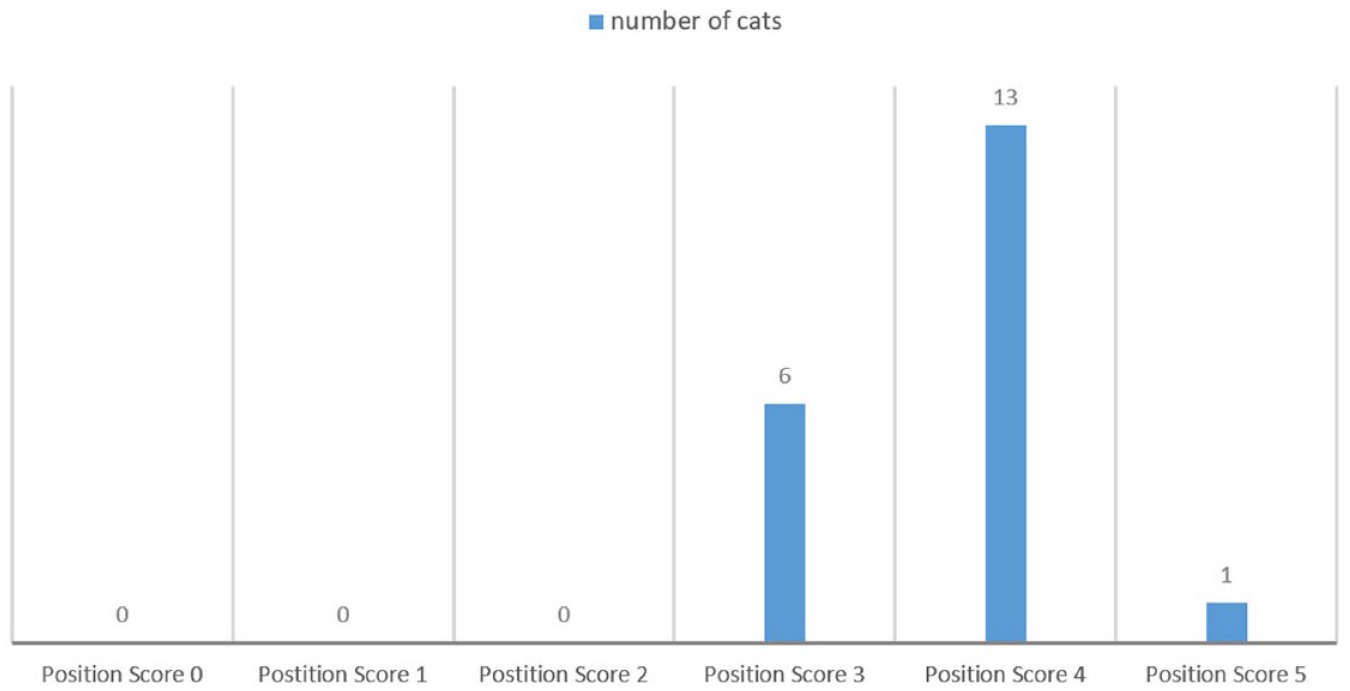
Tomographic position score of the V-gel Advanced (V-gel-A) in 20 anaesthetised cats. Scores could range from 0 (total misplacement) to 5 (perfect placement)
In the position scores, 3/5 criteria were achieved in all cases: the caudal tip of the device was correctly inserted in the oesophageal sphincter, the epiglottis remained free and the larynx was symmetrical. Occlusion of the oesophageal sphincter was not achieved in 13 cats (Figure 2). The device appeared rotated in 12 cats (Figure 3), but rotation remained moderate with a maximum of 10° from the sagittal plane.
A subjective assessment of the V-gel-A position confirmed that the device did not move between successive scans.
CMV was easily and successfully performed in all cats. No audible leaks were detected. Ventilation parameters applied during CMV are presented in Table 3. ETCO2 remained lower than 35 mmHg in five cats despite the decrease of fR to 6 mpm and PIP to 7 cmH2O.
