
Abstract
Objectives
Airway management during anaesthesia in cats is always a demanding task and is associated with several complications. The aim of this study was to evaluate the practicability and complications during feline-specific laryngeal mask placement in anaesthetised cats as an alternative to endotracheal intubation.
Methods
In this prospective clinical study, laryngeal masks were placed in 148 anaesthetised cats. Success of placement was evaluated by capnography.
Results
Placement was possible at the first attempt in 136 cats, at the second attempt in eight cats and at the third attempt in one cat. In one cat, placement was not possible. Two cats were excluded. Failure to position the laryngeal mask at the first attempt was not different between laryngeal mask sizes (P = 0.313) or positioning during placement (P = 0.406). In nine cats, the laryngeal mask dislocated during the procedure. Dislocation occurred more often in the dorsal position than in the sternal (P = 0.018) and right lateral positions (P = 0.046). Mucous obstruction of the laryngeal mask occurred in one of these cats and regurgitation in another. Material-related issues, such as disconnection of the parts of the laryngeal mask and leakage of the balloon, were observed in 2/8 laryngeal masks.
Conclusions and relevance
The placement of a feline-specific laryngeal mask was easy to perform. In about 7% of the cases, replacement of the device was required due to mispositioning or dislocation. Full monitoring, including capnography, should be provided to uncover dislocation and airway obstruction immediately.
Introduction
According to the Association of Veterinary Anaesthetists guidelines, one of the major responsibilities of the anaesthesiologist in the management of the anaesthetised patient is the maintenance of a patent airway to avoid airway obstruction and maintain adequate oxygenation and ventilation. 1 Endotracheal intubation is considered the standard method to secure the airways in cats. An increased odds ratio of perioperative mortality has been described in intubated cats during and after a minor procedure vs non-intubated cats or intubated cats during major procedures. 2 These complications, which lead to increased mortality, include laryngospasm and laryngeal oedema, tracheal irritation and rupture, tracheal stricture and trauma to the arytenoids, and have been mostly described in case reports and case series.3–6
Supraglottic airway devices were first developed for humans as an alternative to endotracheal intubation. 7 A review of human studies has proven a lower incidence of coughing and laryngeal spasm during and after laryngeal mask placement, compared with endotracheal intubation. 8 Laryngeal masks from human medicine have also been used and evaluated in veterinary patients. Some authors have described difficulties in achieving a safe seal without over-inflation of the cuff and trauma to the larynx and its cartilage. 9
Feline-specific laryngeal mask airway devices have been developed and are now marketed for use in cats under the brand v-gel (Docsinnovent).10,11 This supraglottic airway device has been specifically designed according to the anatomical situation of the feline larynx. It consists of a non-inflatable cuff that forms a seal around the laryngeal inlet and an inflatable dorsal pressure adjuster to increase seal pressure. 12 Furthermore, delivery of anaesthetic agents in oxygen-enriched gas is necessary for the safe administration of inhalants during maintenance of anaesthesia. 13 A study in cats showed decreased leakage during the use of the v-gel, which makes this device safer than face masks. 11
To date, the practicality and success rate of placing the feline-specific laryngeal mask airway device and complication rates during placement have not been described in depth. The aim of the study was to investigate the success of placement and complications during v-gel placement and maintenance in anaesthetised cats.
Material and methods
Animals
The study protocol was approved by the Ethics Committee of the Centre for Clinical Veterinary Medicine, LMU Munich (number 17-09-10-13).
Cats of American Society of Anesthesiologists (ASA) status 1–3 were included in the study. In total, 148 client-owned cats, anaesthetised for diagnostic or therapeutic procedures, were available for the study. One cat had to be excluded owing to massive swelling of the larynx, which was observed during laryngeal examination before v-gel placement, and one due to severe salivation after premedication.
Finally, 146 cats with a median age of 11.0 years (range 0.5–17.0) and weighing 4.4 kg (range 2.3–7.0) were enrolled in the study. Fifty-one cats were female spayed, 42 male castrated, 39 female intact and 14 male intact. Median ASA status was 2 (range 1–3).
