
Abstract
Service robots with advanced intelligence capabilities can potentially transform servicescapes. However, limited attention has been given to how consumers experiencing vulnerabilities, particularly those with disabilities, envisage the characteristics of robots’ prospective integration into emotionally intense servicescapes, such as long-term care (LTC). We take an interdisciplinary approach conducting three exploratory studies with consumers with disabilities involving Community Philosophy, LEGO ® Serious Play ® , and Design Thinking methods. Addressing a lack of consumer-centric research, we offer a three-fold contribution by 1) developing a conceptualization of consumer-conceived value of robots in LTC, which are envisaged as a supporting resource offering consumers opportunities to realize value; 2) empirically evidencing pathogenic vulnerabilities as a potential value-destruction factor to underscore the importance of integrating service robots research with a service inclusion paradigm; and 3) providing a theoretical extension and clarification of prior characterizations of robots’ empathetic and emotion-related AI capabilities. Consumers with disabilities conceive robots able to stimulate and regulate emotions by mimicking cognitive and behavioral empathy, but unable to express affective and moral empathy, which is central to care experience. While providing support for care practices, for the foreseeable future, service robots will not, in themselves, actualize the experience of “being cared for.”
Keywords
Introduction
Service robots are a physically embodied form of artificial intelligence (AI) that are attracting exponentially growing attention (McLeay et al. 2021). Defined as “system based autonomous and adaptable interfaces that interact, communicate and deliver service” (Wirtz et al. 2018, p. 909), robots offer the prospect of remarkable and revolutionary changes in service delivery and experiences (Mende et al. 2019). A key challenge, however, will be to ensure that these changes increase the provision of fair opportunities and choices for receiving and co-creating value from service (Williams et al. 2020). This challenge emerges from the contemporary shift in research and practice toward service inclusion—a paradigm that requires service providers to anticipate, diagnose, and rectify problems that might preclude or disadvantage some consumers from realizing value in a service experience (Boenigk et al. 2021; Fisk et al. 2018). Adopting a service inclusion perspective in early stages of research on robots’ integration into services can facilitate avoiding problems that have characterized “traditional” servicescapes (e.g., non-accommodation for visual impairments in retail design; Baker 2006).
A service inclusion perspective is inherently consumer-centric, in that it requires service concepts, systems’ architecture, and frontline interactions to cater for the precise needs and circumstances of all potential consumers. In particular, this includes consumers who may be disadvantaged (through belonging to a group potentially targeted for discrimination, such as ethnic minorities or women) or experience vulnerabilities (through lacking power and control) in service exchanges (Fisk et al. 2018). A focus on service inclusion can enable service providers to anticipate and address aspects of a servicescape that might preclude these consumers from realizing (i.e., receiving and co-creating; Fisk et al. 2018) value and thus enhance social justice and consumer wellbeing (Anderson and Ostrom 2015). However, the factors impacting the (non)acceptance of robotic interactions in servicescapes are largely understudied from the consumer perspective. This is the case for broad consumer populations (Xiao and Kumar 2021(Xiao & Kumar, 2021)) and specifically for consumers experiencing vulnerabilities (Huang et al. 2021). We argue that, if service research is to answer calls for making a positive impact to the lives of vulnerable consumers (Huang et al. 2021), it must address the fundamental question of whether consumers consider robotic service agents to provide significant potential to relieve or, conversely, exacerbate vulnerabilities. The current absence of a consumer perspective represents a significant gap in our understanding of how, and under what conditions, robots might facilitate consumers realizing greater or lesser value in servicescapes.
Emotion-intense services, such as long-term care (LTC), provide a compelling setting for beginning these explorations. Robots are perceived as a key potential solution to a looming crisis in the LTC service sector, in which rapidly increasing demand 1 will be accompanied by significant labor shortages (Osterland 2021; Spetz et al. 2015). Care is consumed when people face threats to their wellbeing. The care service experience can thus be emotionally fraught and has the inherent potential to ameliorate and/or exacerbate consumer vulnerabilities (Berry et al. 2020). Prior research on the integration of non-robotic technologies in care service demonstrates dual, sometimes diametrically opposed, changes in the value consumers are able to realize. For instance, in medical care, electronic patient records can improve the continuity of care provision, but also limit consumers’ ability to control data informing decisions on the type of care they receive (e.g., curative vs palliative; Berry et al. 2020).
The small number of studies concerned with robot integration into care service highlights the possibility of similar dual impacts. For example, robots may create value by motivating physical exercise but destroy value by invading space (e.g., Čaić, Oderkerken-Schroder and Mahr 2018; Deutsch et al. 2019). Uncertainties regarding whether AI will replace or augment human care agents are also considered to be a significant factor in continued consumer resistance toward the deployment of robots in this context 2 (Longoni, Bonezzi and Morewedg 2019; Van Doorn et al. 2017). While these initial insights are drawn from the contexts of medical care (Agarwal et al. 2020) and care for the elderly (Čaić et al. 2018, Čaić, Mahr and Oderkerken-Schröder 2019; Melkas et al. 2020), holistic consumer-informed knowledge concerning the implications of robots’ integration into care servicescapes is in its infancy. Extant research has largely overlooked the robot-integrated LTC servicescape—a particularly complex context that extends beyond medical and elderly care. LTC incorporates a wide range of services (e.g., personal, social, and medical; Grabowski 2008) as it is something that is often required by everyone who faces health circumstances without “quick cure” possibilities, regardless of age (e.g., stable disabilities or long-term illness with prognoses of recovery or deterioration). Against the backdrop of crisis in LTC, the deployment of AI and robotic technology is vital in addressing resource shortages (Tan and Taeihagh 2020). Yet consumer willingness to accept robots as caregivers remains uncertain (Deutsch et al. 2019).
In this paper, we—a team of consumer, service marketing, sociology, healthcare technology, and engineering design researchers—explore how consumers with disabilities envisage the potential value of robots in LTC, and the vulnerability-inducing factors that may impact their acceptance. We ground our study in the perspectives of consumers with disabilities because it is a population that has been subject to significant marketplace exclusion and constitutes a group of potential LTC consumers with a heightened propensity for experiencing vulnerability (Fisk et al. 2018; Higgins 2020). Adopting a consumer with disabilities’ perspective can thus offer valuable directions for designing inclusive service concepts for complex, emotion-intense service, and for care service in particular.
Our objective is to develop a consumer-centric conceptualization that illuminates how the integration of robots in LTC service might contribute to (or detract from) consumer opportunities to realize value in terms of enhanced wellbeing. We achieve this objective by drawing on three multi-method qualitative studies, conducted as part of a wider and ongoing program of research exploring robots in the context of LTC. Following a grounded theory approach (Gioia, Corley and Hamilton 2013; Strauss and Corbin 1998), we examine insights from consumers with disabilities concerning what care constitutes as a service experience and how robots are envisaged in this context. We synthesize the emergent consumer characterizations of robots in LTC by drawing on the notion of conceived value, that is, how value is envisaged in the absence of prior experience (see Hardyman, Kitchener and Daunt 2019; McGinn 2004). We theorize that the consumer-conceived value of LTC robots is mitigated by conceptions of potential pathogenic vulnerabilities—a perverse effect of a change aimed at ameliorating existing vulnerabilities, whereby new vulnerabilities arise (Lange, Rogers, and Dodds 2013). Pathogenic vulnerabilities emerge as a key factor influencing consumer conceptions of how robots might enhance or detract from the realization of value.
Our study responds to calls for interdisciplinary research that explores how inclusive technology-integrated service (re)design can offer opportunities to enhance value-centered care and improve consumer wellbeing, particularly amongst those experiencing vulnerability (Anderson, Nasr and Rayburn 2018; Huang et al. 2021). Specifically, we provide three distinct theoretical contributions. First, by conceptualizing the consumer-conceived value of robots’ integration into LTC servicescape, we show that robots are envisaged as a supporting and (to an extent) emotion-regulating resource, which can a) augment a human-facilitated LTC service offering and b) postpone or reduce the need to consume LTC service. Second, by empirically evidencing that consumers conceive robots might mitigate existing vulnerability, whilst also potentially inducing pathogenic vulnerability experiences, we offer an explanation for consumer resistance to the idea of robots in LTC. In this respect, the service inclusion perspective provides important insights into the factors informing robots’ (non)acceptance. Third, by showing that consumers do not envisage AI to be capable of affective and moral dimensions of empathy, we illuminate a deep-seated belief amongst consumers that “robots cannot care.” This provides an important clarification of prior theorizations of robots’ empathetic and emotion-related AI capabilities (Huang and Rust 2021; Wirtz et al. 2018).
Informed by guidance on presenting grounded theory-based studies (Gioia et al. 2013), the paper follows a conventional structure. We first present literature concerned with concepts that informed our conceptualization. We then outline the data collection and analytical procedures, followed by findings that are integrated in a conceptualization of consumer-conceived value of robots’ integration in a LTC servicescape. For clarity, our empirical analysis guided initial consultations with the literature, and our conceptualization was developed through iterating between findings and literature.
