
Abstract
Objectives
The aim of this study was to determine the maximal endotracheal insertion length by measuring the larynx to carina (L–C) distance by means of CT. An additional objective was to establish certain anatomical landmarks to optimise the process of endotracheal intubation (ETI).
Methods
Head, neck and thoracic CT images from adult cats at a single referral hospital between 2013 and 2020 were retrospectively evaluated. After standardising and identifying key markers (larynx, carina and first rib) the L–C, larynx to first rib (L–1R) and first rib to carina (1R–C) distances were measured.
Results
Forty-five adult cats were enrolled in the study, from which a total of nine different breeds were identified. The L–C distance was 14.3 ± 1.1 cm. This was longer in male (14.7 ± 1.1 cm) than in female cats (13.5 ± 0.7 cm). The first rib (1R) was 8.8 ± 0.7 cm from the larynx and the mean 1R–C distance was 5.4 ± 0.7 cm. The carina was found within the fifth intercostal space in 93.3% (n = 42) of the cats.
Conclusions and relevance
The process of ETI in adult cats may be guided by using the L–C and L–1R distance for a maximal and optimal endotracheal tube introduction, respectively. In addition, the maximal insertion length may be guided by estimating the position of the carina parallel to the fifth intercostal space.
Introduction
Endotracheal intubation (ETI) is a routine procedure during anaesthesia that refers to the placement of an endotracheal tube (ETT) into the trachea. ETI will facilitate a patent airway, delivering oxygen and inhalant anaesthetic agents, and providing invasive mechanical ventilation. 1 ETI is not without risks; misplacement of the ETT at the vicinity of the larynx may lead to dislodgment of the device and/or laryngeal damage. 1 Insertion caudal to the carina may result in endobronchial intubation (EBI). Other complications associated with this technique include oesophageal intubation, aspiration pneumonia, ETT kinking during maximum neck flexion, blockage in the presence of mucous and lodgement to the larynx during extubation. Tracheal rupture has also been reported, which is commonly associated with cuff over-inflation, ETT misplacement and failure to deflate the cuff during repositioning or extubation. Tracheal tears commonly affect not only the cervical region, but may also appear intrathoracically, which typically have a poorer prognosis the closer they are to the carina.1–8
Several methods have been described in veterinary medicine to select the appropriate ETT diameter, including tracheal palpation, measuring the distance between nares or measuring the tracheal internal diameter on a lateral thoracic radiograph.9,10 However, none of these strategies would prevent misplacement of the ETT in the vicinity of the larynx or EBI. In human medicine, methods to determine the optimal length of ETT insertion have been studied. These are based on topographic landmarks, cuff palpation, bronchoscopy, continuous lung auscultation and predicted equations according to the patient’s height.11–13
The main objective of this study was to measure the distance from the larynx to the carina, to determine the maximal ETT insertion length in adult cats by using CT. Secondary objectives were to find anatomical references for both determining the optimal length of ETT insertion and identifying the position of the carina using external landmarks.
Materials and methods
Ethical approval was granted by the university’s Social Science Research Ethical Board (reference number SR2020-0031).
In this retrospective descriptive study, all CT images acquired at our institution between 2013 and 2020 were reviewed. Only CT studies from client-owned cats presented to our institution that underwent head, neck and thorax CT scans were included. From this population, all CT scans of cats with anatomical abnormalities on the region of interest, or cases missing relevant clinical data such as breed, age, sex or body weight (BW) were excluded from the study.
An 80-slice multidetector CT scanner (Canon Aquilion One; Toshiba Medical Systems) was used to acquire the images. Cats were positioned in sternal recumbency, perpendicularly to the isocentre of the CT scan with the head in a neutral position and the forelimbs extended cranially. The imaging protocol included the axial images of the head, neck and thorax. The CT images were obtained as Digital and Communication in Medicine (DICOM) files and reconstructed with soft tissue and lung windows.
