
Abstract
Practical relevance:
Traumatic injury of the urinary tract may be caused by external accidental trauma or due to iatrogenic injury (typically as a result of catheterisation procedures). Thorough patient assessment and careful attention to patient stabilisation are essential, with diagnosis and surgical repair delayed until the patient is stable, if necessary. Treatment depends on the location and severity of the trauma. If diagnosed and treated promptly, the chance of survival of a patient without other concurrent injuries is good.
Clinical challenges:
Following accidental trauma, at the initial presentation urinary tract injury can be overshadowed by other injuries, but if left undiagnosed or untreated it can lead to serious morbidity and potentially mortality. Many of the surgical techniques described for management of urinary tract trauma can be associated with complications, and so comprehensive communication with the owners is necessary.
Patient group:
The main population affected by urinary tract trauma is young, adult male cats, owing to their roaming behaviour, as well as their anatomy and the resulting increased risk of urethral obstruction and its associated management.
Aims:
This article aims to serve as a guide to all veterinarians who treat cats for the diagnosis and management of urinary tract trauma in cats.
Evidence base:
This review summarises the current knowledge available from a number of original articles and textbook chapters in the literature that cover all aspects of feline urinary tract trauma, and is supported by the authors’ own clinical experience.
Keywords
Introduction
Urinary tract trauma may be caused by external accidental trauma, typically blunt abdominal trauma (eg, resulting from a road traffic accident), or due to iatrogenic injury (eg, from catheterisation). The main affected population is male cats, due to their anatomy and roaming behaviour. Trauma is the most common cause of mortality in cats in England and is responsible for 12.2% of all deaths, with the percentage much higher (up to 47.3%) in cats younger than 5 years of age. 1 Injury to the urinary tract is easily missed at the presentation of trauma patients, as clinical signs can be vague and are often overshadowed by more apparent injuries or life-threatening conditions, such as hypovolaemic shock or head trauma.2,3 The high incidence of iatrogenic catheter-associated injury in male cats is associated with lower urinary tract obstruction and the abrupt change in angle between the penile and pelvic urethra, which presents a risk of dorsal tearing of the urethra with improper technique.
Initial stabilisation
Diagnosis and treatment of urinary tract injuries cannot take precedence over the treatment of shock, respiratory distress or ongoing haemor rhage. 3 Initial stabilisation of trauma patients should include re-establishing tissue perfusion, which can be achieved by administering isotonic crystalloids and oxygen delivery. When administering fluid therapy, concurrent conditions such as brain injury should be taken into consideration and fluid rates should be adjusted accordingly. Aggressive fluid administration may result in interstitial oedema, dilution of coagulation factors and dislodgement of blood clots; 4 therefore, the current recommendation is administration of crystalloids in increments of a proportion of a total shock volume (5-10 ml/kg over 15-20 mins initially), followed by re-evaluation of the patient’s vital parameters (eg, heart rate, Doppler arterial blood pressure, capillary refill time).
In patients with uroabdomen, potassium is reabsorbed into the systemic circulation, resulting in hyperkalaemia. Hyperkalaemia leads to an increase in cell membrane excitability of cardiac myocytes, which can cause life-threatening cardiac arrhythmias, progressing from bradycardia (Figure 1a) to ventricular fibrillation or asystole. 5 ECG monitoring is therefore recommended throughout stabilisation (Figure 1b). Calcium gluconate is administered as a slow intravenous injection to provide emergency stabilisation of the cardiac myocardium. If serum potassium exceeds 7.5 mmol/l, additional therapeutic intervention (eg, dextrose administration with endogenous or exogenous insulin, depending upon severity), in addition to fluid therapy, may be necessary. 6

(a) ECG monitoring of a feline patient presented with suspected urethral rupture. The ECG documents bradycardia and tented T waves consistent with changes secondary to hyperkalaemia, which was demonstrated on blood work in this patient. (b) ECG is monitored continuously while this cat is stabilised with intravenous fluids, calcium gluconate and warming
During the initial stabilisation, avoiding medications that are not reversible and/or that may have a negative impact on gastrointestinal and renal blood flow is recommended. Reversible pure mu agonists (eg, morphine, fentanyl) are preferable for management of pain, although caution should be taken with unstable patients, as opioids can worsen hypotension and hypoventilation. 7 Patients should be monitored carefully and the dose of analgesia titrated to effect based upon pain scoring.8,9
Diagnosis
Early signs of urinary tract trauma can include anuria, stranguria, haematuria, abdominal pain, the presence of free abdominal fluid or lack of a palpable bladder. It is important to remember, however, that the ability to urinate and the presence of a palpable bladder do not rule out urinary tract trauma. 10 In addition, rupture of the intrapelvic or penile urethra may not result in immediately detectable free peritoneal fluid, as the leaking urine may seep subcutaneously. The resulting subcutaneous swelling and fluid accumulation might not be initially apparent and/or could be considered related to bruising due to external trauma. 11
Serum biochemistry
In cats with urinary tract trauma, an increase in creatinine and blood urea nitrogen on serum biochemistry may be noted, as leakage of the urine can lead to post-renal azotaemia. Hyperkalaemia, however, may not develop for 48 h or more following trauma and should not be relied upon to detect urinary tract rupture.