Ventilation parameters applied and recorded in 20 cats every minute during a 5 min controlled mechanical ventilation with the SAV03 ventilator (Vetronics) and using a V-gel Advanced supraglottic airway device

ETCO2 = end-tidal carbon dioxide; FGF = fresh gas flow; IT = inspiratory time; fR = respiratory rate
Gas scores
Total median gas scores obtained for each CT acquisition are shown in Table 4.
Total tomodensitographic gas scores and increases in gas scores obtained in 20 anaesthetised cats

The total score (from 0 [no gas] to 15 [marked gas accumulation]) is the sum of five sub-scores (0-5) obtained from cervical oesophagus, cranial thoracic oesophagus, caudal thoracic oesophagus, pylorus and fundus
Significantly different from CT-0
Significantly different from CT-V-gel-A
Significantly different from CT-CMV
CT-0 = baseline; CT-V-gel-A = after placement of the V-gel-A; CT-CMV = after 5 mins of controlled mechanical ventilation with the V-gel-A; CT-ETT = after endotracheal intubation; V-gel-A = V-gel Advanced
Total gas scores were significantly increased after placement of the V-gel-A compared with baseline (P <0.001). They were significantly increased after the ventilation period of 5 mins with the V-gel-A (P <0.001), but significantly decreased after intubation (P <0.001).
The amount of gas present in the cervical oesophagus after ETT placement seemed reduced in almost all patients. The mean regional gas scores obtained for each CT scan and each region are presented in Figure 5.

Mean regional gas scores obtained in 20 cats based on CT images at baseline (CT-0), after the insertion of the V-gel Advanced (CT-V-gel-A), after 5 mins of controlled mechanical ventilation (CT-CMV) and after endotracheal intubation (CT-ETT). For each of the five regions, a subjective regional gas score was attributed based on the presence of gas and the degree of distension, from 0 (empty) to 3 (marked). A mean regional gas score represents the mean of the gas scores attributed to a selected region in 20 cats for a CT scan
Time to place the devices and number of attempts
The median time between premedication and induction was 29 mins (range 18–82 mins). Alfaxalone 0.2 mg/kg (range 0.1–0.4 mg/kg) was necessary to place the V-gel-A in all cases. The size of the V-gel-A or ETT, number of attempts and time required to place the devices are presented in Table 5. The V-gel-A C3 size was overrepresented (14/20). Rescue endotracheal intubation was never required.
Sizes of the devices used and number of cats receiving it, number of attempts for each device and time of placement for each device

Data are n or median (range)
ETT placement was performed without additional alfaxalone. A single attempt was necessary in 14/20 cats. Prolonged intubation occurred in three cats (at 24, 45 and 59 s) due to marked laryngeal reactivity or technical issues with the laryngoscope light bulb.
No significant difference was found between time or number of attempts required to place the V-gel-A and the ETT (P = 0.47 and 0.53, respectively) (Table 5).
Discussion
The devices were easy to place and safe to use in our study. The manufacturer’s recommendations regarding the sizes of the V-gel-A seemed appropriate. No severe complications occurred. This contrasts with previous studies using the classic V-gel,1,5 which reported airway occlusion, desaturation, obstruction of the device with mucus, displacement of the device and laryngeal obstruction. No displacement or airway obstruction occurred in our study; however, cats were minimally moved after placing the V-gel-A. The authors’ subjective appreciation was that the V-gel-A appeared more stable than the older version, with limited axial rotation or craniocaudal movements over the course of manipulations.
Total position scores were satisfying, with all cats scoring at least 3/5. Inadequate position scores were never associated with immediate safety concern. Specifically, no compression or occlusion of the larynx and no severe displacement of the device were observed. Viscasillas et al 9 reported similar findings with V-gel-A, with adequate fitting of the bowl around the larynx in 46/55 cats. In contrast, a study of rabbits reported that the original version of the V-gel partially occluded the larynx in most patients. 7 Similar to previous results in rabbits and capybaras,7,8,10 an adequate capnogram trace did not guarantee perfect positioning of the device.
