
Abstract
A 54-year-old male entered a deep cave for recreational purposes. Near the bottom of the 324-meter-deep cave, he slipped and sustained an open femur fracture and a head injury. His companions stabilized him with direct pressure for bleeding control and improvised splinting and then summoned help. Medical personnel found the patient hypotensive with an altered mental status. Arriving rescuers further stabilized him, packaged him in a litter, and then transported him. While waiting for a technical rope to raise him up a 179-meter pit, he was transfused 1 unit of blood. Twenty-one hours after his injury, he exited the cave and was transported by helicopter to a trauma center. He made a full recovery.
Introduction
Trauma can happen in many wilderness settings. Hemorrhage is the leading cause of early death after trauma. 1 If rapid evacuation is an option, decisions about fluid and blood can be made in an emergency department. In cases where immediate transport is not an option, these decisions must be made in the field or through a medical control if communication is available. Field transfusion saved lives in combat situations in Afghanistan but was less important as transport times decreased.2,3 Intravenous fluids can supply needed pressure support but in traumatic cases can also risk worsening blood loss and thus oxygen-carrying capacity. Civilian transfusion from helicopter services is becoming more common; however, they are mostly administered with short “on-scene” times rather than in a deep wilderness setting.4,5 We report on a case in which blood was transfused more than 300 meters deep in a cave.
Case
A 54-year-old white male entered Ellison’s Cave in rural northwestern Georgia with 3 companions in May 2013.6,7 Ellison’s is known for having the 2 deepest underground free-hanging drops in the contiguous United States—Incredible Pit at 134 meters and Fantastic Pit at 179 meters. The total cave is 19.5 km long and 324 meters deep. The cave is popular due to its long, free-hanging drops, which allow for lengthy rappels and climbs out. The party intended to descend to the bottom via Incredible Pit, cross under the mountain, and then exit by way of Fantastic Pit, which had been rigged by another party. This party would then use the Incredible rigging to exit in a crossover trip, as shown in Figure 1.
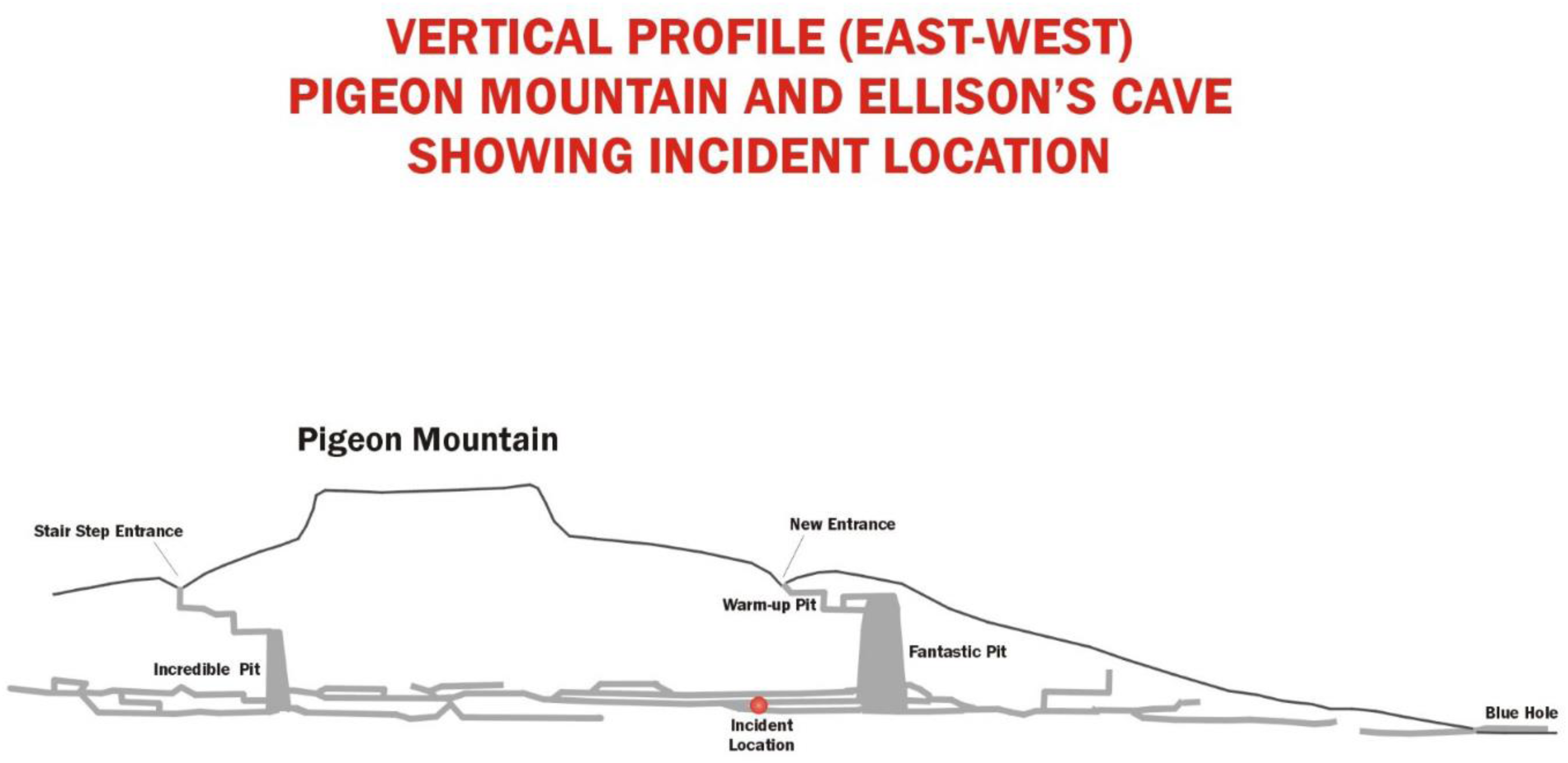
Vertical Profile of Ellison's Cave.