Conceptual Background
Service Inclusion: An Important Lens for Conceptualizing Robot-Integrated Service
Advancing socially just service systems is a vital priority for contemporary service research (Field et al. 2021). Crucially, this entails going beyond “simply replicating established research with vulnerable groups of consumers” [and] “tackling new problems faced by these consumers that have the potential to improve their quality of life and wellbeing” (Huang et al. 2021, p. 460). Addressing this priority is at the heart of the concept of service inclusion (Fisk et al. 2018) which stems from a transformative service research family of initiatives (e.g., Anderson and Ostrom 2015; Boenigk et al. 2021; Sandberg et al. 2021). Exclusion from service can harm consumers’ wellbeing by depriving them of opportunities to fully realize (e.g., receive and co-create) value as a result of systemic biases, discrimination, and customer vulnerability (Fisk et al. 2018). Consequently, service inclusion entails a multi-level service (re)design paradigm that targets the causes of exclusion to improve consumer wellbeing. It does so by developing 1) inclusive service concepts—identifying what consumers experiencing exclusion need and want and developing offerings that eliminate or mitigate causes of exclusion; 2) service systems that promote inclusion through system architecture and navigation; and 3) processes for inclusive service interactions (Fisk et al. 2018). Taking theoretical direction from service inclusion perspective, this paper is founded on a premise that the design of robot-integrated service requires consumer-informed service concepts.
Because service inclusion highlights the importance of grounding service concepts in consumer views of what constitutes value,
The concept of perceived value is defined in health and social care contexts as “perception of benefits received for burdens endured” (Berry et al. 2020, p. 1). It encapsulates the notion that a service concept offering consumers meaningful value rests on understanding the service resource(s) characteristics that they consider important for enhancing, as opposed to burdening, their wellbeing (Anderson, Narus, and van Rossum 2006). However, where consumers have not experienced a given service resource (e.g., where new technologies, such as AI, are yet to be designed and deployed within a particular service), conceived value is arguably a more pertinent notion to consider. Conception is defined as “an idea of what something or someone is like” (Cambridge Dictionary 2021). Hence, conceived value entails how consumers envisage the nature of value in a given experience, and how this might be realized via interaction with particular service resources (McGinn, 2004; see also, Hardyman, Kitchener, and Daunt, 2019).
The development of inclusive service requires an understanding of what may deprive consumers in disadvantaged and/or vulnerable circumstances from realizing value (Fisk et al. 2018). Therefore, in the context of robot-integrated services, it is necessary to consider how consumers conceive robots as new resources that impact (improve or limit) their opportunities for realizing value. In a consumption encounter, vulnerability entails a dependency on marketized (private or public) systems providing goods and services to enable the individual to function, whereby a lack of or restriction in access or control over these resources renders a person unable to realize value (Fisk et al. 2018; Hill and Sharma 2020). That is, (in)sensitive service design and delivery can increase consumer vulnerability if it prohibits the freedom of choice necessary for receiving a fair service. Conversely, it can “render consumers less vulnerable” by eliminating barriers and empowering consumers to realize value from a service offering (Baker, Gentry and Rittenburg 2005; Shultz and Holbrook 2009, p. 126).
On this basis, and to gain a complete understanding of consumer-conceived value in robot-integrated LTC servicescape, we explore consumer conceptions of a) care, in terms of what constitutes value in an overall care service experience and the vulnerabilities that might preclude the realization of value in care; and b) whether, how and why the integration of robotic care service resources might enhance or detract from the realization of value in care. To situate our inquiry in the extant literature, the following sections synthesize concepts, findings, and debates in two key areas: i) care itself and ii) the integration of robots into LTC.
Understanding Consumer-Conceived Value in Care Service
Value in care consumption experience: an integrated conceptualization
Defining care as a social experience remains a contested terrain (Edwards 2009). Here, we draw on the seminal ethical perspective on care developed by Tronto (1993), and subsequently extended by Puig de la Bellacasa (2017), to define care in terms of the three components by which it is actualized: cognitive care (recognizing a need for care), emotional care (taking care of: having a concern for and assuming the responsibility to provide care and feeling cared for: experiencing care as a response to one’s needs), and care action (participating in care as a giver or receiver). Actualization of care is generally recognized as activities by those participating in care (givers—Wilkes and Wallis 1998; receivers—Söderhamn, Dale, and Söderhamn 2013) whereby they draw on abilities, competences, ethical codes, and resources to materialize care with a goal of restoring, sustaining, or improving wellbeing. Three pertinent considerations follow: 1) actualizing care incorporates emotions with particular practices; 2) care is co-actualized through interactions between givers and receivers; and 3) determining whether care has been actualized requires consideration of the outcome(s) as experienced by care recipient(s). Hence, the value in care as a service offering rests upon how those being cared for (care consumers) conceive of care attributes essential for their wellbeing.
A deeper understanding of what underlies care recipients’ conception of essential care attributes and determination of whether actualization of care has taken place is afforded by the concept of empathy. Empathy is often regarded as a primary attribute of good care by those receiving it (Mercer and Reynolds 2002). Simply, empathy represents a foundation of a helpful interaction sought to satisfy the basic human need of being understood (Kunyk and Olson 2001). In assimilating the extant literature to consider empathy in the context of care, Jeffrey (2016) identifies four interacting dimensions that correspond with care actualization components discussed above: 1) cognitive empathy—comprehending another’s emotions; 2) affective empathy—sharing and re-experiencing the feelings of others; 3) behavioral empathy—acting and communicating in therapeutic ways, as needed by others; and 4) moral empathy—genuine compassion for the others and an altruistic motivation to improve their wellbeing (Irving and Dickson 2004; Morse et al. 1992). The opportunity to realize an experience of an empathetic, therapeutic interaction that engages their perspectives in determining and pursuing wellbeing outcomes is key to consumer conceptions of value in care. A quote from a healthcare consumer in Berry and Bendapudi (2007, p. 113) eloquently illustrates this: “We want doctors who can empathize and understand our needs as a whole person. […] every doctor needs to know how to apply their knowledge with wisdom and relate to us.”
Together, the integrated conceptualization of care and empathy (in terms of their shared cognitive, affective, behavioral, and ethical/moral dimensions), provides a useful theoretical foundation for informing the design of care service that offers consumers opportunities to realize value. There is a recent momentum toward (re)designing care service to foreground consumer perspectives on value in care, for diagnosing and addressing factors that maximize or limit the wellbeing outcomes—and, consequently, value—sought by consumers across the entire care experience (Anderson et al. 2018; Berry et al. 2020). To conceptually explicate how these factors occur, we consider consumer vulnerability in care servicescapes.
Consumer vulnerability in care servicescapes
Care is a service whereby consumer expectations and evaluations of both utilitarian and experiential dimensions of service resources are emotionally intense (Agarwal et al. 2020; Berry et al. 2020). Often, the need for care is associated with experiencing concern, perceived helplessness due to lacking specialist knowledge and skills required for (some) care practices, and anxiety over potential outcomes (Anderson et al. 2018; Berry et al. 2020). Hence, the wellbeing outcomes consumers seek in care servicescapes are multidimensional, ranging from physiological, to psychological, to affective (Agarwal et al. 2020).
Further, consumers seek to be engaged in decisions regarding their care and its design, yet this engagement can place a variety of burdens upon them (Anderson et al. 2018; Berry et al. 2020). These burdens can include regulating emotions associated with needing and receiving care, identifying care provider(s) that feel safe and trustworthy, managing records or prescribed self-care practices, and preserving a sense of self and independence (Agarwal et al. 2020; Baker et al. 2005; Berry et al. 2020). From this perspective, another important wellbeing outcome sought from the care service (and thus, a component of conceived value) is for some of these burdens to be alleviated by mitigating consumer vulnerability potential (Anderson et al. 2018; Berry et al. 2020). That is, the burdens people might endure in themselves do not necessarily render a person vulnerable as a consumer (Sandberg et al. 2021). However, the propensity for experiencing consumer vulnerability is inherently significant, particularly if one requires care for a serious health condition (Agarwal et al. 2020; Berry and Bendapudi 2007). Consumer vulnerability occurs if the encounters with care service limit a person’s ability to access care resources, and to exercise agency in which resources are utilized, and how, to transform burdens into manageable circumstances (Baker et al. 2005; Sandberg et al. 2021). Hence, the (re)design of service concepts entails adaptation of care resources’ offering such that consumer vulnerability sources are mitigated, and conceptions of value in care are realized.
The potential impacts of service (re)design initiatives should be examined holistically. Even well-meaning efforts to mitigate existing vulnerabilities might unintentionally give rise to pathogenic vulnerabilities—a perverse effect of a change in an external environment aimed at ameliorating existing vulnerabilities, whereby new vulnerabilities are generated (Lange et al. 2013). Sandberg et al. (2021) recently exemplified such effects, albeit without pathogenic vulnerability underpinnings, in a study of people consuming care in nursing homes. In their findings, mitigating the circumstances of deteriorating physical security (e.g., being at risk of sustaining injuries) increased consumer feelings of diminishing autonomy, and vice versa. Hardyman et al. (2019) have shown that consumer conceptions of whether a care service resource enhances or limits the conceived value of care experience is dependent on conceived nature of the resource; which we understand to be the total of this resource’s characteristics and role in the experience. Thus, consumer evaluations of a care service resource will entail appraisal of 1) benefits a resource offers, including whether it might mitigate existing vulnerabilities vs 2) pathogenic vulnerabilities that may arise from the resource.