Ultrasonography and radiography
Initial ultrasonographic assessment (abdominal point-of-care ultrasound) and/or screening abdominal radiography can indicate the presence of fluid in the abdomen, with ultrasound being significantly more sensitive at detecting small fluid volumes.
Biochemical and cytological fluid evaluation
Uroperitoneum can be diagnosed based on biochemical and cytological evaluation of abdominal fluid. A ratio of the creatinine concentration in abdominal fluid to blood greater than or equal to 2:1 is predictive of uroabdomen, with a specificity of 100% and sensitivity of 86%. 5 A potassium ratio greater than or equal to 1.4:1 is also consistent with uroperitoneum, with a specificity and sensitivity 100%. In contrast, the concentration of urea in the abdominal fluid is an unreliable indicator of uroabdomen due to the rapid equilibriation between the adominal fluid and plasma. 12 Cytological examination of the fluid is used to establish the presence of bacteria and rule out or confirm a diagnosis of septic effusion (septic uroperitoneum).


Retrograde urethrocystograms performed in male cats for investigation of (a) feline lower urinary tract disease and (b) a suspected urethral rupture. In (a), the normal shape and course of the male feline urethra can be seen. In (b), the extravasation of contrast agent into the surrounding tissues confirms urethral rupture (note that a fracture of the femur can be seen also)
Positive contrast retrograde urethrocystography
If the patient presents with ascites and fluid analysis confirms urine leakage, performing a positive contrast retrograde urethrocystogram (see box) is indicated. In addition, in any cat that has suffered trauma associated with the hindquarters, in particular pelvic fractures, there should be a high index of suspicion of urinary tract injury until this is ruled out with positive contrast retrograde urethro-cystography.
Intravenous excretory urography
Presence of fluid within the retroperitoneal space can indicate damage to the kidneys or ureters, and an excretory (intravenous) urography (Figure 3) should thus be performed. It is recommended that this procedure is carried out under general anaesthesia, as the contrast given intravenously can lead to vomiting, retching and nausea; 13 it should also not be performed on dehydrated animals, due to the potential risk of renal damage. 4 Non-ionic iodinated contrast is given intravenously as a bolus, with ventrodorsal and lateral radiographs taken immediately after the injection. Radiography is usually repeated 5, 20 and 40 mins later, until a diagnosis is made. 13

Excretory urogram in a male neutered domestic shorthair cat. The cat had presented depressed and recumbent following an unwitnessed trauma. There was evidence of marked abdominal bruising and blood work demonstrating azotaemia. The excretory urogram shows ureteral rupture and leakage of contrast agent into the peritoneal cavity (arrows); it is not contained within the retroperitoneal space. The cat was managed with an emergency unilateral ureteronephrectomy following stabilisation
Further diagnostic imaging
Advanced diagnostic imaging, including fluoroscopy and CT, may also be beneficial in some cases of urinary tract trauma.
Urinary tract trauma conditions
Uroperitoneum
Uroperitoneum usually develops from disruption of the urinary bladder, proximal urethra or distal ureters, and leads to severe electrolyte and metabolic changes. The most common causes of uroperitoneum are blunt abdominal trauma, urethral catheterisation and bladder expression.14-16
Treatment
At presentation, patients with uroperitoneum may not be stable enough to pursue further diagnostic procedures or surgery, and initial stabilisation is key; as such, uroperitoneum is initially a medical, rather than surgical, emergency, and should be treated accordingly. It is important, however, to recognise that medical management of hyperkalaemia will only provide a short period of improved stability and that definitive repair or urinary diversion must then be prioritised.
Alongside adequate patient stabilisation, urinary diversion techniques are required to reduce urine accumulation in the peritoneal cavity. An indwelling catheter should be placed in the urinary bladder to constantly drain urine. If a urinary catheter cannot be placed, for example if complete urethral obstruction is present or urethral rupture has occurred, other urinary diversion techniques must be used.
