
Abstract
Objectives
The aim of this study was to compare the outcomes of cats undergoing open cystotomy with those undergoing minimally invasive surgery (MIS) for removal of cystic calculi by use of a composite outcome score.
Methods
Twenty-eight cats were retrospectively enrolled and divided into two groups: open cystotomy (n = 14) and MIS (n = 14). The primary outcome measure was a composite outcome score, including three variables: pain scores ⩾2 at either 6 or 12 h postoperatively; failure to remove all stones as determined by postoperative radiographs; and postoperative complications requiring a visit to the hospital separate from the planned suture removal appointment. Other data collected included signalment, history, other procedures performed during anesthesia, willingness to eat the day after surgery and the financial cost of the procedures.
Results
There was no significant difference in age, weight, sex or breed between the two groups. The risk of experiencing the composite outcome was 3/14 (21.4%) in the MIS group and 10/14 (71%) in the open procedure group (P = 0.02). The cats in the open surgery group had 8.3 times greater odds of developing the composite outcome than cats in the MIS group (odds ratio 8.3, 95% confidence interval 1.3–74.4; P = 0.02). In the MIS group, 10/14 cats were eating the day after surgery vs 3/14 in the open procedure group (P = 0.02). The procedural cost was higher in the MIS group, with a median cost of US$945 (interquartile range [IQR] US$872–1021) vs US$623 (IQR US$595–679) in the open group (P <0.01).
Conclusions and relevance
In this study the composite outcome score provided evidence to support the use of MIS techniques in cats with cystic calculi. The composite outcome score should be considered in future veterinary studies as a promising method of assessing clinically relevant outcomes.
Introduction
Urolithiasis is common in veterinary medicine with a high recurrence rate and a large impact on the quality of life of affected patients. Clinical presentation may range from incidentally diagnosed uroliths in asymptomatic patients to cases that present for life-threatening urinary obstruction. 1 An increased incidence of patients presenting with calcium oxalate stones has led to a corresponding increased need for surgical options. Minimally invasive interventional procedures are recommended for patients that present with obstructive urolithiasis, stones that cannot be medically dissolved (calcium oxalate) or clinical scenarios in which urocystoliths are causing patient morbidity. 1
Minimally invasive techniques for the surgical removal of cystic calculi in dogs and cats have been well described.2–7 The advantages of minimally invasive surgery (MIS) include reduced postoperative pain, reduced infection rate and earlier return to normal activity. However, disadvantages exist, such as longer surgical times, the need for specialized equipment, the expense and the requirement for specialized training.8–11 Both dogs and cats may benefit from minimally invasive procedures; however, reports of outcomes solely in feline patients are under-represented in the literature.12–16 While laparoscopic-assisted cystotomy (LAC) and percutaneous cystolithotomy (PCCL) techniques have been described in cats for treatment of cystic calculi in several studies,4–6 they made up <30% of the study populations.
Feline patients are not presented to specialty clinics for treatment of cystic calculi with the same frequency as dogs, presenting a challenge for the recruitment of adequately powered study populations. Recently, assessment of a net (summary) clinical benefit, sometimes known as a composite outcome, rather than multiple specific single endpoints, has been encouraged in studies enrolling human patients.17–19 Composite outcomes typically comprise a combination of efficacy and safety outcomes in order to better assess overall clinical benefit. Because the net outcome occurs at a higher incidence rate than for a single endpoint, they also have the advantage of achieving statistical power at lower case numbers.
The objective of this study was to compare the outcomes of a group of cats undergoing an open cystotomy (OC) with those of a group of cats undergoing MIS for the removal of cystic calculi. The primary outcomes under consideration were formatted into a composite outcome consisting of postoperative pain severity, incidence of residual stones at the end of surgery and incidence of early postoperative complications following discharge. We hypothesized that cats undergoing MIS cystotomy would have a lower composite outcome score than cats undergoing an open procedure.
Materials and methods
Case selection
Cats presenting to a large specialty practice for the surgical removal of cystic calculi from January 2012 to December 2019 were included in this retrospective cohort study if they underwent OC or cystotomy by minimally invasive techniques by one of the two authors (NJB or JB). Only cases performed by one of two board-certified doctors (NJB or JB) were included, to minimize differences in surgical technique and postoperative management. Cases were identified by an electronic medical record search. Cases were included in the MIS group if they were scheduled to receive an LAC or a PCCL. The procedure performed was selected by the owner after being provided with information on both procedure types by the veterinarian. The number or size of uroliths did not affect recommendations for open vs MIS techniques. Cases with incomplete medical records or cases without in-person owner follow-up at suture removal were excluded.