After successfully rappelling Incredible Pit, the party went through several crawls and rooms before the subject slipped and fell down a 12 m slope, then into an 8 m pit. 7 He did not respond when called. Companions went down to assess. He was not conscious and had an obvious deformity of his left thigh with an open wound and copious blood. They applied pressure with an improvised dressing and splinted the leg with a brake bar rack and 1-inch tubular webbing. They then got him into a garbage bag for hypothermia prevention, kept him as comfortable as possible, and sent for help, sending one party member climbing up the 179 meters of free-hanging rope in Fantastic Pit. 7
The emergency response started with the local cave and cliff rescue team, followed by the near-immediate activation of other teams from Tennessee, Alabama, and Georgia. Two paramedics hiked up the mountain, traversed the upper passages, and then rappelled down Fantastic Pit with their gear and crawled through boulders to access the patient. They found him altered, with a GCS of 13 and an improvised dressing covering a large laceration, causing them to attribute his altered state to head trauma. There was copious blood on the ground, but no more active external bleeding by then. He was tachycardic, hypotensive on measurement, and had narrow pulse pressures. The patient was further treated with a liter of saline as part of initial trauma stabilization, 1 g of intravenous (IV) ceftriaxone for his compound fracture, 4 mg of IV ondansetron to prevent vomiting during evacuation, and 50 mcg of IV fentanyl for pain. The saline had entered the cave, warmed, and was kept inside a cave suit during transit, but was no longer at body temperature. Initially unconscious right after his fall, he was conscious and combative when paramedics arrived. The paramedics sedated with 1 mg IV lorazepam to allow for packaging, personal safety, and evacuation. Having observed the extent of blood loss and knowing the patient's clinical condition, poor vital signs, and the long time required for evacuation, rescuers requested extra equipment and O-negative packed red blood cells (PRBCs) for transfusion. They packaged the patient in a litter with insulation and a vapor barrier. Once stabilized and packaged, the team evacuated the patient to the base of Fantastic Pit.
Cell phones, satellite phones, and, to a large extent, radios are ineffective underground. Communication from incident command was established with wired field phones to the top of Fantastic Pit, radio contact at the bottom, and another set of wired field phones to the patient. This communication system enabled contact with medical control and allowed for the request of specialized medical gear, such as a traction splint and blood.
The unit of PRBCs was delivered by helicopter from the local trauma center to a landing zone near the cave, then taken by off-road vehicle to the entrance, where it was given to a caver known to be able to move quickly underground. Other teams working underground were given directives to prioritize his movement. Once the blood arrived at the base of Fantastic Pit, the single unit was given via a commercial, battery-powered blood warmer while the rigging team finished preparation for the haul up the pit. The patient was ready to move by the time the first unit was infused. A second unit on site was not used so as not to delay transport.
He was raised the 179 meters by a rappelling counterweight haul system in 25 min. After one more raise up a 38 meter drop, he left the cave and was transported 30 miles by helicopter to the local trauma center, 21 h after his accident (see Figure 2). The rescue used 106 persons, of whom 71 went underground.