Cystocentesis may be used for decompression of the urinary bladder, but this is only acceptable if a definitive management plan is executed within the following 12-24 h period. While cystocentesis in the normal bladder rarely cause problems, the puncture sites may not seal if the bladder is distended or diseased. The use of a percutaneous cystotomy pigtail catheters is also suitable for urinary diversion in the cat; however, a 40% complication rate was noted in one study of urine leakage, dislodgement, urinary tract infection and bladder rupture. 17
Placement of a cystostomy tube (see box on pages 10 and 11) is advised for prolonged urinary diversion and, in particular, when there is significant trauma to the lower urinary tract or neurological dysfunction. This requires general anaesthesia and can be performed via a ventral midline approach 18 or a minimally invasive approach. 19 The choice of tube used as the tube cystostomy depends upon the anticipated length of urinary diversion required. If use for up to 3-6 weeks is anticipated then a silicone Foley catheter is suitable; however, if longer term use is required a polyurethane tube with mushroom tip is more durable. For patients with severe azotaemia, peritoneal dialysis, haemodialysis or continuous renal replacement therapy can be used.16,20
Prognosis
Although studies show the mortality rate of cats with uroperitoneum can be 25-38.5%, with one finding that an elevation in blood creatinine at presentation is significantly associated with a failure to survive to discharge, 15 the prognosis for cats with a treatable underlying cause and no concurrent injuries seems to be good.14,15
Renal trauma
Renal injury is rare due to the relatively protected location and mobility of feline kidneys.
Treatment
The approach to renal injuries depends on the severity of the renal damage. While kidney contusion can be treated conservatively, trauma resulting in rupture or avulsion of the ureter from the renal pelvis requires surgical exploration. Mild renal contusions or fractures heal primarily by synthesis of fibrous connective tissue. Although wound contraction in these cases is usually minimal, it may lead to scar tissue formation. For minor laceration repair, the renal parenchyma is apposed with digital pressure and the capsule is closed with simple continuous absorbable suture. There is a documented use of semi-elastic polyglactin mesh and polyglycolic acid mesh on severely lacerated kidneys to control haemorrhage and preserve renal function. 21
Ureteronephrectomy (see box) is indicated for uncontrollable haemorrhage, persistent urine leakage and in situations where finances or client preference dictates a definitive solution with minimal chance of revision surgery being required. In theory, before the nephrectomy is performed, the glomerular filtration rate should be checked to assess the function of the opposite kidney; however, this is not realistic in practice due to the need for emergency intervention. If bilateral trauma has occurred, or contralateral kidney function is compromised, other surgical methods that preserve both kidneys should be utilised; for example, partial nephrectomy or the use of a subcutaneous ureteric bypass (SUB) system (see box), which has been described for management of bilateral ureteric rupture in a cat. 25


Partial nephrectomy is occasionally warranted, to preserve renal function, if bilateral renal damage is discovered or if severe injury affects only a pole of the kidney. This technique may also be useful if the contralateral kidney is diagnosed with impaired function; one study has shown that cats exhibit comparative stability of renal function for 12 months after moderate to marked reduction of functional renal mass owing to partial nephrectomy. 26 However, total nephrectomy is usually easier to perform and carries less risk of postoperative haemorrhage. Despite the risk of potential excessive blood loss, electrocoagulation of bleeding vessels should be avoided as this causes parenchymal damage.
Prognosis
In a retrospective study on morbidity and long-term outcome of unilateral nephrectomy in feline kidney donors, there were no long-term effects observed in 84% of the patients. Within 10 years of the surgery, 7% of the cats had developed renal insufficiency or died of urinary tract disease. 22 These data allow us to speculate that if the contralateral kidney is proven to be healthy, the long-term prognosis for cats undergoing unilateral nephrectomy is very good. For data regarding SUB device prognosis, see the box.
Ureteral trauma
Owing to the mobility of the feline kidney, blunt trauma is a less common cause of ureteral rupture; in contrast, iatrogenic ureteric injury as a complication of ovariohysterectomy is seen more frequently. 27
Treatment
Owing to the small diameter of the ureter, repair is technically challenging or unfeasible for end-to-end anastomosis and requires magnification and fine instruments/suture. The risk of ureteral stricture and stenosis is significant. 28 The key aim of ureteral trauma treatment is preservation of renal function. Current guidelines for treatment of ureteral injuries advise ureteroneocystostomy, ureteronephrectomy (see box on page 4) or ureteral ligation with SUB device placement (see box), all of which are techniques most suited to a referral setting.