Laryngeal mask
A feline-specific laryngeal mask, designed according to the anatomy of the feline pharyngeal area (v-gel) was evaluated in this study. The size of the v-gel was chosen depending on the body weight of the patient and according to the manufacturer’s instructions (Table 1). Size 3 and 4 are both recommended for 3–5 kg body weight. However, v-gel size 4 has a longer piece between the connecting part for the breathing system and the laryngeal part. After each application, the v-gel was cleaned and autoclaved according to the manufacturer’s instructions.
Success of placement of the feline-specific laryngeal mask (v-gel) in 146 anaesthetised cats

C1–C6 = Different sizes of the v-gel used in the study
Anaesthesia and procedures
The ASA status of the cats was determined according to the patient history and the preanaesthetic examination. Anaesthesia protocols were chosen at the discretion of the anaesthetist. After placement of a venous catheter, cats were intravenously premedicated (Table 2). Preoxygenation was performed with a face mask for 3 mins, if tolerated. Thereafter, 26 cats were intravenously induced with alfaxalone (0.5–4.0 mg/kg [Alfaxan; Jurox]) and 118 with propofol (2.5–9.0 mg/kg [Narcofol; cp-pharma GmbH]). The laryngeal mask was placed in two cats without further induction (Table 2). Subsequently, all cats were connected to a coaxial rebreathing system receiving oxygen. Anaesthesia was maintained with inhalant anaesthetic in oxygen in 117 cats, and with intravenous anaesthesia in 10 cats. Owing to the short duration of anaesthesia, medication for maintenance was not required in 19 cases. Patients were breathing spontaneously during the placement of the v-gel and during the following anaesthesia. Besides clinical monitoring, electrocardiogram, non-invasive blood pressure, end-tidal CO2 and SpO2 were monitored using a multiparameter monitor (Nihon Kohden BSM - 2301K).
Anaesthetic drugs for 146 cats before during feline-specific laryngeal mask (v-gel) placement and for maintenance of anaesthesia

Cats were anaesthetised for radiation therapy (n = 113), skin biopsy (n = 10), ultrasound examination (n = 9), bronchial lavage (n = 3), bone marrow biopsy (n = 3), urinary catheter placement (n = 2), electromyography (n = 1), otoscopy (n = 1), radiographic examination (n = 1), colonic irrigation (n = 1), placement of a thoracic drain (n = 1) and placement of a central venous catheter (n = 1).
V-gel placement and monitoring
Prior to placement of the v-gel, a visual examination of the larynx with a laryngoscope, performed in a similar manner as before intubation, was undertaken in order to exclude severe laryngeal pathology. The lubricated laryngeal masks were placed blindly, as instructed in the user manual. After placement, the standardised cuff of each v-gel size was inflated with 3 ml air and fixed with a tight gauze bandage material around the neck, as instructed by the manufacturer.
Investigated parameters
Successful placement of the v-gel in its proper position was determined by a sufficient capnography curve provided by the multiparameter monitor. An additional leak test was not performed. Misplacement, dislocation and subsequent attempts to correct the positioning of the v-gel, and further device-related adverse events and complications were documented.
Statistical analysis
Data were evaluated with commercially available statistical software (GraphPad Prism 5; Graph Pad Software). Normality was tested for with the D’Agostino and Pearson omnibus test. Normally distributed data were presented as mean ± SD. Non-normally distributed data were reported as median (range). A χ2 test was used to compare the success of placement with different sizes of v-gel and complication rates.
Results
Placement of the v-gel was possible in 145/146 cats (Table 1). In the cat with unsuccessful placement, neither airflow nor a capnography curve were observed, and orotracheal intubation was used to secure the airways. V-gel size 1 was used in one cat, size 2 in one cat, size 3 in 49 cats, size 4 in 30 cats, size 5 in 51 cats and size 6 in 14 cats. According to the planned procedure, cats were placed in different body positions during application of the v-gel (Table 3). Success of placement was not different between v-gel sizes (P = 0.850) nor between body position during insertion (P = 0.919).