Holistic consideration of the potential impact of resource innovations is particularly crucial as care service continues to undergo what Rust and Huang (2014) term the “service revolution,” facilitated by the widespread integration of new technology resources (Berry et al. 2020). Technology resources offer promise for improving the efficiency and effectiveness of care services, such as safety, convenience, and consistency in accessing consumer records and care providers, analyzing which consumers are benefitting from, or are disadvantaged by, particular care options, safeguarding from diagnoses errors and mitigating work pressures for caregivers (Agarwal et al. 2020; Berry and Bendapudi 2007). Concurrently, integration of technology resources might inadvertently raise barriers to access for culturally and socio-economically underserved consumer populations (Agarwal et al. 2020) and minimize or eliminate the relational, empathy-centered care attributes (Anderson et al. 2018).
In summary, understanding consumer conceptions of the value that the integration of robots into care service might create, and the potential barriers to realizing this value, requires contextualized consideration of how robots are envisaged as care service resources. With this in mind, we next introduce the context for our study, long-term care (LTC) service, and review extant knowledge on consumer perspectives of robot-integrated LTC servicescape.
Long-Term Care (LTC) and Current Knowledge on Robots’ Integration in LTC Servicescape
LTC is representative of care servicescapes that are associated with prolonged consumption and complex, large-scale systems where the potential for consumer vulnerability is greatest (Berry et al. 2020; Spanjol et al. 2015). LTC incorporates a wide-ranging set of services required over a sustained period of time by consumers whose abilities to perform daily living tasks, such as preparing food or dressing, are permanently or temporarily (with a prolonged effect) impaired (Grabowski 2008). This may include people living with stable disabilities or a long-term illness, or those with diminishing capacity, as in case of elderly people, or people with deteriorating health conditions. A majority of people may require LTC at some point in their lives; as Kane (2001, p. 295) asserts, “LTC
While systems and structures of LTC service vary across national contexts, they can be broadly classified as personal and social support, treatment maintenance, and rehabilitative and palliative care; their provision can thus include elements of both social and medical care (Grabowski 2008; Spetz et al. 2015). According to Kaye, Harrington, and LaPlante (2010), in the USA alone, 10.9 million people (half of whom are non-elderly) consume LTC in non-institutional settings, residing in communities; while 1.8 million (predominantly elderly) people consume LTC in institutional settings, residing in care facilities. Globally, 2.3 billion people will require LTC in 2030, with demand expected to continue rising due to age longevity and the growing prevalence of long-term conditions (International Labor Organization 2018; OECD 2021).
The mounting concerns over the “crisis of LTC” drive surging global interest in integrating robotic technologies in LTC service (International Labor Organization 2018; Osterland 2021). LTC robotics is a rapidly growing field of research and industry (Maalouf et al. 2018), and a stream of robots for rehabilitation, hospital, and home-based care have, or are about to, enter the market and, consequently, LTC servicescape (Kyrarini et al. 2021).
However, nascent evidence highlights that consumer recognition of the benefits robots can offer is accompanied by a persistent resistance to their deployment in LTC service. For example, already-developed robots have been withdrawn from production after being rejected by consumers (Wang et al. 2017; also see Broadbent, Stafford and MacDonald 2009). This resonates with the service literature assertions that “the factors impacting customer acceptance of robotic interactions in the service context, and the factors that impede adoption need to be thoroughly addressed but remain largely understudied thus far” (Xiao and Kumar 2021, p. 13). A concurrent trend is criticism of “traditional” LTC services’ design and delivery for prioritizing care providers’ perspectives, with calls for consumer-centric (re)design (Anderson et al. 2018; Batavia 2002). Hence, grounding the development of robot-integrated LTC service in how consumers conceive the value of robots in LTC, and the potential barriers to realizing this value, is crucial to both alleviating the “LTC crisis” and advancing service inclusion.
Robots’ characteristics (which incorporate capabilities and attributes—see Wirtz et al. 2018) are highlighted as central to how humans (consumers and/or service staff) will conceive of, and respond to, integration of robots in servicescapes (Simon, Neuhofer, and Egger 2020; Wirtz et al. 2018). Yet consumer-informed conceptualizations of robot characteristics and their role in LTC service experiences are sparse in service research. A handful of studies theoretically propose that in complex, emotion-laden service contexts, such as medical care, consumers may expect robots to possess specific characteristics addressing a wide variety of functional, socio-emotional, and relational needs (Mende et al. 2019; Van Doorn et al. 2017).
The general service literature concerned with systematically characterizing AI capabilities for service delivery offers complementary perspectives (Van Doorn et al. 2017; Wirtz et al. 2018). Huang and Rust (2021), for example, conceptualize three levels of AI capabilities, whereby each consecutive level is more complex: 1) mechanical AI involves capabilities related to standardized routine tasks; 2) thinking AI integrates mechanical, analytical, and intuitive capabilities through which the service actions AI performs can be personalized; and 3) feeling AI is a futuristic projection of technology that, along with mechanical and thinking AI, will possess capabilities to “recognize, emulate and respond appropriately to human emotions” (Huang, Rust and Maksimovic 2019, p. 46). As there have been few applications of thinking and feeling AI so far (Čaić et al. 2019), whether and how consumers perceive these capabilities to add to, or detract from, the value they might realize from service experiences is little understood and subject to “considerable debate” (Wirtz et al. 2018, p. 913).
The lack of consensus concerning how consumers envisage the value potential of service robots in the service literature can be attributed to the dominance of conceptual and experimental approaches examining consumer responses to robot(s) with pre-determined service functions in contexts characterized by relatively simple, short-term interactions, such as restaurants, hotel or airline check-in, and shop assistance (McLeay et al. 2021). Recent comprehensive literature reviews (see Mende et al. 2019; Xiao and Kumar 2021), and studies published since these reviews, highlight that current research mainly focuses on the technical and functional attributes informing robot acceptance, usually utilizing quantitative methods (Jörling, Böhm and Paluch 2019; Xiao and Kumar 2021). Indeed, only 4 of the 43 studies in Mende et al.’s (2019) and Xiao and Kumar’s (2021) reviews adopt open, qualitative approaches that afford consumer-informed, contextualized explorations.
An interdisciplinary review of the literature on LTC robots, conducted as part of this study (presented in Appendix 1, supplementary online material), provides an overview of the current state of knowledge in this area. Studies in the context of social care offer useful conceptual and empirical insights into the ambidextrous nature of consumer sentiment concerning robots’ characteristics and their role in realizing value in care (Čaić et al. 2018; Henkel et al. 2020; Longoni et al. 2019). For instance, a robot’s cultural competency can enhance the emotional wellbeing of elderly care home residents (Papadopoulos et al. 2021). However, elderly consumers can also see LTC robots as intruders violating privacy and taking up valuable space (Čaić et al. 2018). The focal point of the majority of studies (e.g., Čaić et al. 2018; Longoni et al. 2019; Melkas et al. 2020; Tuisku et al. 2019) is on institutional LTC settings with elderly adults as care recipients. With exceptions (Čaić et al. 2018; Wang et al. 2017), empirical research mainly focuses on understanding the perceptions of specialists and caregivers. A small selection of studies delineate forms of vulnerability experienced by specific consumer groups (e.g., elderly, young consumers; Henkel et al. 2020; Papadopoulos et al. 2021), but rarely examine the relationship between vulnerability and robots’ (non)acceptance.
Most empirical research has focused on robots that exhibit low levels of primarily mechanical AI capabilities, in contrast to many recent conceptual papers in leading service journals that call for consideration of more advanced capabilities (Huang and Rust 2021; Van Doorn et al. 2017). In comparison to the general services literature that is starting to explore attributes informing robot acceptance (Jörling et al. 2019; Simon et al. 2020), most studies on robots in LTC lack a specific focus on attributes, particularly regarding how social attributes, in comparison to functional attributes, may influence consumer responses (exceptions include Čaić et al. 2018, 2019). A handful of studies explore how anthropomorphism (humanoid vs non-humanoid) attributes affect trust (Erebak and Turgut, 2019), and how behavioral (speech, mobility), appearance (size), and functional attributes relate to wellbeing (Henkel et al. 2020).
Several studies have sought to gain empirical insights to address very specific practical problems (e.g., Deutsch et al. 2019; Melkas et al. 2020; Wang et al. 2017), which, whilst of value, are necessarily limited in terms of theoretical advancement. Few efforts adopt a service inclusion, or—more broadly—transformative service research perspective to explicitly examine or develop customer-centric service concepts, systems, and interactions, following a multi-level service design framework (see the 3 inclusive service design columns in Appendix 1; Henkel et al. 2020 is an exception). Robotic design research is increasingly adopting user-centered (or participatory) approaches to accommodate consumers’ personal, environmental, and social experiences and contexts alongside technological solution(s) (Ármannsdóttir et al. 2020). Yet, user perspectives continue to be mainly restricted to evaluation of a product that “researchers have envisioned and developed for a certain purpose or task” (Reich-Stiebert, Eyssel and Hohnemann 2020, p .228), leading to a potential mismatch. For example, Bradwell et al. (2019) demonstrate striking differences in the visions of companion robots held by older adults and roboticists. The majority of empirical service research mirrors the focus on consumers’ perceptions of an already-developed robot (Longoni et al. 2019; Papadopoulos et al. 2021).