Ureteroneocystostomy, or ureteral reimplantation, is a technique indicated mainly for trauma in the distal part of the ureter. A ventral celiotomy is performed and the ureter is dissected from the retroperitoneum. Stay sutures are used to facilitate delicate tissue handling; it is vital to avoid crush injury with surgical manipulation or trauma to the blood supply. The proximal ureter is transected at a level just proximal to the site of ureteral trauma. The distal end of the remaining ureter is passed through a stab incision in the bladder wall and anastomosed to the bladder mucosa. 2 The redundant distal ureteral segment is ligated proximal to the bladder and resected. If needed, psoas cystopexy and/or renal descensus can be performed. 29 A comparison of techniques has been described for ureteroneocystostomy in cats with undilated ureters and the optimal technique is reported as extravesicular ureteroneocystostomy with a simple interrupted suture pattern. 30 This technique had a lower mortality rate in the experimental study compared with the use of simple continuous sutures and resulted in a lower serum creatinine concentration. 30
Another option when the proximal ureter is short is ureteroneocystostomy performed after elongated cystoplasty through the creation of Boari flap and kidney transposition. 31 A case report of a successful replacement of the ureter in a cat, with the use of an ileal graft, has also been published. 32
Although the SUB (Norfolk Vet Products) system (see box on page 5) was designed for treatment of ureteral obstruction, there are known and published cases of its successful use in ureteral trauma patients.25,33,34
Prognosis
In a retrospective study on management and outcome of iatrogenic ureteric injury following ovariohysterectomy, 14 cats were identified. The cats were managed with ureteronephrectomy as a definitive approach to management (4/14), ureteroneocystostomy (5/14) or use of unilateral or bilateral SUB devices (3/14), and two cats died without further management. 27 Three cats that underwent ureteroneocystotomy subsequently had a ureteronepherectomy, predominantly due to pyelonephritis, but went on to have excellent outcomes. 27
Urinoma
A urinoma, also known as a uriniferous pseudocyst, is an accumulation of extravasated urine within a fibrous sac in the retroperitoneum.35-39 A urinoma occurs when there is a disruption of the urinary collecting system at any level from the renal pelvis to the urethra, which can be due to blunt trauma, ureteral obstruction or iatrogenic causes. It is typically seen associated with the upper urinary tract (ureteral or renal injury). Blunt trauma may lead to rupture of the ureter due to an increase in intraluminal pressure or may secondarily lead to ureteral obstruction by a haematoma, clot or fibrosis. Small tears may heal spontaneously. Larger defects, allowing ongoing slow leakage of urine, may result in urinoma formation; significant trauma with greater urine leakage results in uroabdomen and systemic effects. When a urinoma forms, initially the extravasation of urine results in lipolysis and fat necrosis. This is followed by a fibro-blastic hyperplasia and round cell infiltration, which confines the urine in 5-12 days and encapsulates it within 3-6 weeks.
Diagnosis
Patients with a urinoma usually present several weeks after the initial trauma as the urinoma increases in size due to ongoing urine accumulation.35-39 The clinical signs associated with urinoma are usually non-specific, such as anorexia, depression, lethargy and weight loss, although presence of a mass/ swelling in the dorsal mid-abdomen may help to narrow the differential diagnoses (Figure 4a). Hematobiochemical analysis may detect mild azotaemia and a non-specific inflammatory leukogram.35-39 Hydronephrosis, an anechoic mass in the renal/ureteral region and dilation of the proximal ureter may be noted on ultrasound examination. 38
Imaging plays a key role in diagnosing a urinoma, with excretory contrast studies and CT considered the modalities of choice (Figure 4b-d). Single imaging studies may not be sufficient to detect urinary lesions, potentially leading to an underdiagnosis of the condition. Manzini et al had improved results with achieving a diagnosis by performing a further radio-graphic examination 4 h after the contrast injection and a delayed (70 mins) CT study. 39 Additional time is needed to observe the iodinated urine attenuation, and so combining different imaging modalities and performing delayed imaging studies seem to be the key to detecting urinomas. 39 A definitive diagnosis can be made when the fluid from the pseudocyst is aspirated and the concentration of the creatinine exceeds that of peripheral blood at a ratio of equal to or greater than 2:1. Percutaneous aspiration of the fluid is, however, associated with a risk of further fluid leakage into the retroperitoneal or peritoneal space.