Axial rotation of the device (12/20 cats) and incomplete occlusion of the oesophagus (13/20 cats) were common. The rotation was minor in all cases (<10°) and had no significant consequences on the larynx symmetry or the airway diameter and the epiglottis remained free in the bowl. Viscasillas et al 9 also reported an incomplete oesophageal occlusion in 43/55 cats. This may increase the risk of aspiration and decrease tracheal selectivity during mechanical ventilation. This is concerning, as use of LMA may promote gastro-oesophageal reflux in humans11–14 and cats.4,15
Total gas scores were always mild or moderate, in all cats (range 0–9/15), which suggests limited accumulation of gas in the digestive tract.
Manipulation and placement itself produced air trapping in the upper digestive tract, especially in the cervical oesophagus (Figure 5). Similar observations were made in capybaras after placement of a human LMA. 10
In the authors’ experience, gas in the oesophagus is also commonly observed on CT images after endotracheal intubation in cats and has been described in intubated dogs. 16 Air trapping due to manipulation is possible with any device but could be more pronounced with V-gel-A vs ETT. In our study, total gas scores significantly decreased after removal of the V-gel-A and subsequent orotracheal intubation (Table 4, Figure 5).
Inadequate permeability of the airway with LMA may expose the patient to upper digestive tract insufflation during positive pressure ventilation. Severe gas distension may result in cardiovascular and respiratory dysfunction and promotes gastro-oesophageal reflux. 17 In order to evaluate the occurrence of this possible undesirable effect, we evaluated gas collection on the digestive tract using a custom-made scoring system. We used a subjective semi quantitative evaluation of gas accumulation based on regional subjective scores of gas, which was added to yield a total gas score. In rabbits, Wenger et al 7 used a quantitative technique allowing the calculation of gastric gas volume based on CT images. Although our technique is not quantitative, it allows a more detailed regional analysis of gas trapping patterns.
Median total gas scores significantly increased during the 5 mins of CMV from 4 (range 1–7) to 6 (range 3–9) out of 15 (Table 4). Gas was collected preferentially in proximal regions of the digestive tract, as shown in Figure 5. Incomplete occlusion of the oesophagus by the tip of the V-gel-A may have promoted the lack of tracheal selectivity during CMV. In cats, Prass et al 1 made similar observations of gastric gas after ventilation with the classic V-gel.
Gastric gas is commonly detected in both anaesthetised and sedated dogs and cats (14–20%)16,18 without noticeable consequences. Severe gas distension may result in both cardiovascular and respiratory dysfunction and can promote gastro-oesophageal reflux. 17 In our study, the surgeon did not observe bloating, nor any other associated clinical consequence; however, the duration of CMV was very short in this study and does not mimic a true clinical situation. Prolonged or more aggressive ventilation (increased PIP or respiratory rate or flow) may exacerbate the accumulation of gas in the digestive tract. Further studies are warranted to evaluate this adverse effect.
In our study, V-gel-A placement was successfully achieved at the first or second attempt for the majority of cats (17/20). This is consistent with previous results obtained using the classic V-gel. 5 Three patients required three attempts to correctly insert the V-gel-A, but no further complications were encountered.
No differences were found in the times required to place the V-gel-A and ETT in our study. This is surprising as previous reports showed a significantly shorter time to place a V-gel compared with ETT in cats.2,3 This could be attributed to the operator’s experience, as in previous studies, untrained veterinary students were placing the devices. 3 It is likely that the time and ability to correctly place a V-gel is less experience-sensitive than the ability to perform endotracheal intubation in cats, as in humans. 19 The method used to measure the duration of device placement may also have contributed to minimising the difference between the V-gel-A and ETT. Van Oostrom et al 2 measured the time from induction to first acceptable reading on a capnogram, whereas we measured the time from starting device insertion to satisfactory capnogram waveforms. The time required for induction, positioning and laryngoscopy was not recorded in our study. This creates a bias reducing duration of orotracheal intubation. Similarly, confirmation of V-gel positioning requires an extended observation of capnogram shape, which introduces a bias, increasing the duration of V-gel-A placement. Finally, the endotracheal intubation conditions of the study may not accurately reflect clinical practice, as patients received isoflurane before tracheal intubation.
