
Abstract
Objectives
The aim of this study was to evaluate the effect of two differently sized butterfly catheter needles and the effect of venepuncture difficulty on thromboelastography (TEG) results in healthy cats.
Methods
Twenty-four healthy cats were included. Blood samples were collected from the jugular vein by syringe aspiration via direct venepuncture with 21 G and 22 G butterfly needles. The venepuncture difficulty score was classified into four categories. The first 1.5 ml blood drawn from each subject was discarded before collecting a sample for TEG analysis. TEG analyses were performed on citrated whole blood samples from 17 clinically healthy cats, using assays with kaolin as activators. Among the TEG parameters, reaction time (R), clot formation time (κ), alpha angle (α), maximum amplitude (MA) and global clot strength (G) were recorded from each tracing.
Results
Seven cats were excluded from the study; results were obtained for the remaining 17 cats. There were no statistically significant differences between the use of two different needles for R (P = 0.72), κ (P = 0.74), α (P = 0.99), MA (P = 0.08) and G (P = 0.09). Samples with difficulty scores ⩾1 were not significantly different from samples with difficulty scores of 0 for R (P = 0.24), κ (P = 0.65), α (P = 0.65), MA (P = 0.72) and G (P = 0.77).
Conclusions and relevance
The results of TEG in clinically healthy cats do not differ significantly when using two different gauge needles. There was no significant difference in the TEG results according to venepuncture difficulty scoring.
Introduction
Thromboelastography (TEG) is a point-of-care technique designed to detect the viscoelastic properties of whole-blood clot formation and dissolution.1,2 In veterinary medicine, TEG has been used since the early 1960s, and it has been routinely used in the past decade. 3 TEG can be used to identify and predict coagulation states relating to various types of feline diseases and surgical complications, including hypertrophic cardiomyopathy, liver disease, feline infectious peritonitis, disseminated intravascular coagulation, vitamin K deficiency, inflammatory disease and neoplasia. 4
Minimally invasive venepuncture is the ideal method for collecting blood samples for use in coagulation testing. This method minimises activation of the coagulation cascade and provides the most accurate measurements. 5 However, various factors can affect the coagulation results, leading to shortened activated clotting times, platelet activation or clumping. The factors that affect the coagulation results are defined as pre-analytic factors, and they should be considered in coagulation testing, such as with TEG. 6 The blood collection site, venepuncture technique and needle size are commonly known pre-analytic factors. 6 In canine and human medicine, studies on pre-analytic factors have been widely carried out;6–9 considerably fewer have been carried out in cats.
In veterinary medicine, various activators have been used for TEG analysis. The addition of an activator, such as tissue factor or kaolin, can be employed to decrease analytical variability, when compared with native samples in healthy cats.1,10 One study reported that significant differences were observed between native and kaolin assays for reaction time (R), clot formation time (κ), alpha angle (α), maximum amplitude (MA) and clot lysis. 1 In another study, significant differences were found between native, kaolin-activated and tissue factor-activated samples for all TEG parameters. 10
According to the guidelines on rotational viscoelastic assays in veterinary medicine, needle size is considered one of the pre-analytic factors. Thus, the use of 21 G or larger gauge needles is recommended in small animals. 11 In dogs, a study evaluated whether there was a significant difference in TEG results when using a 20 G vs a 21 G needle for blood collection. No significant differences between the two different sizes of needles were reported. 6 However, the effects of different needle diameters used for sample collection have not been considered in cats. Recent studies have established TEG reference interval values using activators in healthy cats; however, they have used a combination of 21 G or 22 G needles for blood sampling.1,4,12–15 It is known that the venepuncture technique also affects the results of coagulation tests in veterinary medicine.5,6 One author classified the venepuncture difficulty score into four categories in dogs and then reported whether there was a significant difference in TEG parameters between the samples assigned with different difficulty scores. No significant differences were observed with regard to the venepuncture difficulty score. 6
In cats, studies of pre-analytic factors for TEG analysis are necessary because cats require the use of large needles for blood collection and are more difficult to restrain than dogs.