Studied variables included larynx to carina (L–C), larynx to first rib (L–1R) and first rib to carina (1R–C) distance (in cm). The position of the carina in respect to the intercostal spaces (intersection between both landmarks in the sagittal plane) was used as an anatomical reference to estimate the location of the carina. Additional variables included breed, age, sex and BW. The measuring point for the larynx was considered as the midpoint of the laryngeal vestibule when the most rostral aspect of the arytenoid cartilage appeared in a transverse plane (Figure 1a). This was confirmed by identifying the arytenoid processes in a dorsal view (Figure 1b) and in a sagittal view (Figure 1c). The carina was identified as the most caudal midpoint of the tracheal lumen, where the trachea bifurcated in two main bronchi (Figure 2). The position of the carina was correlated with an intercostal space by assessing the intersection between both landmarks in the sagittal plane (Figure 3a). The virtual intersection between the midpoint of the trachea and the first rib in the sagittal plane was denoted as 1R (Figure 3b).
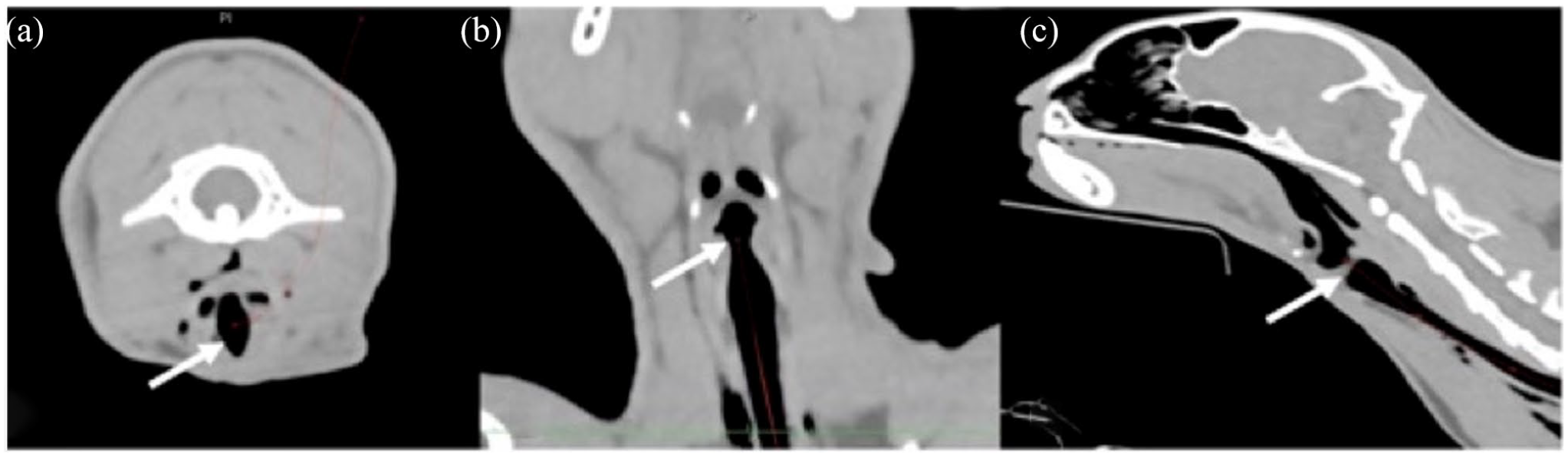
Multiplanar reconstructed CT image of the upper airway from a cat in (a) transverse, (b) dorsal and (c) sagittal views. White arrows show the position of the larynx

CT image of the lower airway from a cat in (a) transverse and (b) coronal views. White arrows show the position of the most cranial aspect of the carina. White dotted line shows the trace of the trachea from larynx to carina

CT image in a sagittal view showing (a) the intersection between the carina (black arrow head) and the fifth intercostal space (black arrow) and (b) the intersection between the trachea (black and white dotted line) and the first rib (white arrow)
Distances were measured using a curved multiplanar soft tissue reconstruction viewed in a lung window (WW1400, WL-500), using commercial viewing software (OsiriX, v.6.5.2. 64bit; Pixmeo SARL). The L–C distance was measured from the larynx to the carina by manually selecting the midpoint of the tracheal lumen at variable intervals of less than 20 mm from cranial to caudal. This produced a curved plane through the trachea, the length of which was provided by the software. The L–1R distance was measured using the same curved plane from the larynx to the virtual intersection of the trachea and the first rib, as determined by the transverse, dorsal and sagittal planes. The 1R–C distance resulted from the subtraction of L–C to L–1R. Where present, the tip of the indwelling ETT was identified and distances measured from the larynx to the ETT tip and from the ETT tip to the carina. All images were evaluated by a board-certified specialist in diagnostic imaging.