ETCO2 was in the range of 32–47 before initiating CMV and returned to normal values after discontinuation of CMV. During CMV, most cats developed rapid hypocapnia even when subjected to the usual ventilation parameters for the species. This contrasts with previous reports of LMA use in spontaneously or mechanically ventilated cats4,20 and rabbits.21,22 Reduction of respiratory rate (down to 6 mpm) and PIP (down to 7 cmH2O) was necessary to contain hypocapnia. Reduced airway resistance due to the larger internal diameter of the LMA (vs ETT) may have promoted a larger than expected tidal volume with the pressure cycle ventilator, resulting in hypocapnia. 20 Alternatively, the initial ventilator setting (PIP 8 cmH2O) may not have been adequate, considering recent findings that indicated that PIP >7 cmH2O leads to lung overinflation in cats. 23 Direct observation of the chest did not suggest lung over expansion, but this hypothesis would be confirmed with a tidal volume measurement using spirometry. The inspiratory times used here (up to 1.8 s) were longer than usually prescribed in cats. As the respiratory rate was decreased to limit hypocapnia, we tolerated this prolonged inspiration to keep the inspiration/expiration ratio higher than 1/5 in our cats. The inspiratory time could have been decreased by increasing FGF; however, our experience with pressure-cycled ventilators in small animals is that increasing FGF to a greater extent often leads to a premature trigger of the expiration, due to excessive inspiratory peak pressure created by the artificial array resistance.
Cyanosis of the tongue is commonly reported with LMA use in cats 3 and rabbits. 7 It is thought to result from venous congestion due to tongue compression and is not associated with arterial desaturation. Clinical signs of venous engorgement were observed in four cats presenting tongue cyanosis in our study. Sagittal CT images revealed compression of the base of the tongue caused by the ventral wings of the V-gel-A. No further complications were noted after removal of the V-gel-A, but consequences after longer procedures are unknown.
The homogeneity of our population (young healthy domestic shorthair cats) limits the external validity of our findings. The small number of cats and their fit and healthy profile reduced the likelihood of encountering a difficult airway access situation. Our results may not be extrapolated to cat populations with unusual head shapes (eg, Orientals, Maine Coon or brachycephalic breeds). We only tested V-gel-A sizes C2, C3 and C4 as they were indicated for our patients.
Given the relatively small sample size (20 cats), there was a decreased likelihood of encountering rare but severe complications such as hypoxemia or airway occlusion. The study was not powered to detect these complications.
All gas scores were attributed by a single radiologist who remained blind to the clinical aspects of the procedure (ie, number of attempts, duration of intubation and ventilation parameters). However, the radiologist could not be blinded to the device used.
Spirometry was not used in this study, which decreased sensibility to detect leaks and did not allow measurements of ventilation parameters, such as applied tidal volume.
Conclusions
In our cohort of 20 young healthy cats, blind positioning of the V-gel-A was adequate and allowed safe preservation of airway patency. This supports the use of this device in situations where tracheal intubation is debatable (mainly, unexperienced operator, short minor procedures, repeated short periods of anaesthesia, etc). However, incomplete occlusion of the oesophagus was frequently observed and raises concerns regarding airway protection, especially when reflux is at a higher risk. Positive pressure mechanical ventilation through the V-Gel-A was possible and efficient, allowing short-term rescue ventilation; however, our results might suggest a lack of tracheal selectivity, raising concerns about the prolonged use of positive pressure ventilation with the device. Studies addressing digestive gas accumulation over longer periods of mechanical ventilation are required to bring more information about the safety of prolonged use of the V-Gel-A for this purpose. Meanwhile, tracheal intubation should remain the standard of care for airway control and mechanical ventilation, especially in the hands of experienced operators.
Footnotes
Acknowledgements
The authors would like to thank Julien Brune for his help for the study design; Julien Brune, Sophie Segond and Magali Gutierrez for acquisition of the CT scan images; Adrien Maggiar for his participation in recruiting subjects; and Maha Abunemeh and Bernadette Guirguis for their assistance in proofreading.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.