Composite outcome score
The primary outcome measure was a composite outcome score created to include three variables, which were considered by the authors to be of similar significance to patient outcome. A cat was recorded as positive for the composite outcome if any of the following criteria were met: pain scores ⩾2 at either 6 or 12 h postoperatively; failure to remove all stones, as determined by postoperative radiographs; and postoperative complications requiring a visit to the hospital separate from the planned suture removal appointment. The Colorado State University Feline Acute Pain Scale (http://csu-cvmbs.colostate.edu/Documents/anesthesia-pain-management-pain-score-feline.pdf) was utilized for this study (score of 0–4), with scores applied contemporaneously by technicians trained in this scoring system. 20 All cats received postoperative radiographs while still under anesthesia following surgery. All incisions were covered postoperatively with adhesive dressings (Primapore; Smith & Nephew) for the duration of hospitalization. Postoperative complications were summarized from review of the medical record and discussions with owners, and classified as major or minor according to the definitions and criteria proposed by Cook et al. 21
Medical records review
Additional data collected included signalment, history (urethral obstruction or not), stone type, bladder wall culture results, incision length, other procedures performed during anesthesia and procedure performed (classified as LAC, PCCL or OC). Data were also collected on the patient’s willingness to eat the day after surgery and financial cost. Procedural cost was calculated by adding the surgical procedure fee and all materials fees associated with the procedure. Anesthesia charges were consistent across procedures and were not included.
Surgical techniques
Prophylactic antibiotics (cefazolin 22 mg/kg IV) were administered to every patient at induction and every 90 mins thereafter. Clipping and standard aseptic preparation of the ventral abdomen, including the vulva/prepuce, were performed for every patient.
LAC
All procedures were performed by one of the authors (NJB), as previously described by Pinel et al, 4 with the following adjustments. The urinary bladder was partially exteriorized and a stay suture of 3-0 polydiaxonone was placed to retract the urinary bladder. The bladder was not sutured to the body wall. A stab incision was made into the ventral mid-body of the urinary bladder through which the 30° 2.7 mm diameter 18 cm length cystoscope within its sheath was positioned within the urinary bladder. Saline was infused through the cystoscopic sheath, as well as a preoperatively placed urinary catheter when possible (male cats).
Uroliths were removed with suction placed alongside the cystoscopic sheath. For uroliths too large to be removed in this manner, grasping forceps were introduced into the urinary bladder along the sheath. Following removal of all visible cystoliths, the urethral catheter, if present, was slowly withdrawn and the proximal urethra was examined with the telescope for remaining uroliths. A biopsy of the urinary bladder wall was performed in every case and submitted for bacterial culture and sensitivity ± histopathology. The cystotomy incision was closed in one layer with a simple interrupted pattern of 3-0 polydioxanone. Leak tests were performed with a 22 G needle and instillation of saline. The urinary bladder was replaced within the abdomen and the abdomen closed routinely.
PCCL
All procedures were performed by one of the authors (JB), as previously described by Cruciani et al. 5 Briefly, a laparoscopic trocar (6 × 10.5 cm Ternamian Endotip; Karl Storz Veterinary Endoscopy) with diaphragm was introduced in a caudodorsal direction through the abdominal and bladder incision. A 30° 2.7 mm diameter 18 cm length rigid cystoscope (Karl Storz Veterinary Endoscopy) was introduced into the trocar and used to examine the bladder and then switched out for a flexible ureteroscope (FLEX-XC flexible ureteroscope; Karl Storz Endoscopy) for evaluation of the proximal urethra. A 2.4 Fr stone basket (NCircle Tipless Nitinol Stone Extractor 1.5 Fr × 115 cm; Cook Medical) was used to grasp and remove stones. For larger stones, the trocar was removed, and the stone was pulled through the bladder incision. In male cats, the ureteroscope was able to be passed through the proximal two-thirds of the urethra. Complete evaluation of the urethra in female cats was achieved with the flexible ureteroscope. The urinary bladder and abdominal wall were closed as previously described.