Positioning of 146 cats during feline-specific laryngeal mask (v-gel) placement

The median number of attempts for sufficient placement was 1 (range 1–3). Placement of the v-gel was possible during the first or second attempt in all but one cat (Table 3). Failure to position the v-gel at the first attempt was not different between v-gel sizes (P = 0.313) nor position during placement (P = 0.406). Coughing was observed in 17 cats during insertion.
Maintenance of anaesthesia
During the following procedure, most cats were positioned in lateral recumbency. According to the procedure, dorsal, sternal and a combination of these recumbencies were also applied (Table 4). In nine cats, the v-gel dislocated during the procedure and was replaced in four cats by manipulation of the v-gel. In the remaining five cats, the v-gel could not be replaced by manipulation of the laryngeal mask and it was removed. These cats were intubated thereafter (Figure 1). Mucous obstruction of the v-gel occurred in one of these cats and regurgitation in another. Dislocation occurred significantly more often in the dorsal position compared with the sternal (P = 0.018) and right lateral positions (P = 0.046; Table 4).
Position of 145 cats after successful placement of the feline-specific laryngeal mask (v-gel) during anaesthesia

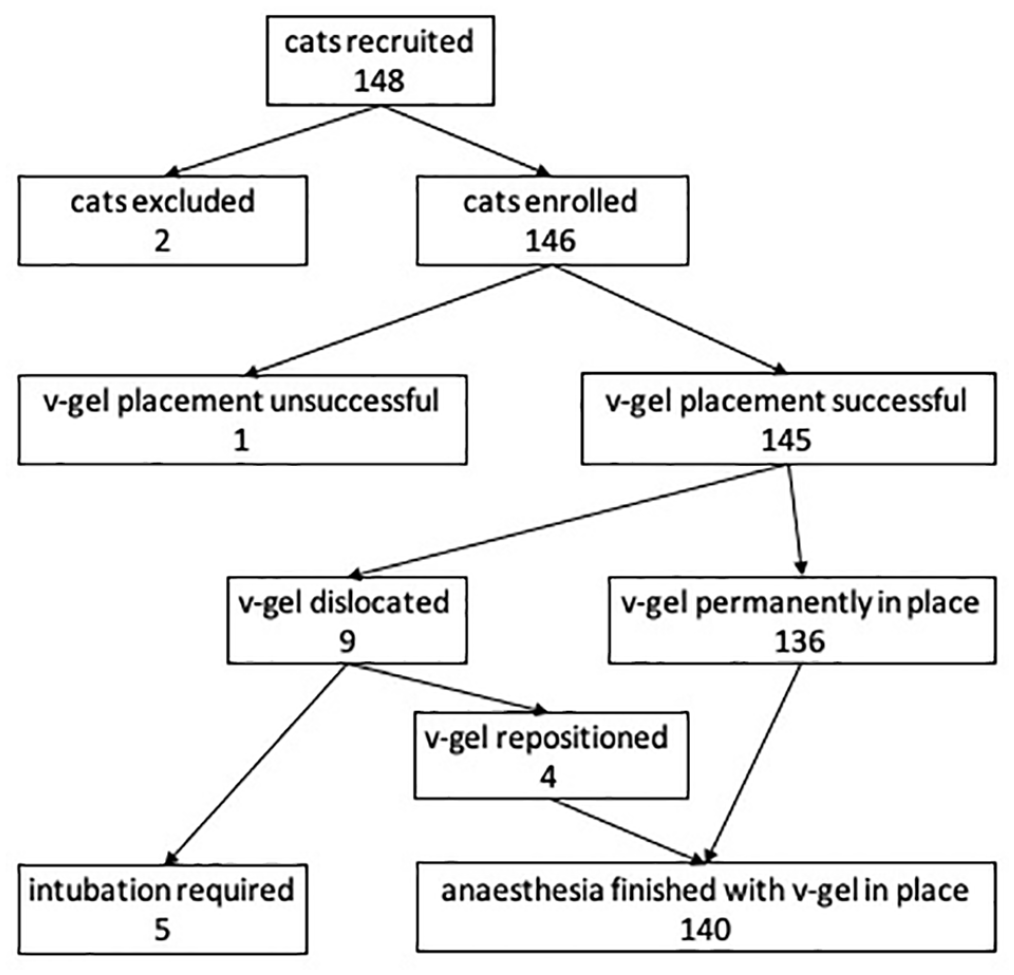
Overview of 148 cats recruited for feline-specific laryngeal mask (v-gel) placement
Material failure
Laryngeal masks were used a median of six times (range 1–21) during the study period. Material-related issues were observed in 2/8 v-gel laryngeal masks used in the study. In one of the laryngeal masks, the connecting piece to the anaesthesia tubing system disconnected from the rest of the laryngeal mask during the sixth application, but the mask could be used further (v-gel size 3). In another mask (size 6) the balloon developed a leak after the fourth application and the mask had to be discarded.
Discussion
Insertion of the v-gel laryngeal mask into the correct position was possible during 1–3 attempts in all cats except one. In another feline study with a small number of cats, 14/15 v-gels were successfully placed in cats at the first attempt. 14 In the present study, the v-gel had to be removed in nine cases owing to dislocation or obstruction. Similarly, 1/15 cats in the previously published study showed signs of upper airway obstruction after the insertion of v-gel. 14