In our exploratory study, we focus on how consumers with disabilities conceive the value of robots’ integration into LTC servicescape. We thus seek to extend the body of knowledge summarized in previous paragraphs by eliciting consumer perspectives that were not restricted by specified robot design, appearance, or functionality/task orientation, and by reaching beyond institutional LTC and elderly consumer group boundaries. Our reasoning specifically builds upon the contributions by studies that examined value creation/destruction potential in robots’ integration into social care (e.g., Čaić et al. 2018; Henkel et al. 2020). We deemed that an open, qualitative exploration will afford a more holistic perspective into consumer-conceived value implications of LTC service (re)design integrating robots.
Method
Approach and Data Collection
The findings presented in this paper stem from a wider ongoing interdisciplinary program of research (titled Improving Inclusivity in Robotics Design) which is exploring innovations in methodological approaches for integrating user viewpoints in the conceptual design of robots for care. 4 Explorations of user viewpoints were grounded in the lived realities of people with disabilities, since early knowledge exchanges in the entire research team indicated that, while care robotics research outside of the service robots domain advocates user-centered design, grounding in the “social, emotional and practical contexts where care is given and received” (Van Aerschot and Parviainen 2020, p. 247) remains a challenge.
The data comprising of user viewpoints lends itself to examination from a service research perspective. As a population subjected to marketplace exclusion, consumers with disabilities generally possess a heightened propensity for experiencing consumer vulnerability (Fisk et al. 2018; Higgins 2020). As one of the groups potentially requiring LTC (Grabowski 2008), consumers with disabilities can provide focused insights into the conceived value robots in LTC may offer and vulnerability-inducing factors that might preclude this value realization.
The data were collected via three focus groups, taking form of workshops, with 20 people with disabilities in the United Kingdom, drawing on methodologies encompassing different types of qualitative elicitation techniques that belong to the following broad categories (see Barton 2015; McLafferty 2004; McMahon et al. 2016): semi-structured group interviewing (Study 1); guided storytelling with construction tasks (Study 2); and a combination of brainstorming and explanation tasks (Study 3). The rationale for deploying different methodologies was encouraged by transformative service and consumer research literature recommendations to apply varied and innovative methodological approaches, particularly when engaging with consumer stakeholders experiencing vulnerabilities (Boenigk et al. 2021; Ozanne and Fischer 2012). Study 1 utilized Community Philosophy—a method encouraging grassroots communities’ collaborative philosophical thinking on issues of common concern (Bramall 2020), akin to dialogical practices in co-research (Frank 2005). Study 2 utilized LEGO® Serious Play®—a method integrating cycles of building tasks (utilizing specialized kits) with sharing and reflecting facilitated by questions whereby metaphorical explanations elicit concepts from participants’ imagination (Rasmussen 2006; Simon et al. 2020). Study 3 utilized Design Thinking—a method drawing on industrial design tools for facilitating group ideation of innovative consumer offerings (Brown 2008; Seidel and Fixson 2013).
To ensure consistency across studies and following Gioia et al.’s (2013) recommendations to guide an open qualitative inquiry with an overarching question, all workshop protocols were guided with a question specified as follows: how do people with disabilities envisage the qualities of a useful robot? Subsequent tasks and probes built on the guiding question. Three authors of this paper worked with facilitators trained in each method to ensure alignment of the methodological protocols with the guiding question, while agreeing the adaptations required by each methodology’s specifics. Each facilitator conducted the workshop pertaining to their training, with one member of the author team acting as co-facilitator and observer. 5 Further details of methodologies and the adopted protocols are provided in Appendix 2, supplementary online material. All workshops were conducted in autumn 2020, and—owing to the Covid-19 pandemic restrictions—took place online. The workshops were audio and video recorded with participants’ consent and assurance of anonymity in all data outputs.
Participants
Participants were recruited via a market research agency. In line with ethical considerations that underpinned the studies’ design, we briefed the agency to recruit people with physical disabilities only, since the specialist competences and skills required for conducting research with people with cognitive and mental health disabilities were beyond the skillset of the research team members. While applying this recruitment filter, we aimed to broaden democratic validity (Ozanne and Saatcioglu 2008) by employing a maximum variation sampling strategy (Patton 1990). Specifically, we screened self-reported type(s) of physical disabilities, age, ethnicity, and gender, with the aim of recruiting participants with varied backgrounds. Owing to the online data collection format and the requirements of employed methodologies, participants were asked to confirm that they were comfortable with, or had adequate assistance for, typing, manipulating small objects, and viewing, listening to, and speaking at the workshop via a video conferencing platform (Zoom).
The final sample comprised 20 participants aged between 26 and 74, with a range of reported occupations (full time employment, self-employment, stay at home parent, and retired) and disabilities (visual and hearing impairments, health conditions impacting mobility, and the capacity for physical activities). Nine participants identified as female (11 as male), five as Black or Asian (15 as white). Each participant was allocated into a workshop through a combination of maximum variation sampling, participant availability, and expressed interest in a workshop (based on briefs provided in final recruitment stages). Thus, each individual participated in one study: eight in Study 1; and 6 and 6 in Studies 2 and 3. Appendix 3 (supplementary online material) details sample characteristics and workshop allocations.
Data Analysis
The audio recordings of all workshops were transcribed verbatim, yielding 145 pages of single-spaced text. The analysis strategy followed Gioia and colleagues’ (Corley and Gioia 2004; Gioia et al. 2013) recommendations for systematically organizing the analyses while allowing for “a flexible orientation toward qualitative, inductive research that is open to innovation” (Gioia et al. 2013, p. 26). We began by subjecting the transcripts to open coding (Corley and Gioia 2004), conducted by three authors of this paper. The open coding stage encompassed identifying particular characterizations of and reasonings about care and/or robots in the context of care articulated by participants and coding these into first-order concepts (articulations). The first-order concepts represent in-vivo codes reflecting expressions by participants or a simple phrase describing these expressions (Strauss and Corbin 1998).
Two authors first coded each workshop transcript independently, while a third author read through the transcripts without coding. On completion, the three met to cross-check, discuss, and reconcile the identified first-order concepts, following the constant comparative method (Glaser and Strauss, 1980) to examine concepts identified within and between workshops for differences and similarities. Some concepts were identified across all workshops; others in one or two in different combinations. The full author team of this paper subsequently used axial coding to apply our interpretations. This stage was an iterative process whereby we went back and forth between the first-order in-vivo codes and the literature to identify relevant theoretical concepts; this informed categorization of the first-order concepts into broader second-order analytical themes (Corley and Gioia 2004). The analytic themes were then conceptually related to aggregate dimensions (see Appendix 4, supplementary online material, for the final data structure framework). The open coding was conducted manually; Inspiration 9.2 6 mapping software was utilized to organize and visualize the developed thematic structure.