OC
All procedures were performed by one of the authors (NJB), as described by Lipscomb, 22 with minor adjustments. A ventral incision was performed, and a bladder spoon was used to remove all visible stones. The bladder was flushed in a normograde and retrograde manner, if possible, with 3.5 F or 5 F red rubber catheters. Sample procurement for culture, bladder closure, leak test and abdominal closure was performed as described for LAC.
Postoperative management
Patients were administered postoperative antibiotics consisting of cefazolin (22 mg/kg IV q8h) for 24 h and were discharged with amoxicillin–clavulanic acid 12.5–20 mg/kg PO q12h for 5–7 days pending culture results. Postoperative pain medication consisted of either continuous rate infusions of fentanyl, bolus intravenous injections of hydromorphone, methadone or buprenorphine, or transmucosal buprenorphine. Non-steroidal anti-inflammatory drugs (meloxicam or robenocoxib) were administered, depending on primary veterinarian preference. All cats were offered food the night of and morning after surgery.
Statistical methods
Power analysis was performed using a Fisher’s exact test. For the study to have 80% power to show a 50% reduction in the incidence of the composite outcome (from 8/14 [57%] cats in the OC group to 1/14 [7%] cats in the MIS group) at the 5% significance level would require the enrollment of 14 cats in each group.
Continuous descriptive data were represented as mean ± SD, where normally distributed, and as median (interquartile range [IQR]) where not normal. Normality was assessed using the Shapiro–Wilk test. Differences in categorical data were tested using Fisher’s exact test, where cell numbers were ⩽5. Group differences between means were tested using the Student’s t-test, and between medians using the Mann–Whitney U-test. Exact logistic regression was used to estimate odds ratios (ORs) and the association between surgical group assignment and outcome after controlling for the effect of concurrent procedures performed. Statistical significance was set at P <0.05. All statistical testing was performed using Stata 16 (StataCorp).
Results
Twenty-eight cats that met the inclusion criteria for this study were identified. No cats were subsequently excluded owing to incomplete medical records or lack of in-person follow-up at suture removal. Fourteen cats were included in the MIS group, of which 11 underwent LAC and three underwent PCCL. Fourteen cats were included in the OC group. No cats were excluded from either group owing to incomplete owner follow-up. All stones were within the urinary bladder prior to surgery. One patient in each group did have stones located within the urethra at the time of or during the surgical procedure. None of the MIS cats required conversion to an open approach.
Study population
Cats were, on average, 6.6 ± 3.2 years and weighed 6.34 ± 1.59 kg, with a greater proportion of neutered males (n = 21/28). Twenty-four (86%) cats were domestic shorthairs, two (7%) were domestic longhairs, and there was one each of Maine Coon and Himalayan.
There was no statistically significant difference in age (P = 0.95), weight (P = 0.28), sex (P = 0.99) or breed (P = 0.23) between the two groups. In the MIS group, 2/14 cats presented with urethral obstruction vs 7/14 in the OC group; however, this difference did not reach statistical significance (P = 0.10). Six of the 14 OC cats had additional surgical procedures performed during anesthesia, including perineal urethrostomy (n = 2), excision of urachal diverticuli (n = 2) and bladder polyps (n = 1) identified intraoperatively, and a small tongue laceration repair (n = 1) vs one cat in the MIS group, which had a laparoscopic liver biopsy (P = 0.08). When the definition of concurrent procedures was restricted to procedures not involving the urinary bladder, these proportions changed to 3/14 vs 1/14 in the OC and MIS groups, respectively (P = 0.60). Incision lengths for the OC group were a mean of 8.4 ± 1.3 cm long vs 3.1 ± 0.6 cm in the MIS group.
Diagnostic results
Cystic calculi analysis was performed for all patients. The following stone types were obtained from these procedures: 18 struvite (nine cases each in the OC and MIS groups), eight calcium oxalate (three cases in the OC group and five cases in the MIS group) and one 50% urate/50% calcium oxalate stone in the OC group. One patient in the OC group had a calcium oxalate exterior shell surrounding a remnant of a ureteral stent from a previous surgery. Eleven patients in the open group and all 14 in the MIS group had no growth on their bladder mucosa biopsy. The three cats in the open group that did have positive cultures grew Pseudomonas aeruginosa (n = 1), Salmonella species (n = 1) and coagulase-negative Staphylococcus species (n = 1).