The objective of this study was to determine whether the needle size (21 G vs 22 G) and level of venepuncture difficulty, led to a significant difference in TEG results. We hypothesised that variation in needle size and venepuncture difficulty would have a significant effect on TEG results
Materials and methods
Recruitment and sampling
Twenty-four clinically healthy cats owned by students or staff members at the Department of Veterinary Internal Medicine, College of Veterinary Medicine, Chungnam National University, were recruited for this study. Owners were provided information about the study through a notice, and they agreed to participate. The cats included in the study did not take any medications for more than 6 months, and they had no previous history of coagulation dysfunction. They were determined to be healthy based on a normal physical examination and the results of a complete blood cell count (CBC [Advia 2120 Hematology System; Siemens Medical Solution Diagnostics], serum biochemistry panel (Mindray BS300; Randox Laboratories) and coagulation profile (prothrombin time [PT; Nycocard D-Dimer assay; Nycomed Pharma], activated partial thromboplastin time [aPPT; Nycocard D-Dimer assay], D-dimer [VetScan VSpro and PT/aPTT cartridges; Abaxis] and fibrinogen [Neodin Veterinary Diagnostics]). This study was granted approval from the Institutional Animal Care and Use Committee at Chungnam National University (approval number CNU-01065).
Blood sampling was performed by atraumatic jugular venepuncture using 21 G and 22 G butterfly needles (MDR-04121A; Cosmomedical) without sedation. The first 1.5 ml of blood drawn was discarded before collecting a sample for TEG. Blood for TEG analysis was moved into a 1.3 ml 3.2% sodium citrate tube, resulting in a 9:1 blood to citrate ratio. After blood collection, all citrate tubes were inverted gently five times to ensure adequate mixing of the anticoagulant and blood. This procedure was repeated on the opposite jugular vein using a different gauge needle. The procedure was conducted randomly to control for order effects.
TEG analysis
After collection, each citrate-containing tube was incubated in the upright position at room temperature (20–23°C) for 30 mins. Thromboelastographic analysis was performed using TEG (TEG 5000 Thromboelastograph Hemostasis Analyzer System; Haemoscope]. One millilitre of citrated blood was placed in a tube containing a kaolin activator (disposable TEG cups and pins, 0.2 M calcium chloride and kaolin vials; Haemoscope) and then inverted five times. The analyses were performed using pre-warmed TEG cups (disposable TEG cups and pins, 0.2 M calcium chloride and kaolin vials; Haemoscope] (37°C) filled with 20 μl 0.2 M calcium chloride, and then 340 μl kaolin-activated citrated blood was added to each cup within 1 min. After the addition of blood, the cup was immediately raised to the pin and analysis was started. Each sample was run for 60 mins, and R, κ, α, MA and global clot strength (G) were recorded from each channel.