Rescue Timeline.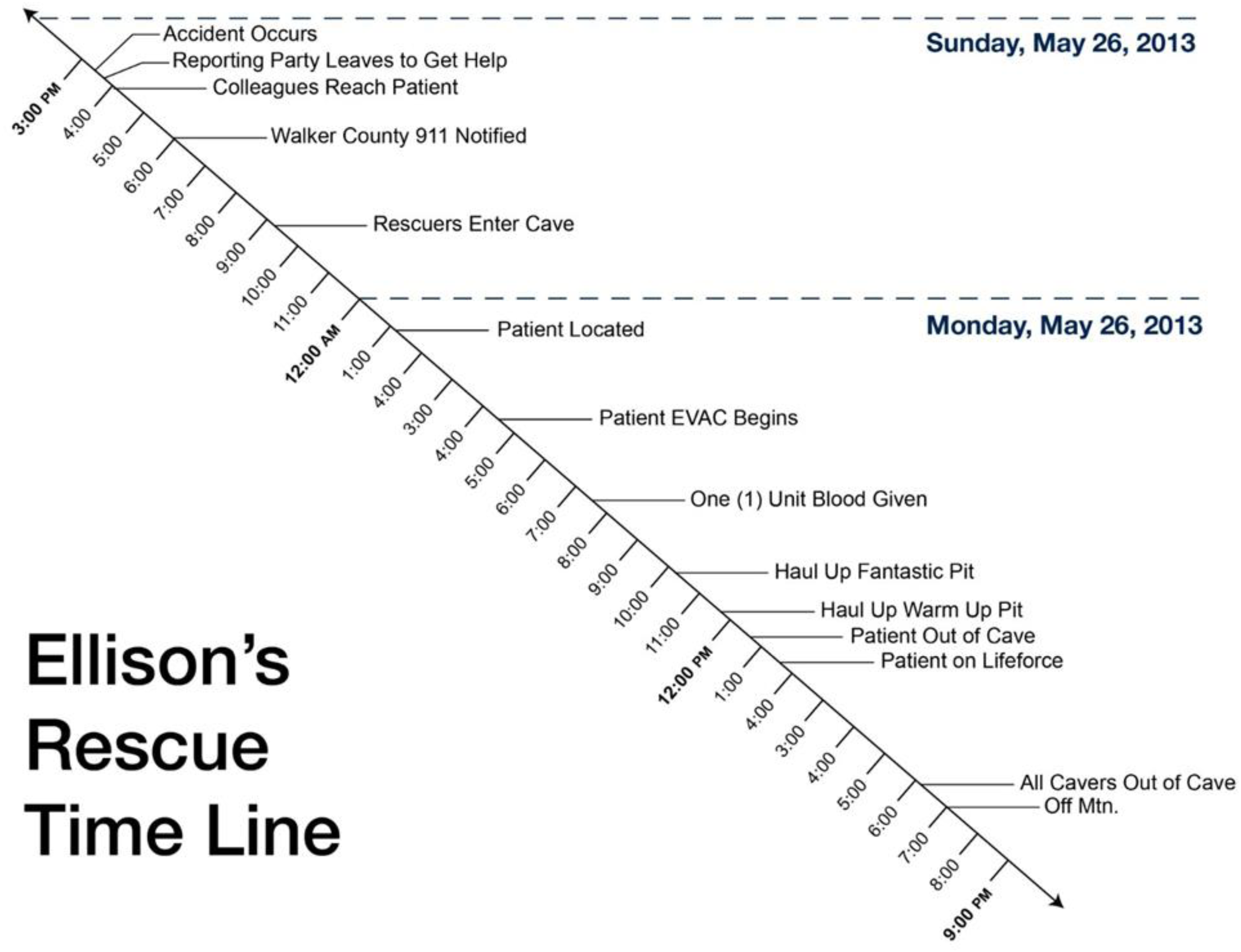
At the hospital, he was found to have a frontal skull fracture with subarachnoid hemorrhage and pneumocephalus, besides his femur fracture. After treatment and rehabilitation, he made a full recovery.
Discussion
Only under specific conditions is field transfusion both feasible and appropriate. In almost any situation, immediate evacuation is more appropriate than waiting for blood to arrive. In this case, the time required for rigging a complex rope rescue made the choice reasonable. An obstacle to transfusing at blood storage temperature is the concern of worsening hypothermia and risk of coagulopathy in traumatized patients in wilderness environments. 8 Body heat is ineffective at warming fluids to body temperature. 9 Fortunately, a number of field heating methods have been found to be effective for intravenous fluid, which could be used to warm blood.10,11 Warmed blood temperature should be kept to ≤42° C to avoid hemolysis.12,13 Much like the case of acute trauma in a trauma center, standard cross-matching will not be possible in field conditions. Type O blood will be preferred, though low-titer O+ blood can be considered depending on availability.14,15 Consideration of risk versus benefits and consent for transfusion will require discussion of the higher risk of transfusion reaction.