Findings: Conceptualizing Consumer-Conceived Value of Robots in LTC Servicescape
Two aggregate dimensions emerged as we theorized our data in consultation with the literature. We describe these dimensions as 1. Conception of Care and 2. Conception of Robots in LTC Servicescape. By considering how themes from both aggregate dimensions relate to each other holistically, we derived a conceptualization of consumer-conceived value of robots’ integration in LTC servicescape, represented graphically in Figure 1. In the paragraphs that follow, we provide an overview of derived conceptualization, before offering a detailed presentation of two dimensions derived from the findings. A conceptualization of consumer-conceived value of robots’ integration in LTC servicescape.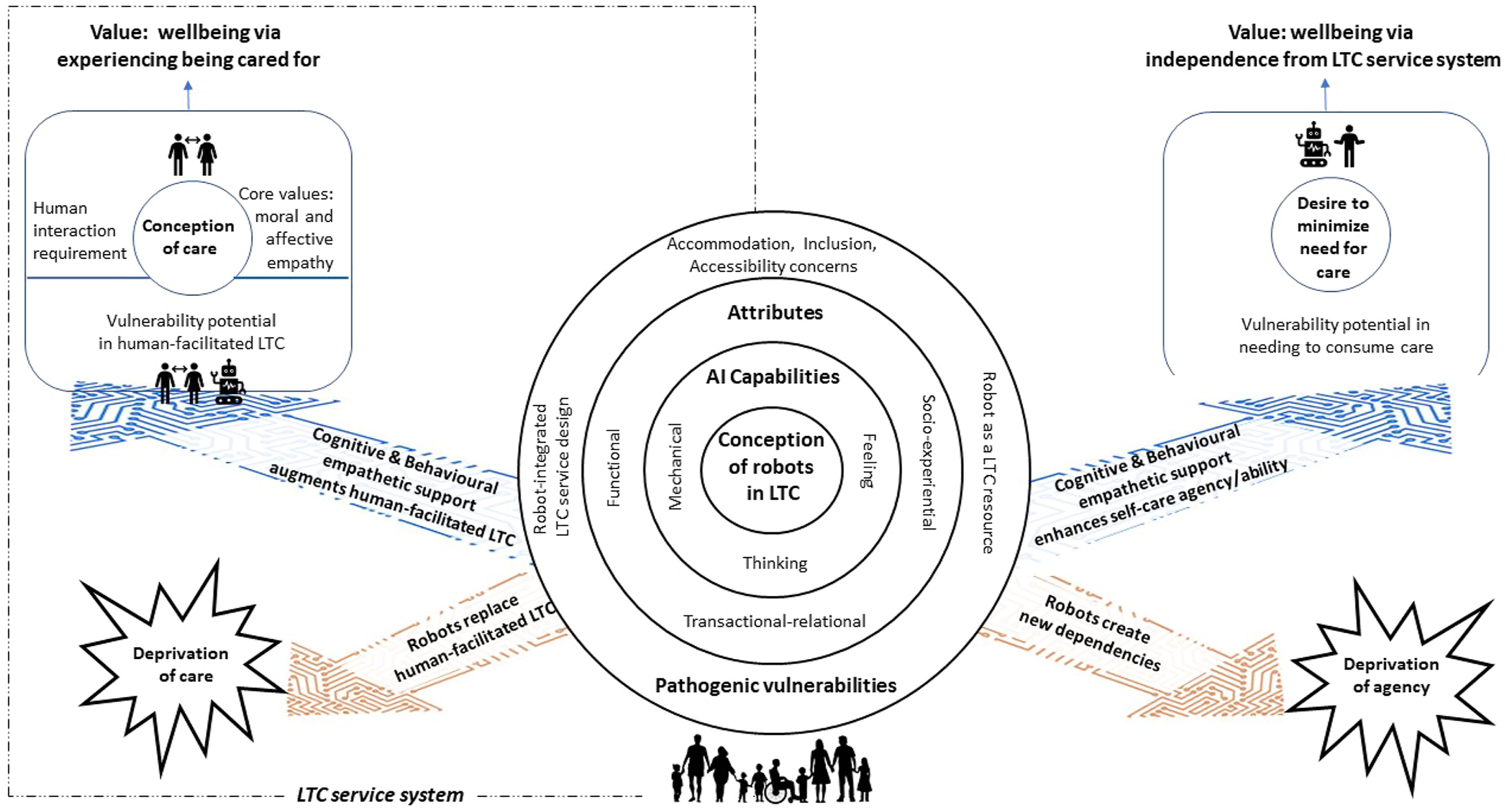
A conceptualization of consumer-conceived value of robots’ integration in LTC servicescape
Data analysis and theorization elicited participants’ conceptions of robots in LTC (depicted as concentric circles in the center of Figure 1). As we expected, conceptions of robots in LTC are comprised of articulations/first-order concepts characterizing robots’ as a potential care service resource. These articulations are related to participants conception of care (represented on the top left of Figure 1). An unexpected observation was that selected articulations 7 also characterized robots as a resource that may support consumers’ desire to minimize the need for care, depicted in the top right of Figure 1. Based on these findings, we theorized that consumers with disabilities conceive LTC service robots to offer potential for realizing value (Fisk et al. 2018), via two distinct paths (depicted as blue arrows in Figure 1) whereby robots augment human-facilitated LTC and/or enhance self-care agency/ability. Value associated with both paths is represented by wellbeing outcomes 8 that consumers envisage robots can facilitate them to achieve, by performing supportive care actions akin to expressions of cognitive and behavioral empathy (Jeffrey 2016). The wellbeing outcomes—and, consequently, value consumers desire to realize—take different forms.
The first form of value encompasses wellbeing via experiencing being-cared-for in the context of LTC service system. Although, as envisaged by consumers, robots can support humans caregivers and thus augment human-facilitated LTC, their potential is conceived to be external to the value of the care experience itself. Participants reasoned that robots, on their own, will not fully actualize care, given their inability to offer interactions where affective and moral empathy is experienced. Consistent with integrated conceptualizations of care and empathy, analysis revealed that experiencing affective and moral empathy (for which participants stipulated human interaction to be a necessary condition) is core to actualizing a “good” care experience (Jeffrey 2016; Mercer and Reynolds 2002). However, as the image conception of care in top left of Figure 1 depicts, consumers envision that robots can mitigate vulnerabilities potentially arising in human-facilitated care service contexts.
The second form of value entails wellbeing via independence from LTC service system. Here, robots’ potential is conceived as creating an opportunity to minimize, or postpone, care consumption, as the image desire to minimize the need for care in top right of Figure 1 depicts. Consumers envisage that robots can address this desire by extending their self-care abilities, thus mitigating potential vulnerabilities associated with the circumstances of requiring care.
Data also illuminated participants harboring unresolved concerns about robots in care contexts. We theorized these concerns to encompass pathogenic vulnerabilities (Lange et al. 2013) consumers conceive they might experience as a result of integrating robots into LTC servicescape. Envisaging these pathogenic vulnerabilities arising elicited participant conceptions of how robots might potentially take over from and replace human caregivers, subjecting consumers to deprivation of care as a result. Similarly, participants also envisaged robots creating new barriers and dependencies, subjecting consumers to deprivation of agency. Hence, we theorized pathogenic vulnerabilities as factors driving consumer conceptions of robots precluding, and in the extreme eroding, realization of both value forms via two alternative paths (depicted as brown arrows in Figure 1) whereby robots replace human-facilitated LTC and/or create new dependencies.
We next elaborate the derived dimensions and themes, illustrated with data extracts. 9
Conception of Care
Participant discourses concerning how they envisage care across LTC contexts (personal, social, medical) commonly resonated with the literature highlighting that experiencing care as an empathetic interaction is foundational to care recipients” conception of “good care” (Kunyk and Olson 2001; Mercer and Reynolds 2002). These considerations, captured in the theme “Core values,” align with the affective, behavioral, and moral empathy dimensions delineated by Jeffrey (2016). Participants prioritized affective and moral dimensions as pertinent to the sense of “being-cared-for”: “That act of wiping my face doesn’t necessarily mean that you care about me. It’s an act. […] that somebody is doing that so softly or gently or meaningfully, that comes across in the warmth, in the emotions of that individual” (P1); “I don’t want to simplify it by just saying good or bad care, but morality in that you know, in your heart” (P2).
Resonating with theorizations of the relational nature of care (Berry et al. 2020; Tronto 1993), the next theme encapsulates participants conceiving care as an experience that is “Only produced through human-to-human interactions” and thus something robots cannot actualize. Participants articulated that experiencing care requires a sensing of positive emotions (kindness—P4, love—P13) as part of contact with caregiver(s), something robots will not be able to offer: “…what people were saying about a robot being able to give kindness, I don’t think that’s possible. Because I think kindness stems from with inside a human being towards another human being” (P4). Participants stressed that caregiver interactions go beyond receiving care: “…having somebody just check up on me. And gives me the sense of, it’s something that a robot can’t give, that kind of, you know, social interaction, stimulation, having a conversation about something—complete—not anything to do about my care, maybe, but just having a conversation really helps my mental wellbeing, as well as my physical wellbeing” (P1).
Concurrently, the theme of “Experience of being cared for” captures that, although prioritizing the emotional aspects of care founded on affective and moral empathy characterizing human-facilitated care, participants conceived these components necessary to be integrated with well-provided care actions: “…like being able to get your meds on time, having emotional support from a partner…so, yeah, basically all these different things that need to come together in harmony to complete the big picture” (P10).
Related to these considerations is the theme “Vulnerability potential in consuming human-facilitated LTC” in which participants drew on their experiences of consuming care from current service systems to recount factors that restrict their ability to access care service and/or receive care when they require it and in a manner that aligns with core care values. These experiences are linked to awareness of stretched care service resources (“…there’s limited nurses now, isn’t there?”—P17) and of infusing care provision with positive emotions informed by affective and moral empathy being difficult, if not impossible, capabilities to impart through training: “actions can be learnt or taught but emotions can’t. And I think probably the one thing is, you need to be genuinely caring with empathy. And you can’t teach it, you either have it or you don’t” (P8). Yet, participants also reflected that emotional drivers of ‘good care’ may not necessarily ensure positive care experiences: “love […] can bring out your insecurities, it can bring out things which may be deemed toxic” (P2). Such complexities were elaborated to highlight the potential strain on relationships with caregivers stemming from pressures caregivers experience: “Even though they love you and have to care for you, it can have an impact on relationships in a bad way as well” (P13); “…there is a lot of abuse in these jobs, of being a carer, particularly, because they’re quite low paid” (P6).
The final theme in this dimension, “Vulnerability potential in needing to consume care,” reflects participants expressing that the very circumstance of accepting the need for care is fraught, reflecting the specific characteristic of care as a service offering consumers may need but do not want (Berry et al. 2020; Berry and Bendapudi 2007). P13 and P10 articulate a sense of dependency stemming from needing help: “There’s probably more help out there than I tap into […] mine is a hidden disability, and it’s that, kind of, acknowledging that […] you’re not as able-bodied as potentially somebody who hasn’t got an illness” (P13); “…what [fellow participant] said about the stubbornness, and not maybe being necessarily willing to accept that you need that help” (P10). Other participants identified the sense of dehumanization brought about by the lack of accommodation and insensitivities experienced when accessing care service, as P7 illustrates: “…someone there, just processing appointments for etc, they’re not considering that you’re in pain, they’re not considering that you can’t get up that day or you can’t walk that day or you’ve been crying because you - whatever example.”