The risk of experiencing the composite outcome was 3/14 (21.4%) in the MIS group vs 10/14 (71%) in the open procedure group (P = 0.02) (Table 1). Enrollment in the open surgery group was associated with 8.3 times greater odds of developing the composite outcome vs the cats in the MIS group (OR 8.3, 95% confidence interval 1.3–74.4; P = 0.02).
Composite outcome score
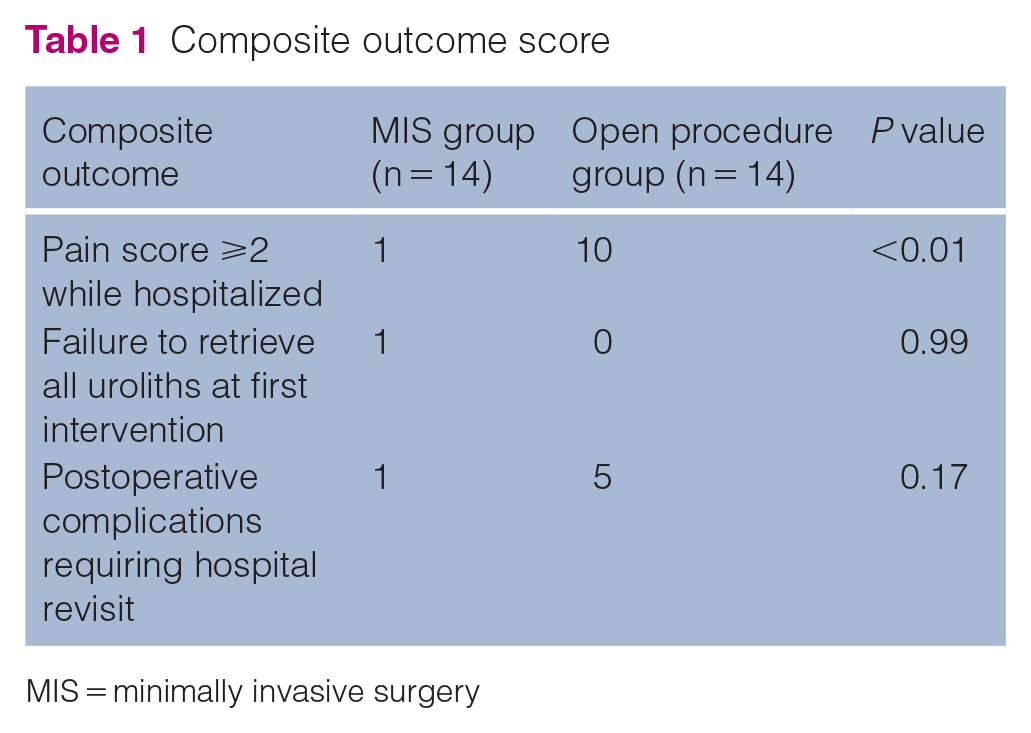
MIS = minimally invasive surgery
The greatest between-group outcome associations were seen in postoperative pain scores, with some disparity also noted in the requirement for additional visits for postoperative complications. Monitored complications included dysuria, stranguria, pollakiuria, gastrointestinal signs and incisional complications. Six of 28 cats required a hospital revisit for management of complications; these consisted of inappropriate urination around the home (n = 1), continued stranguria and pollakiuria (n = 4) and diarrhea (n = 1). The only cat in the MIS group that needed to return for a recheck before suture removal was seen for large bowel diarrhea.
In the MIS procedure group, 10/14 cats were eating the day after surgery vs 3/14 in the OC procedure group (P = 0.02). The procedural cost was higher in the MIS group, with a median of US$945 (IQR US$872–1021) vs US$623 (IQR US$595–679) in the open group (P <0.01).