Data were analysed using SPSS Statistics for Windows 21.0 (IBM). Normality was assessed using the Shapiro–Wilk test. Descriptive statistics were used. Parametric data were reported as mean ± SD. Non-parametric data were reported as median (range).
Results
A total of 45 cats met the study criteria in the 7-year study period.
All the studied variables, including L–C, L–1R and 1R–C distance, the position of the carina in respect to the intercostal spaces, breed, age, sex and BW are shown in Table 1. Within the total population, 37.8% and 62.2% were females and males, respectively. Mean age was 10 ± 4.2 years and mean BW was 4.5 ± 1.1 kg. A total of nine different breeds were enrolled in the study. The most commonly represented breed was domestic shorthair (n = 32), followed by the domestic longhair (n = 5), Maine Coon (n = 2), Persian (n = 1), British Blue (n = 1), Ragdoll (n = 1), Burmese (n = 1), British Shorthair (n = 1) and Oriental (n = 1).
Summary of the studied variables among the total study population

L–C = larynx to carina; L–1R = larynx to first rib; 1R–C = first rib to carina; DSH = domestic shorthair; DLH = domestic longhair
The L–C distance was 14.3 ± 1.1 cm. This distance was longer in males than in female cats, with a L–C distance of 14.7 ± 1.1 cm and 13.5 ± 0.7 cm, respectively. Among the different breeds, the Maine Coon showed a longer L–C distance (mean length 16.8 ± 0.9 cm), followed by the British Shorthair and the Persian (14.8 cm), Oriental (14.7 cm), domestic longhair (14.4 ± 0.7 cm), British Blue (14.1 cm) and domestic shorthair (14.1 ± 0.7 cm), Burmese (13.2 cm) and Ragdoll (12.9 cm).
The L–1R distance was fairly similar among the different cat breeds, with an average distance of 8.8 ± 0.7 cm. In addition, the carina was caudal to the 1R in 100% of the animals; the mean 1R–C distance was 5.4 ± 0.7 cm. For these reasons, the 1R was considered a reasonable anatomical reference that could guide the process of ETI.
In the present study, 60% of the cats were intubated. From this subpopulation, the tip of the ETT was identified 7.8 ± 1.9 cm caudal to the larynx and therefore 6.4 ± 2.4 cm cranial to the carina. The position of the ETT tip was less than 4 cm cranial to the carina in 18.5% of these patients. If the tip of the ETT had been guided to the position of the 1R in relation to the trachea or, the ETT had been advanced 9 cm from the larynx, none of the tubes would have been less than 4 cm to the carina.
The carina was level with the fourth, fifth and seventh intercostal space in 4.4% (n = 2), 93.3% (n = 42) and 2.2% (n = 1) of the cats, respectively. No EBI was present.