Venepuncture difficulty scoring
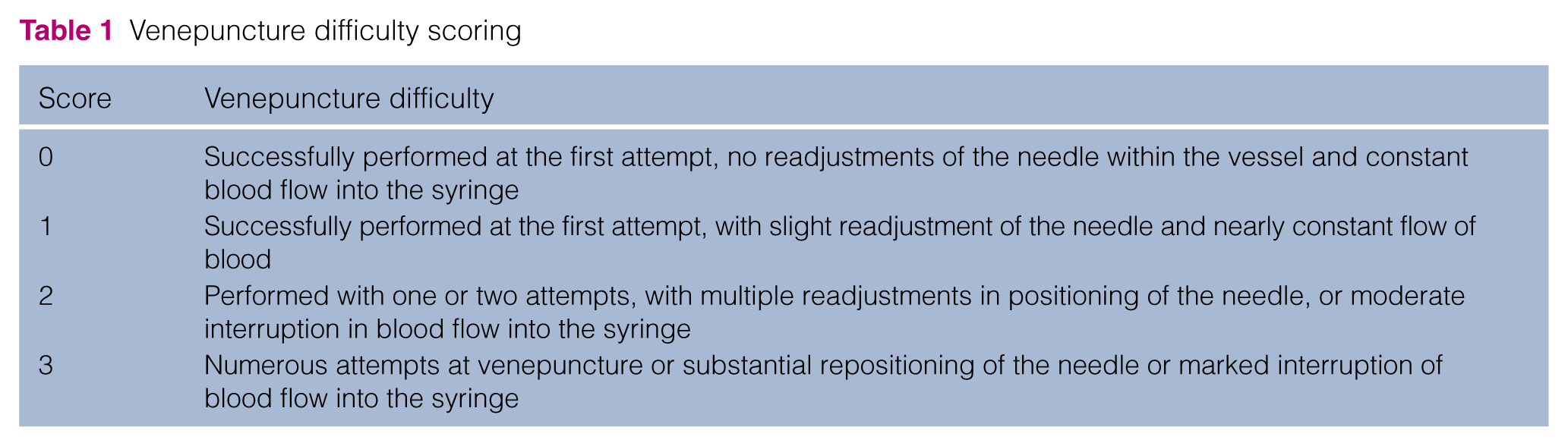
We applied the same venepuncture difficulty scoring method used in previous studies of dogs, which classified the success of venepuncture into four categories (Table 1). All sample collections were performed by one veterinarian. A single method was used to restrain each cat during venepuncture; one person held the cat’s front legs off the edge of the table, while another person extended the cat’s neck to point the nose to the ceiling.
Venepuncture difficulty scoring
Statistical analysis
R software was used for the statistical analyses and graph generation. Data for each TEG parameter were assessed for normality using a Shapiro–Wilk normality test (P >0.05). Paired t-tests were used to evaluate the null hypothesis and to determine that there were no differences between the values of R, κ, α, MA and G measured from the first and second samples (P <0.05). SDs and coefficients of variation for the population were calculated for each parameter. Individual box-and-whisker plots for R, κ, α, MA and G were plotted. Prior to analysis, the venepuncture difficulty score was dichotomised into difficult or not difficult categories; a score of 0 was considered not difficult, whereas a score of 1, 2 or 3 was considered difficult. This was done because there were few observations with difficulty scores of 1 or 2. The categories were compared via independent-sample t-test or Wilcoxon rank sum test.
Results
Of the 24 cats recruited into the study, only 17 were included in the analysis. Seven cats were excluded for reasons that included machine error (n = 2), abnormal aPPT test results (n = 2), TEG results that could not be measured (n = 2) and strong resistance during venepuncture (n = 1).
Physical examination and the results of the CBC, serum biochemistry and coagulation tests were within normal intervals in all 17 cats. The results of coagulation tests are shown in Table 2. Of the 17 cats included in the study, eight were castrated males, seven were spayed females and two were intact males. The breeds comprised 12 domestic shorthairs, two Persians, one Munchkin, one Siamese and one American Shorthair. The mean age of cats in this study population was 3.7 years (range 1–8 years).