Discussion
This study suggests that the benefits associated with MIS documented in other clinical populations can also be identified in cats. This study also introduces a composite outcome score to define clinical outcomes, and identified a significant association between procedure type and composite outcome risk. In human studies, this type of analysis17–19 has the advantage of combining multiple parameters to create a global outcome score for a specific procedure. Inherent advantages to this lie in the ability of clinicians to combine variables of similar clinical significance to create an overall score, decreasing the number of patients necessary to reach statistical power. The following variables were used as they were considered of equal clinical importance as they signified serious discomfort to patients: pain score ⩾2 at two postoperative time points; presence of postoperative cystoliths; and postoperative complications requiring a secondary visit. All of these variables required further intervention: additional pain medication; return to the operating suite; or return to the hospital for evaluation and medication. In this study, enrollment in the open surgery group was associated with eight times the risk of experiencing the composite outcome (10/14 vs 3/14; P = 0.02) than cats in the MIS group.
Examining the individual components of the composite score reveals the following differences within the pain score variable. Ten of 14 cats in the open group had pain scores ⩾2 during the first 12 h vs 1/14 cat in the MIS group. More cats presenting with urethral obstruction were seen within the open group (n = 7/14) compared with the MIS group (n = 2/14), although this difference did not reach statistical significance. All obstructed patients were managed with indwelling urethral catheters and pain medication prior to cystotomy. Decreased pain for MIS procedures has been shown in multiple laparoscopic studies in cats and is theorized to be due to decreased tissue manipulation and trauma.9,10,12,15 There was a difference in incision size of approximately 5 cm between groups, which may be one explanation for the difference in pain scores. Our findings are comparable to another study in dogs looking at minimally invasive cystolith removal and evaluating pain during hospitalization. 3 That study reported reduced intravenous pain medication administration to the MIS group vs the open group. Decreasing pain is significant for surgical implications and secondary effects: reduced need for pain medication; decreased systemic effects; earlier hospital discharge; and reduced cost.3,23,24
Pain scoring in cats is more difficult than in dogs.20,25–28 Guidelines by the American Animal Hospital Association/American Association of Feline Practitioners strongly encourage the use of pain scores to assess and treat feline patients without identifying a gold standard system. 25 We used the Colorado State Acute Pain Score for cats as it was the scoring system routinely used during this timeframe, 25 and it has been reported to have moderate-to-good inter-rater reliability.
The second variable considered in the composite score was failure to remove all uroliths. The one case in which this occurred was in the MIS group. Enhanced visualization is considered one advantage of minimally invasive procedures. The added magnification is valuable; however, telescopes cannot be passed through the entire feline urethra owing to the narrow lumen diameter. This inherent anatomic challenge emphasizes the necessity for postoperative imaging. Previous reports document incomplete removal of uroliths in up to 20% patients,2–7 but since postoperative radiographs are not always performed, the true incidence is unknown. Imaging modalities such as abdominal ultrasound or contrast cystourethrography could also be considered postoperatively to ensure complete urolith removal. In our study there was no difference between groups, which mirrors other comparative studies.4,5 The patient in our study was taken back to surgery, the previous incisions utilized and the cystoscope used to locate the stone. It is possible the stone was trapped between the telescope and the bladder mucosa and therefore was not seen during the procedure. None of the MIS cases required conversion to OC. Long-term recurrence or pseudo-recurrence (calculi left behind previously) of cystic calculi was not included in this study, but has been reported in approximately 13–21% of patients.4–6
The last variable considered was postoperative complications. Five of six cats with reported postoperative complications were from the open group, but this difference did not reach statistical significance. We defined a complication as any clinical sign leading to an unscheduled visit to the hospital or reoperation. Our overall postoperative complication rate of 21% (n = 6/28) is consistent with previous reports (25–35%),4,5 but ours is the only study to compare these postoperative complications between surgical types. Postoperative complications in this study most frequently related to signs of dysuria and consisted of inappropriate urination around the home (n = 1), continued stranguria and pollakiuria (n = 4) and diarrhea (n = 1). The only cat in the MIS group that returned for an unplanned recheck examination was seen for diarrhea. Reported complications were seen as early as 4 days postoperatively and the latest up to 14 days. All patients with dysuria required management with anti-inflammatory medication or reinstitution of pain medication. These visits increased cost and stress for pets and owners. Postoperative complications also affected owners perceived comfort of their pet. Patients with cystolithiasis have bladder inflammation that can continue postoperatively. Only 3/28 cats in this study had active infection according to their surgical cultures, and all were within the OC group. None of these patients were in the group of patients exhibiting postoperative complications. It is difficult to quantify how postoperative clinical signs of dysuria are related to preoperative bladder disease as opposed to procedure type; however, the two intervention groups were similar at baseline, while the point differences in incidence of abnormal postoperative urinary behavior were notable.