Urinoma must not be confused with other types of perirenal pseudocysts, intracapsular pseudocyst and extracapsular perirenal pseudocyst, which have a non-traumatic aetiology. Intracapsular pseudocyst is the most common of these and is described as an accumulation of transudate between the renal capsule and renal parenchyma; it is usually seen in senior cats with chronic renal failure. 40
Treatment
Traumatic urinomas are successfully treated by establishment of upper urinary tract continuity and drainage of the cavity.35-39 Ureteronephrectomy combined with urinoma capsule tissue excision is the standard treatment, as severe ureteral trauma and fibrous adhesions do not allow neoureterocystostomy (Figure 4e,f). In a single case report, successful use of a SUB device for the treatment of a paraureteral urinoma has been described. 41 If complete resection is not possible, incorporation of the omentum into the urinoma cavity is beneficial, as it reduces the dead space through adhesion formation and physiological drainage. 36
Prognosis
Urinomas carry a favourable prognosis if recognised and treated appropriately.35-39


(a) A male neutered domestic shorthair cat, which was depressed and had a reduced appetite, was referred for assessment of an abdominal mass. The cat had experienced trauma 3 weeks earlier but despite an initial improvement remained unwell. A firm mass on the left side of the abdomen was noted on physical examination; the left kidney could not be palpated. Blood work demonstrated a mild azotaemia. Abdominal ultrasound revealed a fluid-filled mass in the left retroperitoneal space. (b,c) Plain radiographs of the abdomen showed a lack of definition of the renal silhouettes and increased radio-opacity within the retroperitoneum. (d) An intravenous urogram showed normal contrast excretion from the right kidney, but contrast excretion or passage on the left was limited. (e) Exploratory laparotomy revealed a large mass lesion (arrow) of the left retroperitoneal region. (f) Dissection of the lesion revealed a large fibrous capsule surrounding a fluid-filled cavity (urinoma; arrow). A left ureteronephrectomy was performed and the urinoma capsule was lavaged and omentalised
Bladder trauma
In a retrospective study investigating uroperitoneum in 26 cats, the bladder was found to be the most frequent site of urine leakage following blunt abdominal trauma (84.6%). 14 In the authors’ experience, bladder rupture can occur as a result of compression of a full bladder on blunt trauma impact or trauma from pelvic fracture fragments, or can be due to bruising resulting in localised areas of necrosis. The probability of bladder trauma correlates directly with the degree of its distension at the time of the accident. 42 Rupture may also occur as a result of not only trauma, but also severe cystitis, neoplasia, urethral obstruction or iatrogenic causes. 16
Treatment
Surgical management of bladder rupture is similar to the technique described for cystotomy. After isolation, the viability of the bladder tissue is evaluated by assessing colour, wall thickness and blood supply. Any necrotic or highly traumatised areas of the bladder are trimmed with delicate scissors. The most important area of the bladder is the trigone; with an intact trigone, up to 75% of the bladder can be removed and will gradually regain adequate size. 42 Where resection of a significant portion of the bladder is necessary, the authors recommend, based on their clinical experience, closing the bladder over a small Foley catheter bulb to ensure the lumen is maintained during suturing. In most cases, single-layer appositional closure of the bladder is recommended, but other suture patterns, such as inverting double-layer closure, have also been described with no significant difference in short-term complication rate and duration of hospitalisation.42,43 When the viability of the bladder tissue at the suture line is questionable, a serosal patch from the antimesenteric border of the small intestine loop can be used or the area may be omentalised. 44
Prognosis
The prognosis for management of bladder rupture is good provided there are not significant concurrent injuries.
Urethral trauma