Discussion
One of the biggest concerns during intubation is the misplacement of the ETT, in particular EBI. This is associated with major complications such as hypoventilation and atelectasis of the non-intubated lung and hyperinflation and barotrauma of the intubated lung in the case of inadvertent single lung intubation. Each of these can lead to hypoxaemia, which may result in significant morbidity and mortality.1–4,14 While adequate monitoring of the capnography trace, spirometry, pulse oximetry and simultaneous movement of the thorax and reservoir bag may be useful to recognise some of these complications, 15 ETT misplacement can only be confirmed by visualisation of the ETT within the trachea. ETT misplacement has been recognised as an incidental finding in human and veterinary patients undergoing diagnostic imaging techniques (bronchoscopy, radiography, CT).12,16–18 Despite their ability to recognise ETT misplacement, none of these imaging techniques is routinely used for this purpose, as they would result in additional costs, are time consuming and involve radiation exposure in some cases. Auscultation remains one of the most common used method for detecting inadvertent EBI. However, this technique showed a poor sensitivity, especially among inexperienced anaesthetists. For this reason, it is recommended to combine this technique with other methods, including direct observation of the ETT depth and checking the presence of bilateral chest movements. 19
Selecting the appropriate ETT is fundamental to avoiding complications during intubation. Currently, there are only few studies in veterinary medicine describing methods to estimate the size of the ETT in dogs. In one of these studies, 9 estimation of the appropriate ETT diameter was based on palpation of the tracheal thickness at the level of the thoracic inlet and width of the nasal septum between nares. The authors concluded that choosing an ETT based on these measures had poor accuracy and was not recommended. In the other study, 10 the authors suggested using an ETT in accordance with the internal diameter of the trachea measured on a lateral thoracic radiograph. An ETT that is 70% of the size of the tracheal internal diameter, at the level of the thoracic inlet, resulted in lower resistance and less tracheal damage during intubation compared with when a larger size was used, whereas difficulty in creating an adequate seal was found with smaller sizes. 10 Premeasuring the ETT alongside the trachea from the incisors to the thoracic inlet is a general recommendation to avoid EBI. However, this method is not based on evidence and the distance from the tip of the ETT to the larynx or the carina remains unknown in both dogs and cats. 15 The British Small Animal Veterinary Association’s Manual of Canine and Feline Anaesthesia and Analgesia provides a table that relates the size of an ETT to the animal’s BW. Careful consideration should be taken when using this table as it is not only based on the clinical expertise of the author, but it also does not consider inter-individual variation in tracheal diameter. 15
The aim of this study was to describe an appropriate ETI method, based on the L–C distance, in order to prevent EBI and other complications in cats. The reason for choosing the larynx as the reference starting point instead of the lower incisors is the remarkable differences in skull length between brachycephalic, mesaticephalic and dolichocephalic cats, 20 which could lead to higher variation among the different breeds. In fact, this has frequently been encountered in human medicine, where the appropriate ETT insertion length has been widely studied. Dronen et al 21 first reported that the ETT insertion should not exceed the distance from the lower incisors to the midpoint between the thyroid cartilage and the angle of Louis, a prominent anatomical landmark at the level of the manubriosternal junction in humans. By using this technique, the 21 cm ETT mark appeared to be an appropriate average length of insertion in the studied population. Despite this approach being one the most recommended by anaesthesia textbooks 22 and other researchers,23,24 other authors report an ETT malposition incidence as high as 33.4% when other ethnic groups were studied, suggesting inter-racial variabilities with regard to the mouth to carina distance.25,26 Consequently, additional studies comprising other racial populations have been carried out. These emphasised the use of predicted equations based on age, height, BW, arm span and vertebral column length that best correlated with the lip to carina distance.25,26The L–C distance in cats showed a normal distribution, with a mean of 14.3 ± 1.1 cm. Among the studied population, male cats had a longer distance (14.7 ± 1.1 cm) than females (13.5 ± 0.7 cm). However, as all Maine Coon cats included in the study were male, it is possible that the longer L–C distance in this breed could have biased these results. Therefore, further studies evaluating the influence of sex on L–C distance are required. The difference between the sexes is consistent with human medicine findings, where they describe a longer mouth-to-carina distance in men than women, with a mean of 23.5 and 22.4 cm, respectively.19,26 Some prospective, in situ studies in human medicine consider the lip to carina a good predictor to avoid EBI, showing minimum incidence. In our case, the retrospective nature of this study hindered confirming this theory.Moreover, an important factor to consider is the movement of the ETT during patient manipulation. A retrospective study evaluating the incidence of ETT displacement in dogs undergoing cervical radiography showed an ETT cranial migration of 0.6 vertebrae during neck hyperextension and a mean caudal migration of 3.3 vertebral bodies with flexion from a neutral position. 