In summary, participants firmly placed the conceived value of care, as well as the opportunities to realize this value, in the domain of human interactions. This both corroborates and extends extant conceptual assertions (e.g., Van Doorn et al. 2017; Wirtz et al. 2018) that in service involving high-level emotions, robots may not be able to sufficiently cater to consumer core needs for empathetic interactions. While prior literature suggests that such needs are harbored predominantly in relation to professional service roles (e.g., a surgeon or a divorce lawyer), our analysis highlights similar needs in relation to what Wirtz et al. (2018) term subordinate service roles (nurses and carers). As the next section shows, participants conceived robots as a resource with characteristics that potentially offer value in LTC servicescape, which appeared to be focused on mitigating vulnerabilities stemming from both consuming human-facilitated LTC and needing to consume care. Concurrently, participants conceived some of the robots’ characteristics, and how robots’ integration in LTC servicescape might be designed and implemented, as having the potential to induce pathogenic vulnerabilities.
Conception of Robots in LTC Servicescape
Aligning with the literature on robot characteristics (Simon et al. 2020; Wirtz et al. 2018), when articulating conceptions of robots in LTC, participants commonly referenced them to possess both a set of envisaged capabilities and attributes for addressing a range of their needs. To categorize these articulations, we drew on the AI capabilities framework by Huang and Rust (2021) and categorizations of service attributes in service robots (Simon et al. 2020; Wirtz et al. 2018) and wider service literature (Payne, Frow and Eggert 2017).
Overall, participant articulations reflect conceptions of LTC robots possessing advanced AI capabilities, spanning mechanical, thinking, and feeling levels of AI (Huang and Rust 2021). The “Mechanical AI capabilities” theme reflects anticipations of robots possessing a range of multi-functional capabilities for assisting with some life-management tasks to extend actualization of participants’ self-care abilities (Söderhamn et al. 2013). The range of assistance participants envisaged robots to offer encompass help with physical tasks (lifting, gripping, tying, balance support, and housework), and planning and organizing tasks: “…help me organise everything and work things out and take the mental pressure off a little bit, if that makes sense. […] that will enable me to do things that I might not necessarily have been able to do, because I was directing my energy elsewhere” (P10). Considering how robots might assist human-facilitated LTC to mitigate potential vulnerabilities, participants articulated support of medical diagnoses (“I know I’ve been misdiagnosed in the past, and they [robots] might be more efficient in terms of that”—P7) and of continuity of care provision (“…if the person doesn’t turn up […] I can still get by because I can use a robot”—P1).
The “Thinking AI capabilities” envisaged by participants similarly included capabilities that would extend actualization of self-care abilities, as P14 illustrates: “I loved everybody’s idea of this brain that learns what it is that I want to be able to see, and how I can get more independent, and I’ve got the wheels to make everything happen for me a little bit faster…”. Some of the other capability articulations aligned with Jeffrey’s (2016) delineation of cognitive and behavioral empathy dimensions. Specifically, envisaged capabilities pertained to the ability to recognize when a person might need to consume care by monitoring their physical and psychological states (vitals and anxiety levels) and to offer and arrange for situationally required care (communicating warnings to the consumer or; alerting emergency care services when required). Finally, participants expected a LTC robot to possess capabilities to adapt multiple mechanical functions to their changing internal and external circumstances: “…actually, people’s needs are complex […] You don’t always need the same thing all the time, and conditions change” (P10). The combination of personalized learning and analytic processing was expected to mitigate vulnerabilities stemming from human biases, and thus the potential for decision-making errors. For example, P7 extrapolated from their experience of misdiagnosis to suggest that robots “would not have any background of like disease or disease in their families […] and any sort of personal emotions that are attached to care,” enabling them to rationalize the need for care in difficult situations (e.g., when considering withdrawing medical care). Participants stressed that their expectations of robots’ intuitive capabilities characterizing thinking AI included the ability to recognize where their service represents an unwanted intrusion and be “whipped back in its box” (P11).
The “Feeling AI capabilities” theme reflects participant envisaging that robots would perform tasks associated with Feeling AI, and might influence how they themselves felt, but that did not necessarily actualize the care experience. Participants reasoned that robots might perform acts of compassion that could evoke a sense of companionship. While extant conceptualizations consider these capabilities to be perceived as surface-acted emotions (Wirtz et al. 2018), participant characterizations suggested greater alignment with the behavioral empathy that encompasses acting and communicating in helpful ways (Jeffrey 2016). P1 illustrates: “So it’s just that kind of, you know, those small things that just add that extra value […] not a companionship with a robot, but it’s just a helping hand. […] And, maybe, partly, it is lip service, but secondly it’s more actions as well, isn’t it? ‘Is that okay?’ ‘Yes, thank you’ or ‘no, it’s not’. And then you’ve got that interaction with the robot that actually shows its compassion.” While envisaging robots to possess capabilities to enact behavioral empathy, participants stressed they recognize that robots cannot care. They articulated affective empathy and its expressions associated with care, such as warmth, humor, non-verbal signals (touch, listening, and smiling), to lie beyond robots’ capabilities. P3 summed up “…it’s the emotional attachment that you have with a human that you would necessarily have with the AI.”
In summary, it appears that participants envisage robots to be able to at least exhibit cognitive empathy (know what will make a person feel better) and behavioral empathy (perform helpful and therapeutic acts). However, they recognize that robots cannot experience and project affective empathy (be compelled to act on the basis of strong emotional responses) and moral empathy (genuine compassion), two aspects necessary for actualizing an authentic experience of “being cared for.” Hence, feeling AI capabilities do not appear to be linked to how consumers envisage care. Concurrently, across mechanical and thinking AI levels, participants envisaged robot capabilities to potentially contribute to their wellbeing in two distinct ways: 1) minimizing or postponing the need for LTC service by extending actualization of their self-care (and thus mitigating vulnerabilities stemming from the need to consume care) and 2) supporting and enhancing the effectiveness of human-facilitated LTC (and thus mitigating vulnerabilities that might occur in the current LTC service).
Participants’ characterizations of LTC robots also reflected them envisaging robots addressing a variety of service needs. We distill these conceptions in three themes reflecting attributes of an envisaged service offering by a robot: functional, socio-experiential, and transactional-relational adaptability. “Functional attributes” theme encompasses categorizations conceptualized by prior service literature (Čaić et al. 2019), including ease of use, reliability, and strength. Participants also listed other functional attributes, such as mobility across spaces, multi-sensory response to environmental conditions (e.g., seeing fire and smelling smoke to determine danger), and environmentally friendly design/performance.
When distilling the “Socio-experiential attributes” theme, we were guided by participants’ articulations that robots cannot be capable of offering emotional expressions of care. Hence, we adapted the socio-emotional attributes categorization by prior literature (Wirtz et al. 2018) to reflect participants’ conceptions. Concerning the social attributes component, participants expected robots’ appearance to take non-threatening and non-humanoid, yet relatable, forms. These expectations were linked to the degree of social presence participants would deem acceptable, supporting theoretically derived considerations in this vein (van Doorn et al. 2017). For example, P7 discussed how curved lines would be perceived as “softer” and “less imposing,” while P2 stressed that the appearance should distinguish the robot as “…first and foremost, a robotronic thing,” but it could feature “limbs and it kind of has a voice.”
Participants also outlined several hedonic experiences LTC robots could offer, including enjoyment (fun) and enrichment of experiences compared to those provided by current technology. Further, participants reiterated their expectation that robots will minimize or prolong them having to need to consume LTC services, thus mitigating the potential vulnerability associated with such circumstances. Central to conceptions of this attribute was the expectation of enhanced independence and extended actualization of self-care, as P1 articulates: “I don’t want to be reliant on another human being, I don’t want people to take pity on me as a disabled person. I don’t want people to, you know, feel that they have to come and visit me because I’m disabled or that I’m actually a burden to someone else. So I am fiercely independent in that respect. So I think if a robot was there to help me, I would be less reliant on others - do you see what I mean?”. Resonating with cautions of potential failed outcomes in care actualization (Sharkey and Sharkey 2012), participants stressed that it is vital that robots mitigate (rather than reconstitute) potential dependencies on care providers. This is exemplified by P11: “I don’t want to hand over responsibility any more than I need to. […] I don’t want it [robot] to become something I physically rely on in any sense, if it’s at all possible. […] that again comes back to retaining your independence….”