Urethral trauma is uncommon in cats and usually associated with urethral catheterisation (Figure 5), 45 bite wounds, pelvic fractures, gunshot injury, blunt abdominal trauma (Figure 6) and calculi, 16 with vehicular trauma and iatrogenic damage owing to attempted catheterisation being the most common causes. 46 The location of the trauma is related to the cause of the rupture. 47 One study of 63 cats with urethral rupture reported that cats suffering from vehicular trauma are more likely to have a pre-pelvic urethral rupture (73.5% of analysed patients) than a post-pelvic rupture (14.7%). 11 Conversely, the same study reported patients with iatrogenic trauma suffered a post-pelvic rupture more frequently (77.8%) than intra-pelvic (18.5%) and pre-pelvic rupture (3.7%). 11 Iatrogenic trauma to the urethra typically occurs at the dorsal aspect of the urethra (where the penile urethra transitions into pelvic urethra), during attempted catheter placement; this can be avoided with appropriate sedation of the cat and caudal retraction of the penis during catheter placement to efface this flexure. Urethral trauma may result in bruising, rupture, avulsion and post-traumatic scarring. With urethral rupture, urine may leak and accumulate in the abdomen, pelvic canal or subcutaneous tissue leading to tissue necrosis, and this will usually become apparent after 24-48 h; the true extent of tissue necrosis, however, may not be noted until around 10 days to 3 weeks after the insult. 48 Complications of urethral trauma include stricture, ongoing urinary leakage and urinary incontinence, and urinary tract infections.11,49


A male neutered domestic shorthair cat was referred following difficulty passing a urethral catheter for management of urethral obstruction. (a) A positive contrast retrograde urethrogram confirmed contrast leakage arising from the junction of the pelvic and perineal urethra (arrow), which is the typical site for injury related to catheterisation. (b) A cystostomy tube was placed to provide urinary diversion and the patient was hospitalised pending definitive management. (c,d) A transpelvic urethrostomy was subsequently performed a week later, once the perineal skin appeared healthy and no sequelae of urine extravasation were apparent. Perineal urethrostomy may often be appropriate with this type of injury; however, in this patient the lesion was slightly more proximal, necessitating a slightly more cranial urethostomy via a transpelvic approach


A female neutered domestic shorthair cat was found collapsed in the garden after being missing for 24 h. Blood work demonstrated azotaemia and hyperkalaemia. (a) A point-of-care abdominal ultrasound revealed an intact urinary bladder. (b) A retrograde vaginourethrocystogram revealed contrast leakage (arrow) consistent with rupture of the proximal urethra. Following ongoing stabilisation, the cat was anaesthetised for exploratory surgery. (c) A proximal urethral rupture, with avulsion of the urethral segments, was confirmed. (d) A red rubber feeding tube (arrows) (3.5 F) was used as a urethral catheter and (e) the urethra was reconstructed over the catheter with preplaced polydioxanone sutures before (f) apposing the segments of urethra and tying the sutures. A cystostomy tube was placed to provide urinary diversion
Treatment
The location of the urethral trauma will affect which surgical options are possible. 47 Urethral trauma can be managed in three ways: (1) temporary urinary diversion and primary repair; (2) temporary urinary diversion and second intention healing; and (3) permanent urinary diversion via urethrostomy.11,49 Literature regarding optimal treatment of urethral rupture in cats is relatively limited. Urethral mucosa will regenerate over a catheter if a viable strip of the tissue bridges the defect. 48 Smaller lacerations will usually heal spontaneously if urine is diverted for approximately 7 days. 49 Larger defects may require the presence of a catheter for up to 4 weeks to completely heal. Addison et al 11 suggest that injuries to the pelvic urethra often require management by urethral anastomosis (Figure 6d-f). To avoid further tissue irritation, urinary diversion is recommended, either via placement of an indwelling urinary catheter or surgical placement of a cystostomy tube. Another advantage of urinary diversion is the reduced potential for urethral stricture, which is associated with urine contact with the healing incision. 49