Coagulation profiles in 17 clinically healthy cats
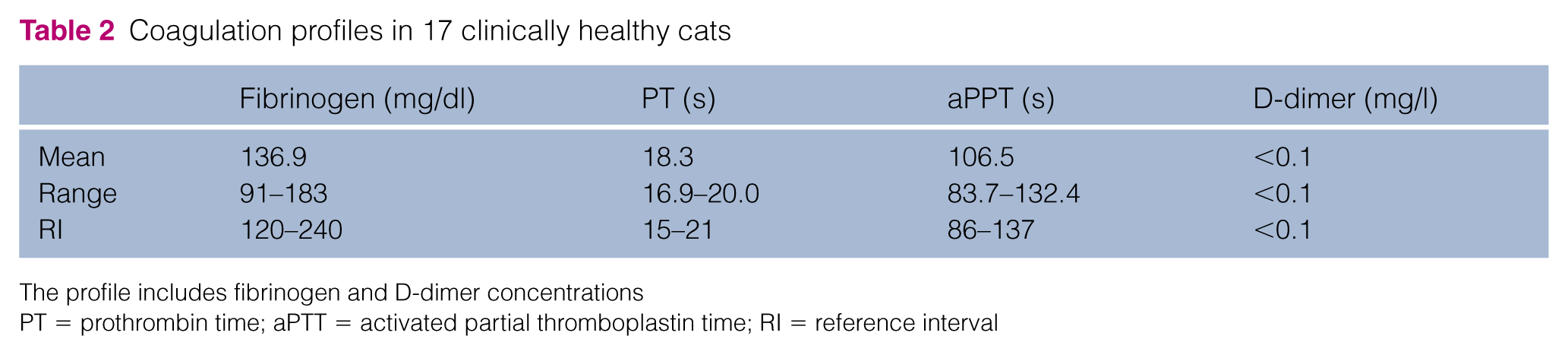
The profile includes fibrinogen and D-dimer concentrations
PT = prothrombin time; aPTT = activated partial thromboplastin time; RI = reference interval
The normality test showed that the results from all five parameters were normally distributed. The results of TEG in the 17 healthy cats are presented in Table 3. The paired t-test revealed that there were no statistically significant differences between the use of two different needles for R (P = 0.72), κ (P = 0.74), α (P = 0.99), MA (P = 0.08) and G (P = 0.09) (Figure 1).
Thromboelastography measurements in 17 clinically healthy cats

R = reaction time; κ = clot formation time; α = alpha angle; MA = maximum amplitude; G = global clot strength

Box and whisker plots depicting thromboelastography (TEG) results for two sampling methods used in 17 cats. Results are displayed according to the TEG variable: (a) R = reaction time; (b) κ = clot formation time; (c) α = alpha angle; (d) MA = maximum amplitude; (e) G = global clot strength. Circles represent outliers (value is less than the first quartile minus 1.5 times the interquartile range or greater)
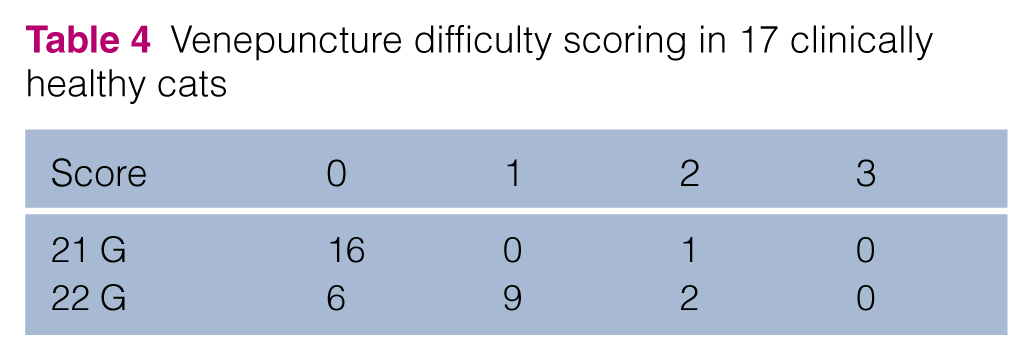
Of the 34 blood samples that were collected, 22 received a difficulty score of 0, nine had a score of 1 and three had a score of 2 (Table 4). Owing to the small number of samples with scores >1, difficulty scores were divided into two groups. Group 1 was assigned a difficulty score of 0 and group 2 was assigned difficulty scores ⩾1. The TEG results of group 1 and group 2 were then compared. Samples with difficulty scores ⩾1 were not significantly different from samples with difficulty scores of 0 with respect to R (P = 0.24), κ (P = 0.65), α (P = 0.65), MA (P = 0.72) and G (P = 0.77).