After successful placement, the v-gel had to be removed from two cats owing to the accumulation of mucous and regurgitation. The use of a human laryngeal mask in kittens is associated with a higher incidence of gastro-oesophageal reflux than with endotracheal intubation. 15 Interestingly, another study found a higher incidence of gastric reflux in cats during controlled mechanical ventilation using endotracheal intubation vs laryngeal mask airway without leading to pulmonary aspiration. 16 In three cases in the present study, the v-gel was dislocated and caused an obstruction of the airway, noted by the absence of the capnography curve after changing recumbency. Airway obstruction is one of the major risk factors of peri-anaesthetic death.17,18 The standard management to avoid this complication is endotracheal intubation. This can be associated with an increased risk of anaesthetic death in cats during minor procedures. In the CEPSAF study (Confidential Enquiry into Perioperative Small Animal Fatalities), 148/175 cats that died in the perioperative period were intubated and 27 were not intubated. 2 Other described complications associated with endotracheal intubation in cats are tissue swelling, tracheal rupture or tears of the arytenoid cartilage.3,5,19,20 Furthermore, laryngeal stridor during recovery from anaesthesia has been reported in 6/10 anaesthetised and orotracheally intubated cats. 11 Therefore, both techniques – orotracheal intubation and the use of laryngeal masks – are associated with upper airway complications and a risk of reflux in cats. In human medicine, a significantly lower incidence of complications (laryngeal spasm and coughing during emergence, and hoarse voice) was proven when managing the airway with laryngeal masks compared with endotracheal intubation. 8
As the v-gel does not seal the trachea, the device can increase the risk of aspiration, especially in patients undergoing dental procedures or in patients with an increased risk of gastro-oesophageal reflux. The instruction manual states that the specific formed tip could prevent aspiration after reflux with its position forming a seal in the oesophagus. 21 In both human and feline studies it is suggested that gastro-oesophageal reflux could be present, but aspiration is rarely seen and as such aspiration does not occur with a higher incidence in patients managed with laryngeal masks vs endotracheal tubes.8,15,16 However, the effect of the v-gel on reflux and risk of aspiration requires further examination.