27 Similarly, Conrady et al 28 reported a significant ETT movement during neck flexion and extension in humans. Flexing the neck showed an ETT caudal movement of 3.1 cm, whereas extension migrated it a total of 5.2 cm towards the larynx. The mean ETT displacement during neck movement was 3.8 cm. For this reason, guiding the ETT tip as far as the mean L–C distance would increase the risk of single lung intubation. Therefore, the latest guidance in humans is to leave a safety margin of 4 cm from both the carina and the larynx to avoid both EBI and laryngeal impingement, respectively.13,28
Following this recommendation, the use of the 1R as an anatomical reference for the ETT insertion would result in a safe margin of 4 cm from both the carina and the larynx of the cats in the present study. In clinical cases, the presence of the thoracic limb may make the identification of the 1R difficult, and caudal flexion of the limb may be needed to identify it. As an alternative, ETT could be introduced through the larynx until the ETT length marking matches the described L–1R distance. This is also recommended when ETT misplacement is suspected during patient manipulation. Sitzwohl et al 19 explain that ruling out EBI by estimating the position of the tube by the insertion depth showed higher sensitivity than bilateral chest auscultation or the presence of bilateral chest movements. The position of the carina was identified in the fifth intercostal space in >93% of the cats. The identification of the fifth intercostal space may be identified as maximum insertion length and could be another reference to guide ETI.
To date, the incidence of EBI, a feared complication during anaesthesia, remains uncertain in cats. In the present study, none of the CT images showed this complication. This study was undertaken in a teaching institution, and despite having a great number of ETIs performed by final-year veterinary students, highly trained personnel and board-certified anaesthetists supervise each step of the procedure. It is possible that in the presence of oesophageal intubation, EBI or other complications, these could have been troubleshooted by the supervisory anaesthetist before the CT scan was performed. As the clinical notes and general anaesthetic records were not reviewed in this study, the absence of oesophageal intubation, EBI or other complications may not reflect the reality in general practice.
The mean ETT introduction distance, which was 7.8 ± 1.9 cm, was similar to our recommendations (L–1R). This could be related to the proximity of the 1R to the thoracic inlet, a common reference used in our institution for ETI.
There are several limitations to this study. The first limitation is the sample size. Even though the study retrospectively evaluated a period of 7 years, the total number of cases included 45 cats. This was markedly influenced by the failure to identify key markers such as the larynx, carina or first rib in the presence of disruptive anatomy, leading to case exclusion. In addition, the majority of CT scans were performed in dogs or exotic species. Secondly, it is possible that the results of the present study may vary among different breeds and therefore further prospective studies evaluating each breed individually are deemed necessary. Owing to the low sample size of certain breeds, it was not possible to evaluate the influence of interbreed variability. In addition, only adult cats were enrolled in the study. As a result, these findings should be carefully extrapolated to juvenile cats. Lastly, we extrapolated the human recommendations of leaving a safety distance of 4 cm from the ETT tip to both larynx and carina. However, there is a lack of evidence in cats in regard to ETT displacement during head and neck movement. For this reason, the authors’ recommendation is to minimise head and neck movement to avoid ETT displacement and other complications during general anaesthesia.
Conclusions
The L–C distance (14.3 ± 1.1 cm) described in this study may guide the maximal insertion length of the ETT in adult cats. This maximal insertion length may also be guided by estimating the position of the carina parallel to the fifth intercostal space. To ensure an optimal ETT insertion length, and following human recommendations where a safe distance of 4 cm from the tip of the ETT to both larynx and carina is advised, the 1R may be used as anatomical reference in adult cats.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee, while not specifically required for publication in JFMS, was nonetheless obtained, as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.