Venepuncture difficulty scoring in 17 clinically healthy cats
Discussion
It is known that venepuncture with a higher gauge needle can reduce patient morbidity, by alleviating discomfort during blood collection and reducing the risk of subsequent haemorrhage. 16 Therefore, in feline patients, an ideal needle size should be selected for safer blood collection; this depends on factors such as patient size, patient cooperation and predisposition to haemorrhage.
This study, which focused on blood sampling from 17 healthy cats, found no differences in TEG variables when 21 G and 22 G butterfly needles were used for blood collection via direct venepuncture. Shear stress, which is defined as the friction resistance of the blood vessel wall due to blood flow, is proportional to the flow rate and inversely proportional to the vessel diameter. 17 In human medicine, several authors have reported studies that evaluated whether collecting blood with different gauge needles affected shear stress levels and coagulation test results.18–20 These investigations have revealed that the use of a smaller diameter gauge needle causes higher shear stress on the blood cells as they pass through the needle, which increases the risk of haemolysis and the activation of platelets and the coagulation cascade; therefore, they can potentially affect coagulation test results. 19 Another study in humans revealed that blood obtained with a 25 G needle had significantly higher D-dimer concentrations and lower platelet counts than blood obtained with a 21 G needle. 18 However, these findings suggest that the differences in shear stress between the 21 G and the 22 G needle size does not affect TEG results in cats.
When trauma occurs in perivascular tissue, such as injury from multiple venous blood collection attempts, this leads to the release of tissue factor, which may initiate coagulation and activate platelets. 21 Therefore, redirection of the needle, which is indicated by a higher venepuncture difficulty score, resulted in a more rapid initiation of clot formation. 7 According to one canine study, mild-to-moderate venepuncture trauma significantly delayed R time in the kaolin-activated TEG, although it did not affect other TEG variables. 5 However, another canine study reported that there was no significant difference in kaolin-activated TEG parameters between the samples with difficulty scores of 0 and those with difficulty scores ⩾1. 6 In the present study, there was no significant difference in the TEG results between the two groups according to the score. These results may have been influenced by the fact that we performed TEG analysis using blood that had been collected after the first 1.5 ml had been drawn and discarded; this was done in an effort to mitigate the factor effect on high-scoring samples. 7 For this reason, the TEG guidelines also recommend that the first tube not be used for TEG, in order to minimise the effect of suboptimal venepuncture. 11 One canine study reported that if a clean venepuncture is achieved with little effect on tissue factors, results of the non-activated TEG analysis were not statistically different between blood from the discard tube and that from the second sample. 8 In cats, it is more difficult and challenging to perform venepuncture than in dogs, and several venepunctures performed during hospitalisation may lead to localised phlebitis. 7 Therefore, this study suggests that if venepuncture is difficult to achieve in cats, the initial blood sample should be discarded, and the subsequent collections of blood should be used as it may be more useful for TEG analysis.
This study was performed on clinically healthy cats to avoid the confounding factors of various medical conditions. An apparent limitation of this study was that a low number of cats were included. Therefore, it is unclear if significant differences might be found in larger study samples or in critically ill cats. Additionally, further study is needed to investigate the intra-individual variability in using 21 G and 22 G needles at two different time points in each cat. Venepuncture was performed through a syringe, resulting in delayed exposure to citrate anticoagulation. However, in many cats, blood collection through an evacuated tube can be limited because the small jugular vein may collapse from the force of the vacuum and the collection of blood into citrate-containing syringes is difficult to use commercially. 8
Conclusions
The results of this study suggest that 21 G and 22 G needles can be used for venepuncture in cats to safely collect blood samples for TEG analysis without affecting the results. There were no significant differences in the TEG values according to the venepuncture difficulty score when using samples collected after the discard tube. Therefore, the results of this study could be used as a reference that provides information on an effective method to collect blood for TEG analysis in cats.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.