At the time of this incident, field transfusion was rare. The military’s 7th edition of Prehospital Trauma Life Support (PHTLS; 2011) suggested that field use of “blood is impractical for use in the prehospital setting.” 16 Based on the military experience of early transfusion, it has become more common, with 34% of trauma center–associated EMS agencies carrying blood into the field in 2015.2,17 By 2023, PHTLS not only allows for blood use but states it is a minimum capability for prolonged field care.18,19
Whole blood was once the transfusion of choice. 20 As needs for separate components grew, PRBCs became more common. With time, military and civilian experience showed that whole blood transfusion was superior to component therapy.21,22 By 2021, the United States armed services made low-titer group O whole blood the resuscitation product of choice in battlefield situations, and the AABB (formerly known as American Association of Blood Banks) recommended it for prehospital care.15,23 PHTLS also makes it the blood product of choice. 19
In this case, the patient received PRBCs. Whole blood was not available at the time. An immobile patient in a cold or even cool environment is at risk for hypothermia, which complicates the care for any trauma patient suffering from the lethal triad of hypothermia, coagulopathy, and acidosis, potentially unified by hypocalcemia.8,24 In this setting, warmed whole blood may be the transfusion of choice for both blood loss and hemorrhage control, if available. 25 The patient received a liter of normal saline. Advanced Trauma Life Support advocates for a liter of balanced IV fluid during a trauma resuscitation; however, there are data to support a policy of permissive hypotension until definitive hemorrhage control has been achieved to avoid further hypothermia, coagulopathy, and blood loss.26,27
Hypocalcemia is a predictor of mortality in trauma settings. 28 Transfusion of citrated blood products may lower calcium even more. 29 While data are lacking that supplementation makes a difference, new military Joint Trauma System guidelines now recommend calcium supplementation after the first unit of citrated blood product. 29
There are significant logistical obstacles to transfusion. Red cells can remain in storage more than a month if kept at 1°–6° C. 30 Transport should be at 1°–10° C in containers validated to maintain temperature. 30 Once warmed, they must be transfused within 4 h. 13 In this case, the blood was maintained in its cooler and transported by helicopter, then by a person dedicated to carrying this one item underground directly to the patient. In a colder cave, there would be more margin for transport, but less so in Ellison's at 13° C. 31 Sticking to these guidelines would not have been possible in a more complex cave without direct pathways to the patient. This was successful because of preplanning between local emergency services and the search and rescue team in the field. The paramedic on site giving blood had training and protocols allowing for blood transfusion and was under the medical control of a physician working at a trauma center with a blood bank. This allowed them to tap into resources not usually present for a response deep in an austere environment.
This case illustrates the value of training in wilderness medicine improvisation techniques. Without bleeding control and fracture stabilization done by party members, he had a high chance of dying on site. They acted early to prevent hypothermia by isolating from conductive and convective heat loss with insulation and a trash bag that they had brought with them for just this purpose. 8 In an austere environment, it may only be party members who can intervene during the golden hour of trauma. Wilderness rescues, and especially cave rescues, can have extended response and extrication times. These early interventions have the chance to be the most important.
This demonstrates the conflict in wilderness care and front county emergency medical care over whether to prioritize movement as definitive care versus stabilization in the field. In this case, a natural pause in transport was an opportunity for further intervention. If immediate evacuation had been possible, it is less clear that transfusion would be beneficial.3,15 There was a second unit of packed cells on site, but no time to give it without delaying evacuation. Balancing stabilization for prolonged transport versus expeditious movement is challenging.
It has been reported in English translations that blood transfusion was done underground after an accident during the initial exploration of the Gouffre-Pierre-St Martin in the Pyrenees of France in 1952. 32 Closer examination of descriptions of the event by those who were there shows no evidence of blood being transfused but rather a clear infusion of liquid, likely saline. 33 We believe that this transfusion, done in Georgia, is the first one done in a cave.
This case study demonstrates that, although technically challenging, blood transfusion is feasible in remote environments, even deep within a cave. Battlefield and civilian experiences have demonstrated the benefits of field transfusion, making it a more common practice. More helicopters and ambulances now carry blood products.4,5,15,34,35 Storage requirements for blood remain complex. Once above 10° C, blood must be transfused or disposed. 13 Communication is required to coordinate transfusion logistics, especially in austere environments. Given potential delays in extrication with blood delivery, though, further work is needed to determine indications. Transfusion should not delay timely evacuation.
Footnotes
Acknowledgments
Buddy Lane, Allen Padgett, and Bruce Smith.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.