The “Transactional-relational adaptability” theme represents the significant participant variation in envisaged relational experiences in LTC robot interactions. As such, these conceptions encompassed a continuum between functional transactions and a symbolic human-like relationship. P11 illustrated the transactional end of the continuum: “I don’t want a relationship with AI; I want a relationship with people, and this is the functionality, and what it would give me in terms of freedom.” Others envisaged interactions with a robot taking a form beyond a transaction with a piece of equipment, albeit different to human relationships, marking the continuum’s midpoint: “I wouldn’t want it to be kind of like my best friend […] it wouldn’t […] be providing me with the sort of relationships that I would usually get from a human, but I think, yeah, it doesn’t have to just be like a machine” (P10). The relational end of the continuum reflects the following views: “I actually believe there is a relationship with my robot […] It is like a person to me. I would spend a lot of time with it […] and I want to be happy with it” (P14). The observed varying nature of relational expectations underscores the centrality of the requirement to robots to adapt and cater for the diversity of individuals’ needs and to empower consumer choice. P11 articulates this demand: “Absolutely, not force it upon people or one size fits all […] as long as you have the choice in that situation, that matters.”
Finally, three themes encapsulate factors considered by participants to have the potential to create pathogenic vulnerabilities. The theme termed “Pathogenic vulnerability potential from robot as a resource” corroborates conceptually identified concerns (Williams et al. 2020) over decision-making logics that may be built into AI algorithms: “I would like to be able to sit down and discuss it with medical professionals, and not just be told that somebody had pulled the plug because a robot had worked out an algorithm that said that’s the best thing to do” (P8). Other participants doubted robots being sufficiently advanced to respond to complex changing circumstances and emergencies: “it [robot] might be set up by somebody else and then just perform a programme of actions. But that programme of actions might not be what I need that day and I might not have the capability or capacity to be able to actually change that programme of actions. […] It also could be dangerous because it could make that person a cup of tea, but I might have Parkinson’s […] or shake that day and end up spilling it all over me. […] And then there isn’t that first aid care either. […] a robot may not be able to do that” (P1). Participants were also concerned about robots performing unwanted actions beyond care tasks, such as pushing information. P5 drew on prior consumption experiences to illustrate technology features inducing these concerns: “… things like Amazon that tries to sell me things that I’ve just bought. Recommendations for things that I might like, which are always wrong.”
The theme “Pathogenic vulnerability potential within robot-integrated LTC service design” reflects concerns over losing human contact and retaining control, aligning with the nascent evidence from information technology and human–robot interaction studies (Deutsch et al. 2019; Sharkey and Sharkey 2012). The concerns over robots replacing human-facilitated LTC related to both caregivers and recipients. P2 expressed a concern that carers might lose their livelihoods: “you don’t have to go to this huge hurdle of trying to recruit so many ‘x’, the people that used to work in the NHS, where you could just use robots”; P8 reflected that the prospect of human carer replacement by robot “can make a difference between somebody getting better and not.” These concerns informed concerns over losing control in consuming LTC services, as P2 illustrates: “…it’s a little bit too kind of Minority Report where it’s like, if they know exactly what you’re going to do before you do it, it’s a bit like you, yourself, don’t have any control.”
Finally, the theme “Accommodation, accessibility and inclusion concerns” captures participants’ strong desire for the AI innovations developed for them as intended consumers to be co-created with them. These expectations go beyond personalization: “…not so much personalization, more on the input into the design” (P11). Rather, these expectations were driven by a concern for the design of LTC robots to accommodate for the diversity of needs: “if every step of the way through the robotics process, you could have normal people, normal users maybe testing it out, testing if it works for them, and different disabilities” (P9). Participants specified concerns about the financial and cultural accessibility of robotic solutions in LTC servicescape. P13 articulated that “it [robot] should be accessible to all, no matter any demographic, age, […] background, […] affluence”; P12 observed that a fellow participant expressed concerns over cultural accessibility: "[fellow participant: I will just say that we have a lot of problems here with Alexa and things like that, because it doesn’t understand our accent.] When you say understands various accents, therefore I assume you’re going to make it for all the languages in the world? […] Yeah, if it’s equality and diversity”. Specific emphasis on articulating these concerns reflects the “nothing about us without us” maxim promoted by the disability movement (Frantis 2005). It also aligns with Fisk et al.’s (2018) theoretically derived principle of fairness embedded in inclusive service design.
Discussion and Implications
Intelligent service robots have the potential to transform LTC and to support resolution of the “crisis of LTC” (International Labor Organization, 2018; Osterland 2021). Yet, it is imperative that the urgency to alleviate this crisis does not overshadow the priority of (re)designing socially just services (Field et al. 2021; Fisk et al. 2018; Huang et al. 2021). The present study sought to explore how consumers with disabilities conceive the potential value of robots in LTC, and the vulnerability-inducing factors that might restrict their opportunities to realize value. Together, these conceptions ultimately inform consumers’ willingness to accept LTC robots’ integration. Employing an interdisciplinary approach, we based our exploration on the premise that the development of service concepts—the first level of service design for inclusion—should foreground the perspectives of people experiencing, or possessing a heightened propensity to experience, consumer vulnerability and consider the impacts of integrating robotic technologies holistically (Fisk et al. 2018). The conceptualization of consumer-conceived value of robots’ integration in LTC servicescape (Figure 1) drawn from our findings offers contributions with important implications for theory and practice.
Implications for Theory
The paper makes three theoretical contributions. First, our conceptualization of the consumer-conceived value of robots’ integration in LTC servicescape (Figure 1) contributes to literature concerned with value-centered care service (re)design (Agarwal et al. 2020; Anderson et al. 2018; Berry et al. 2020). By examining how consumers’ conceptions of robots in LTC relate to conceptions of the care experience itself, our conceptualization illuminates a fundamental vision of robots in LTC held by consumers: while robots are able to provide some LTC services, they lack the innate ability to care in the way a human being might. Having elicited that, in consumers’ minds, robots cannot fully actualize care experience; we identify two value realization paths that consumers associate with robots integration in LTC: 1) augmentation of human-facilitated LTC and 2) extension of self-care actualization.
Second, our conceptualization contributes to the transformative service research drive for identifying routes to enhancing the wellbeing of consumers experiencing vulnerabilities, and to the service robots literature that examines the value creation/destruction potential of robots’ integration in these consumers’ lives (Čaić et al. 2019; Henkel et al. 2020; Huang et al. 2021). By focusing on consumers with disabilities—a marginalized population with heightened propensity to experience vulnerability (Higgins 2020)—we underscore the importance of considering whether and how aspects of service concepts, systems, and interactions might generate consumer vulnerability. We take a service inclusion lens (Fisk et al. 2018) and draw on the concept of pathogenic vulnerability (Lange et al. 2013). By doing so, we illuminate that service (re)design in LTC should consider whether the integration of robots will address both currently experienced vulnerabilities and new vulnerabilities that might perversely arise from (re)design efforts. Consumer-centric perspectives are central here, since marginalized groups (like consumers with disabilities) lack power in the marketplace (Higgins 2020). Hence, pathogenic vulnerabilities can be overlooked without explicit focus on consumers’ voice.
Our conceptualization connects consumer-conceived pathogenic vulnerabilities from robots’ integration into LTC servicescape to two potentially value-destroying paths. The co-existence of these paths alongside value-realizing paths envisaged by consumers with disabilities corroborates earlier findings on elderly consumers (e.g., Čaić et al. 2018). We identify that pathogenic vulnerabilities facilitate these paths’ conception, offering an explanation for consumer reticence toward accepting LTC service robots, as observed in the current findings and prior studies (Wang et al. 2017; Wachsmuth 2018). The unresolved ambiguities concerning the design of robots’ characteristics and the intended manner of their integration in LTC service systems appear to drive consumers to envisage robots’ potential to erode value they desire to realize. Specifically, uncertainties regarding robots potentially possessing characteristics that preclude consumers’ exercising full control over LTC service actions performed by robots and concerns about fair access, accommodation and inclusion of consumers’ perspectives as end users of LTC robots drive concerns over being potentially deprived of agency. Similarly, uncertainties around the intended manner of robot integration in LTC service systems, coupled with the placement of care experience actualization in the domain of human interactions, translate into concerns about being potentially deprived of care. Partly, these concerns may stem from ambiguous policy and consultancy discourses 10 regarding robots’ integration in LTC servicescapes that utilize such terminology as “(social) care robots” and “AI-enabled (health)care.” While these terms do not directly suggest assigning robots with primary role in care decision-making or robots replacing human-delivered care, they could be interpreted this way. By spotlighting how robots’ integration into LTC can be conceived to erode value in care, our conceptualization stresses the necessity to examine (existing or pathogenic) vulnerability-inducing factors when designing LTC service concepts.
Finally, we provide empirical support for, and theoretical extension of, prior categorizations of AI capabilities and attributes (in the broad service domain; e.g., Huang and Rust 2021; van Doorn et al. 2017; Wirtz et al. 2018) within the emotion-intense servicescape of LTC. Our findings show that, for the potential value from robots’ integration in LTC conceived by consumers to be realized, consumers require robots to be equipped with the most advanced forms of AI capabilities distinguished by prior conceptualizations (Huang and Rust 2021; Čaić et al. 2019). These include mechanical (e.g., lifting or housework), thinking (e.g., monitoring physical or psychological states), and feeling AI capabilities that allow a robot to enact helpful and therapeutic behaviors (e.g., interactions). However, there are currently few market-ready LTC robots equipped with the kind of thinking and/or feeling capabilities that consumers expect them to possess; which may explain the limited adoption/assimilation of robots with lower-level mechanical intelligence, such as Nao, Pepper (Kyrarini et al. 2021), and Zora (Tuisku et al. 2019). Extending previous work that suggests consumer expectations of AI capabilities mirror a progression from standardized to personalized service attributes’ expectations (Čaić et al. 2019; Huang and Rust 2021), we show that consumers expect and require the freedom to choose which robots' characteristics to utilize. That is, consumers conceive robots’ characteristics to be adaptable to an individual’s need for social presence and for the relationalization of interactions (van Doorn et al. 2017; Wirtz et al. 2018). Thus, consistent with the “offering choice” pillar of service inclusion (Fisk et al. 2018), the design of service offerings deploying even the most advanced AI/robots should incorporate adaptability attributes to avoid harming and alienating consumers by restricting choice.