This study reports reduced postoperative appetite in the open vs the MIS group. This may be due to decreased pain and pain medication requirement. Opioid administration is known to lead to nausea and dysphoria, 23 and appetite is commonly used as a clinical indication for hospital discharge. While cats may refuse food when hospitalized due to stress or anxiety, lack of appetite is a frequent concern for owners and may place cats in a negative metabolic state.
A consensus statement by the American College of Veterinary Internal Medicine recommended minimally invasive urolith removal whenever possible; however, case enrollment was difficult in this study owing to the high number of general practices in the area offering traditional cystotomy. 1 MIS (LAC, PCCL) were grouped together owing to their procedural similarity. Preoperative stone burden and stone size were not specifically examined in this study, but should be included in future randomized clinical trials. These variables have not been previously analyzed in relation to outcome in minimally invasive cystotomies, but have been collected in one descriptive study on PCCL.3–6
More concurrent surgical procedures were performed within the open group (n = 6/14) than in the MIS group (n = 1/14), although this difference did not reach statistical significance. Three procedures were 1 cm urinary bladder biopsies: two at the apex of the bladder for urachal diverticuli excisions and one for a mucosal polyp. We cannot rule out the possibility that the increased incidence of concurrent procedures in the open group contributed to the higher levels of postoperative pain and increased need for revisits due to the abnormal urinary behavior seen in this group. Having said that, only 1/6 OC cats that had other procedures performed was within the group of OC cats having postoperative complications and only 3/6 of this group had postoperative pain scores ⩾2. Other clinical studies on cystolith removal have included patients undergoing a variety of procedures.3,4
This study also reports a difference in procedural financial costs between groups, with a median difference of US$322. An increased cost associated with laparoscopic procedures in veterinary medicine has been reported previously.3,5 Usually, increased costs stem from equipment costs or longer anesthesia times. Interestingly, in human medicine laparoscopy often saves patients money owing to their earlier release from hospital and reduced need for intensive care. In our study, all cats were discharged a median of 1 day postoperatively, so this aspect of cost savings was not experienced. While the added costs are relevant, the decreased pain scores and improved patient experience might outweigh the added expense to some owners.
Limitations of this study include the non-randomized nature of case enrollment, with the inherent potential for selection and information bias. The need for concurrent procedures may have influenced owner selection of an open vs an MIS procedure, and also influenced the postoperative course of the patient. The increased financial cost of the MIS procedures may also have influenced owner selection, while their knowledge of the procedure selected may have differentially affected their recall of the postoperative course. Hospital staff were not blinded to the procedures performed, which conceivably may have biased the pain scores given and the analgesics administered. Group sizes were also small owing to the exclusion of surgeries not performed by the authors (NB, JB). While we felt that the consistency afforded to the surgical technique and postoperative management and monitoring were important, this may have resulted in imprecise estimates of the association between procedure type and incidence of the assessed outcome. Despite these limitations this study provides information on outcomes following MIS procedures for removal of cystic calculi in cats and introduces the composite score as a valuable tool to compare outcomes in veterinary medicine.
Conclusions
This study provides evidence to support the use of MIS techniques for cats with cystic calculi, including associations with reduced postoperative pain and improved appetite postoperatively. These benefits require an increased financial investment. Composite outcome scores suggest an overall advantage to feline patients. Larger studies are required to evaluate the prevalence of postoperative complications with these procedures. Composite outcome scores hold promise for improving power while assessing clinically relevant outcomes in future studies.
Footnotes
Accepted: 13 November 2021
Author note
These data were presented, in part, at The Veterinary Endoscopy Society 11th Annual Meeting (‘Comparison of surgical times, post-operative pain, and complications after a hybrid laparoscopic-assisted cystoscopy vs traditional cystotomy for removal of urinary calculi in cats’), May 2014, and at the Society of Veterinary Soft Tissue Surgery 16th Annual Meeting (‘Updated comparison of the utility of laparoscopic-assisted cystotomy in cats’), June 2017.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.