The advantages of an indwelling urinary catheter include its relative ease of insertion and removal, effective urine diversion, low cost, low morbidity rate associated with dislodgement, and potential to act as a splint and a guide for re-epithelialisation of the urethral mucosa. 49 It is important to note, however, that retrograde placement of a urinary catheter can be challenging following trauma. The use of a hydrophilic guide wire, inserted transabdominally into the urinary bladder and directed out of the urethra in a normograde fashion under fluoroscopic guidance, has been described to achieve urethral catheterisation where retrograde catheterisation is not possible. 50 This technique is particularly useful when iatrogenic urethral injury has been caused during attempted catheter placement, as typically the injury is a small partial tear amenable to management over an indwelling urethral catheter.
Advantages of a cystostomy tube (see box) for urinary diversion include minimal interference with urethral healing, the ability to empty the bladder in patients where placing a urethral catheter failed and improved comfort for the cat. 42
Permanent urinary diversion can be achieved via a urethrostomy (Figure 5c,d). The most common technique in male cats is perineal urethrostomy, although prepubic and transpelvic urethrostomies have also been described in the literature.38,39 Urethrostomy at more cranial sites is documented to have a greater complication rate. 47
Perineal urethrostomy is a procedure performed to create a permanent opening between the pelvic urethra and the skin in the perineal region (Figure 8). This method is typically recommended for cats suffering from penile urethral trauma, most commonly due to iatrogenic catherisation injury. 51 Several techniques have been described, and that by Wilson and Harrison 52 is reported to have the lowest rate of complications, which can include haemorrhage from erectile tissue, wound dehiscence, urine leakage into the perineal tissue, urinary tract infection, stricture, incontinence, perineal hernia and rectourethral fistula.51,53 Traditionally, non-absorbable simple interrupted suture was recommended for apposition of the urethral mucosa and skin; however, use of simple continuous absorbable suture is also described to have the same outcome. 54 In the early postoperative period, stricture formation is the most frequent complication, affecting 2-12% of patients. Although this is a major complication requiring surgical correction, these patients tend to enjoy complication-free long-term outcomes following surgical revision. The most common late complication is bacterial urinary tract infection, which affects 17-57% of cats undergoing perineal urethrostomy. 55 Ruda and Heiene found that clients consider their pet to have a good quality of life after this procedure. 53 A modified perineal urethrostomy technique has been published by Yeh and Chin that uses the preputial mucosa for anastomosis with the pelvic urethra. 56 This technique seems to have reduced risk for narrowing of the stoma and development of stenosis, as well as irritation dermatitis in the perineal region, but is a more technically challenging surgery to perform.56,57

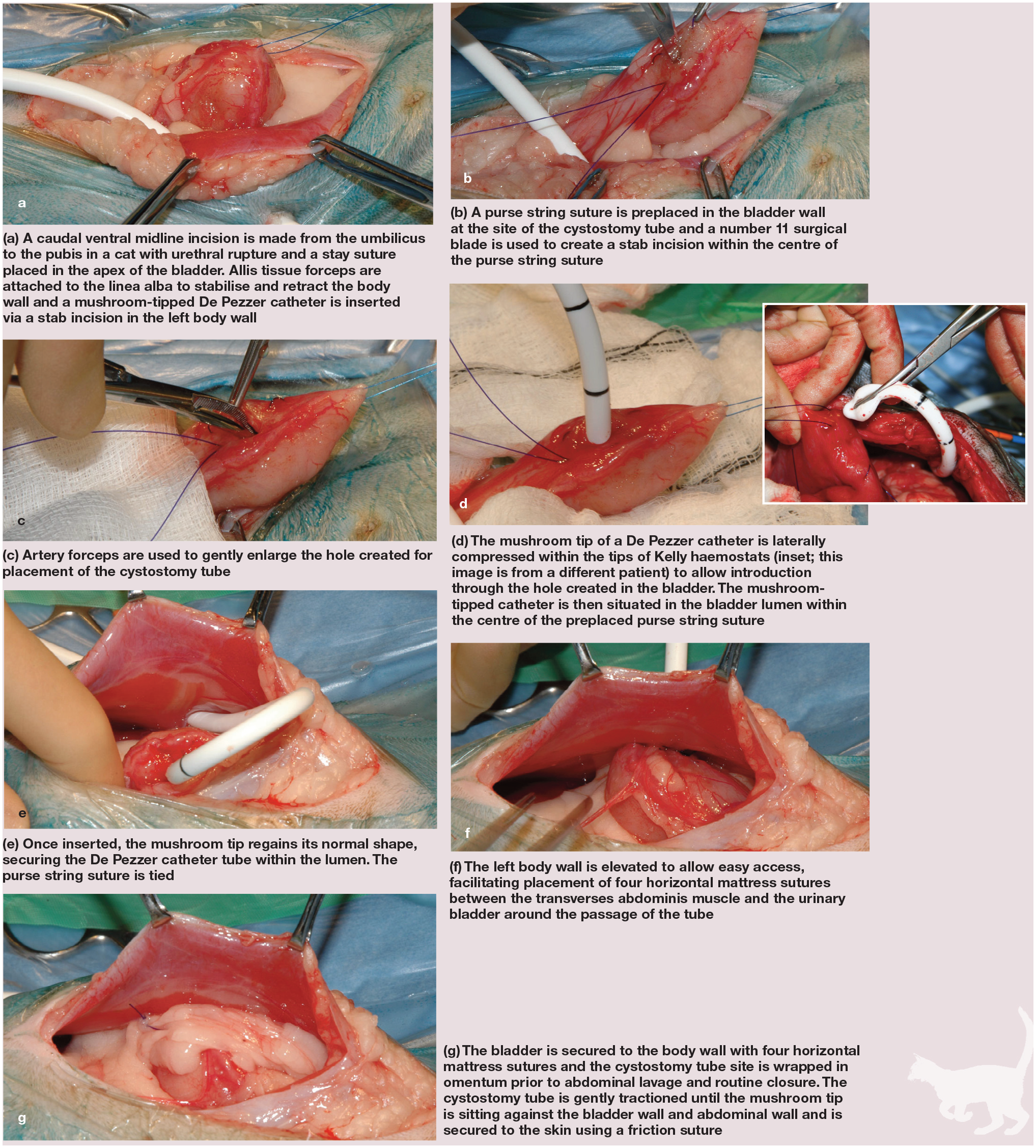
Cystostomy tube placement via a ventral midline approach

Perineal urethrostomy stoma appearance at the end of surgery: (a) including the perineum and (b) close up
Vaginourethroplasty is a procedure described for management of distal urethral rupture in female cats, where an anastomosis is made between the proximal urethra and distal vagina. Owing to the small size of the feline urethra and vagina, use of magnification is advised for this technique. 58
Transpelvic urethrostomy is a technique that can be used as a primary procedure, or as a salvage procedure after failed perineal urethrostomy in cats with urethral trauma. It starts with a celiotomy and cystotomy to insert the urinary catheter into the urethra, to help with later identification. Retrograde catheterisation may not be feasible due to urethral trauma or stricture. The catheter is secured to the bladder with a purse string suture to avoid urine leakage into the abdomen. The scrotum and prepuce are excised using an elliptical incision and the penis is denuded ventrally. Bilateral medial to lateral adductor muscles (gracilis and external obturator) elevation is then performed. Ostectomy of the ischium is carried out, creating an osteotomy area 10 mm wide and 12 mm long. A ventral longitudinal urethral incision is made over the catheter from the bulbourethral glands to a point 2-3 mm cranial from the osteotomy margin. The urethral mucosa is sutured without tension to the skin margin with simple interrupted sutures. The portion of the penis distal to the bulbourethral glands is amputated and the urinary catheter is removed and introduced into the urethrostomy to check its diameter. Cystotomy and celiotomy are routinely closed. The procedure is well tolerated; in a study of 11 cats that underwent transpelvic urethrostomy, four developed complications, but none of them required revision surgery. 