Using the v-gel is a faster technique to secure the feline airway than endotracheal intubation. When performed by inexperienced personnel, it is easier to adequately place the v-gel laryngeal mask than to perform endotracheal intubation. 10 Recumbency during the insertion of the v-gel significantly influenced the correct placement. 10 In the present study, no difference in failure to place the v-gel successfully was observed between the different body positions during placement. The position of the v-gel only had to be corrected in two cats after changing from sternal to dorsal recumbency (Table 4).
Positioning of the v-gel can be performed at a more superficial level of anaesthesia than insertion of an endotracheal tube. 14 In the present study, 17 cats coughed during insertion of the v-gel. These cats received a significantly lower dose of propofol during induction of anaesthesia compared with non-coughing cats (coughing cats: 3.0 mg/kg [range 2.5–5.0]; non-coughing cats: 4.0 mg/kg [range 2.5–9.0]; P = 0.002). No difference between the choice of the induction agent was observed (alfaxalone or propofol; P = 0.564) (Table 2). Premedication with midazolam or butorphanol was not associated with an increased incidence of coughing during v-gel insertion (P = 0.214). Opioid premedication, in general, also did not influence incidence of coughing during laryngeal mask placement (P = 1.000).
Insertion of a laryngeal mask with an insufficient depth of anaesthesia has been described as causing a laryngeal spasm in cats. 22 In the present study, laryngeal spasm was not observed, even if the lower dose of propofol suggested a more superficial level of anaesthesia. The level also depended on the choice and dose of premedication.
Even if insertion of the laryngeal mask was performed at a more superficial level of anaesthesia, adaptation of the depth of anaesthesia may be required, especially in surgical patients. If the v-gel laryngeal mask is used for controlled mechanical ventilation with inspiratory pressure up to 16 cmH2O, surprisingly, it shows significantly less leakage compared with endotracheal intubation. 14
Dorsal recumbency was more prone to dislocation of the laryngeal mask. This could be caused by gravity or lever action of the anaesthesia tubing system. However, the patient was always disconnected from the system during positioning. As placement of the v-gel was never performed in dorsal recumbency, dorsal recumbency during maintenance was always associated with a previous change in position, which also comes with a risk of dislocation.
The abovementioned issue with the material (connector disconnection) in one v-gel was solved by reconnecting the connecting piece to the laryngeal mask, which was reconnected to the tubing system. No leakage was detected after reconnection to the tubing system. The balloon leakage was probably caused by superficial injury of the mask by the cat’s teeth.
The present study had some limitations. Different anaesthetic protocols were chosen at the discretion of the anaesthetists. This could have influenced the first attempt success rate. Additionally, the placement of the v-gel was mostly performed without using supporting staff, which could influence the first attempt success rate. Future studies should investigate the influence of supporting staff on first-attempt success rates during the placement of a v-gel. Laryngoscopy was performed before placement of the laryngeal mask, which is not recommended during routine use of a laryngeal mask. The aim of the laryngoscopy was to discover laryngeal pathology and to avoid additional risk to the patient, which may have influenced the results vs a no-laryngoscopy procedure.
Furthermore, the body position of the cat was changed during some procedures, which could also have had an impact on the laryngeal mask dislocation rate. Leak tests, as well as ventilation, were not performed after placement. To assess performance of the v-gel during mechanical ventilation, additional studies are required.
Conclusions
Placement of the v-gel supraglottic airway device was easy to perform. Misplacement, as well as dislocation, occurred rarely in the study population during the medical procedures. In some cases, it was necessary to adjust the position. Coughing was seen in some cases and was most likely due to a low level of anaesthesia. Full monitoring, including capnography, should be provided after induction and during maintenance of anaesthesia to monitor for dislocation of the laryngeal mask, especially while changing the position of the patient. Owing to a risk of dislocation of the laryngeal mask of about 6%, recommendations to carefully monitor capnography and airflow during anaesthesia and application of the laryngeal mask, as provided by the manufacturer, are supported by the study.
Footnotes
Conflicts of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee, while not specifically required for publication in JFMS, was nonetheless obtained, as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore, additional informed consent for publication was not required.