We also offer a theoretically grounded and empirically supported clarification of types of empathy that consumers conceive to be within the AI capability. Previous conceptualizations (Huang and Rust 2021) attribute AI with empathetic capabilities, linked predominantly to feeling AI capabilities for expressing emotions. We show that consumer conceptions of robots’ empathy extend across thinking and feeling AI capabilities, although the nature of empathy is restricted to cognitive and behavioral dimensions and does not extend to affective and moral empathy (Jeffrey 2016). This suggests that human augmentation, where robots provide action-oriented (rather than emotional) support, is requisite for emotion-intense services such as LTC. Similarly, with regard to robots’ role as a service resource extending consumers’ self-care capacity, robots’ empathy capabilities appear insufficient for providing emotional support akin to “a human conversational partner” (Huang and Rust 2021, p. 33). Robots are conceived capable to support consumers in regulating negative emotions evoked by circumstances of needing care; consumers envisage utilizing robots for maintaining/enhancing independence and, consequently, ability to realize hedonic experiences (fun) not associated with care.
Implications for Managers and Policy Makers
Our conceptualization of the consumer-conceived value of robots’ integration in LTC servicescape has practical applications. It can be utilized by LTC providers (managers and caregivers) to consider the impacts of deploying robots on care recipients when designing service systems and determining the purposes and the extent of recipient-robot interactions. For emotion-intense services, such as care, the potential to experience vulnerability is acute (Longoni et al. 2019). Hence, it is valuable for providers to examine whether care recipients’ concern that their needs will not be fully considered may mitigate robots’ adoption.
Our conceptualization can also facilitate structured considerations of ethical implications of decisions concerning the precise mode of service robots’ deployment in practice (Borenstein & Pearson, 2014). Historic biases toward care professionals’ perspectives in the design and management of LTC service has served to disempower consumers by limiting their ability to influence how care is provided (Batavia 2002). Recent literature (e.g., Williams et al. 2020) cautions that, unless the perspectives of historically overlooked consumers are fully understood, frameworks for deploying AI risk replicating, if not magnifying, longstanding social injustices. Our findings evidence such anxieties amongst consumers with disabilities.
As the deployment and use of LTC robots become more widespread, we recommend that managers, designers, manufacturers, and care providers adopt the following principles: 1) Begin with a consumer-centric service inclusion perspective when developing and designing LTC robots and strategies for their integration in LTC service. While this paper focused on the development of inclusive service concepts, service inclusion lens should be also applied to system architecture/navigation and processes for service interactions; 2) Prioritize adaptable designs when developing robotics for care. Our study shows that there is not a one size fits all solution to providing care consumers with opportunities for realizing value and enhancing their wellbeing. Designs therefore should provide flexibility for consumers to “tune” robots to preferences for specific features and resources; 3) Work with policy makers to address the financial and cultural accessibility of robots. Economies of scale are likely to reduce costs and offer solutions to providers for designing and delivering fair service.
The insights discussed above are also important from a policy perspective, given the substantial investment into care robotics’ development. Clarifying the robots’ role (e.g., care assistant rather than robotic carer) could mitigate consumers’ reticence toward robots in LTC. We stress that we are not recommending a superficial labeling change. Policy makers should seek widespread consumer input to inform (re)design of robot-integrated service systems. This will require policies encouraging interdisciplinary collaborations, including theoretical and practical insights from service and consumer researchers. Policies can also require manufacturers and service providers to avoid suggesting that LTC robots are equivalent to human caregivers in promotion messages. Finally, policies can encourage transformative service initiatives (Anderson and Ostrom 2015), given their social justice and wellbeing foci.
Limitations and Areas for Further Research
Our study has several limitations, warranting further research. While our design followed qualitative research criteria for rigor (Gioia et al. 2013) and reliability and validity (Noble and Smith 2015), we acknowledge that small sample sizes, as in our study, might limit representational generalization. However, small samples afford analytical generalization in that they provide in-depth contextualized insights and account for the unique experiences in deriving theoretical explanations (Halkier 2011). This is particularly valuable when prior knowledge on the area focal to the inquiry and a given population are scarce, as is the case with our study (Crouch and McKenzie 2006).
Due to Covid-19 restrictions, data collection was undertaken online, necessitating adaptation of methodologies and creating new challenges (i.e., unfamiliar technology and broadband (in)stability). A positive unanticipated consequence was that we were able to draw on a nation-wide (United Kingdom) population since people were able participate without the burden of travel. The pandemic has also caused people with disabilities and their caregivers to experience a loss of emotional safety (Berry et al. 2020) and created unforeseen opportunities for service robots to improve consumer wellbeing beyond the pandemic (Henkel et al. 2020). Our study did not address these opportunities, which require further attention. Because the study was conducted in the health-social care context of the United Kingdom and included only people with physical disabilities, research in other countries and consumer contexts is needed. As technologies and robots with higher levels of intelligence are developed and enter the market, longitudinal studies can examine potential changes in consumer views over time.
While the service inclusion paradigm (Fisk et al. 2018) provided our exploratory study with a broad theoretical focus, development of a comprehensive framework for LTC service design that holistically integrates service concept, systems’ architecture and interactions’ processes across service inclusion pillars (Fisk et al. 2018) was beyond the scope of our study. Nevertheless, the emergence of two parallel types of paths representing consumer conceptions of the implications of robots’ integration into LTC indicates directions for extended applications of service inclusion in future service robots research. The two types of paths in our conceptualization highlight that—paradoxically—consumer conceptions of robots’ integration into LTC servicescape reflect the envisaged potential for i) enhancing value realization opportunities, aligning with “enabling opportunities” and ii) possible suffering should robots deprive consumers of care and agency, misaligning with “relieving suffering” service inclusion pillars (Fisk et al. 2018). Future research could examine approaches to resolving this paradox. Consumer conceptions of high-level, yet adaptable AI capabilities, when envisaging a LTC robot underscores the importance of aligning service robots research efforts with the “offering choice” service inclusion pillar (Fisk et al. 2018).
Seeking to address a lack of consumer-centric research, we focused on value-centered care (Agarwal et al. 2020) and explored the conceptions of end users (consumers) of LTC. Additional research could expand the scope to other servicescape actors, thus engaging the voices of carers, families, service providers, robotic designers, and manufacturers (Anderson et al. 2018). This would enable a more holistic comprehension of the role that robots may play in co-creating and co-destroying value over entire care networks (Čaić et al. 2018).
Thoughts on the Future of Consumer-Based AI-Integrated LTC: Will Robots Ever Care?
Perhaps the most important outcome of our study is that it identifies that consumers conceive the value of LTC robots to lie in the domain of performing support/assistance for self-care and care facilitated by other humans, but not the provision of care itself. The conceptualization thus supports theoretically derived propositions that in emotionally intense service contexts, robot service agents constitute a useful complement, and not a substitute, for human agents (Xiao and Kumar, 2021). Our participants were acutely aware that robots cannot biologically experience and thus cannot exhibit the affective and moral empathy necessary for actualizing the care experience. Hence, at least for the foreseeable future, care remains a prerogative of humans, since “robots do not replace a nurse with a beating heart” (Tuisku et al. 2019, p. 47). That said, robots’ inability to care can potentially “de-emotionalize” some aspects of care which evoke negative emotions through, for instance, inadequate care actions. As we show, the prospect of maximizing independence from human-facilitated care constitutes an important value-adding characteristic of robot service. Whether robots will ever be able to actualize care like humans do is a question for the distant future. The answer appears to lie with discerning how robots can express affective and moral empathy—a key topic for future service robots research.
Supplemental Material
Supplemental Material - Service Robots in Long-Term Care: A Consumer-Centric View
Supplemental Material for Service Robots in Long-Term Care: A Consumer-Centric View by Eva Kipnis, Fraser McLeay, Anthony Grimes, Stevienna de Saille and Stephen Potter in Journal of Service Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper originates as a result of work on a project titled “Improving Inclusivity in Robotics Design” which received funding from “Research England, via The University of Sheffield’s Higher Education Innovation Fund (HEIF)" and in-kind funding from IBM. Data collection was supported by facilitators certified in methodologies utilized in the studies reported in this paper, as follows: Kate Halliwell (Community Philosophy), Richard Gold (LEGO® Serious Play®), and Mica Whitby and William Hawken (Design Thinking, IBM). The authors would also like to express their thanks to the participants of the research presented in this paper for sharing their insights.
Supplemental material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.