59 Complications included stricture formation, haematuria, dysuria and urinary tract infection;47,59 pubis fracture is also a rare complication reported secondarily to transpelvic urethrostomy. 60
Prepubic (antepubic) urethrostomy (Figure 9) is a salvage surgical technique that may be used for management of pelvic urethral trauma in cases where standard techniques for urethrostomy cannot be used. The procedure starts with a ventral midline celiotomy followed by identification and blunt dissection of the urethra from the surrounding peri-urethral fat, taking care not to traumatise the urethral vessels and pelvic nerves. The urethra is then ligated in the most distal portion of the healthy urethra with an absorbable suture. Cranial to the ligature, the urethra is transected and catheterised. On the ventral surface of the proximal urethra a spatulating incision is made. The urethra can be exteriorised through the caudal part of the celiotomy. The linea alba is then sutured around the exteriorised urethra with simple interrupted sutures. To create a urethral stoma, the end of the urethra is sutured to the surrounding skin. In a study conducted by Baines et al, 11/16 cats developed some form of complication. The most common complications were urinary tract infection, peristomal skin irritation and necrosis, and urinary incontinence. 61
For cats that have had prepubic urethrostomy, in one study survival rates were reported to be 94% at 6 months and 80% at 1 year. 61 Quality of life was reported to be good for all urethrostomy techniques in 93% of owners. 47 Short- and long-term complications were more likely in cats that had undergone prepubic urethrostomy (peristomal dermatitis and long-term urinary incontinence). 47
(a) Intraoperative photo of a prepubic urethrostomy being created. The urethra has been channelled via the abdominal wall and will be sutured to create a urethrocutaneous stoma just lateral to the midline. (b) Prepubic urethrostomy stoma following healing
Key Points
Ability to urinate and a palpable bladder do not rule out urinary tract trauma.
Hyperkalaemia can result in life-threatening cardiac arrhythmias, progressing from bradycardia to ventricular fibrillation or asystole.
Initial stabilisation is key and cannot be overlooked. Diagnosis and surgical repair can wait until the patient is stable, if needed.
A ratio of the creatinine concentration in abdominal fluid to blood equal to or greater than 2:1 is predictive of uroabdomen with a specificity of 100% and sensitivity of 86%. A potassium ratio equal to or greater than 1.4:1 is also consistent with uroperitoneum with a specificity and sensitivity of 100%.
Elevation in blood creatinine at presentation is significantly associated with a failure to survive to discharge.
Direct end-to-end ureteral anastomosis is a very challenging technique due to the small diameter of the feline ureter and the proliferative capacity of the ureteral endothelium. Ureteroneocystostomy, SUB device placement or ureteronephrectomy are therefore more appropriate techniques for ureteral rupture management.
As long as the trigone is intact, up to 75% of the bladder can be removed and it will still heal and eventually regain normal size and function.
Urethral trauma can be managed in three ways: (1) temporary urinary diversion and primary repair; (2) temporary urinary diversion and second intention healing; and (3) a permanent urinary diversion via urethrostomy.
Healing of the urethra depends on the contact of the damaged tissue with the urine and continuity of the urethral mucosa. Therefore, no matter which technique of urethral trauma management is chosen, urinary diversion is always beneficial to the patient. Urinary diversion can be achieved by placing an indwelling urinary catheter or a cystotomy tube.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.