
Abstract
Introduction
Helicopter search and rescue (SAR) in Africa is conducted primarily by military organizations. Since 2002, the Western Cape of South Africa has had a dedicated contracted civilian helicopter emergency medical service (HEMS) conducting air ambulance, terrestrial, and aquatic rescue. To our knowledge, this is the first description of the operations of an African helicopter rescue service.
Methods
A 5-y retrospective review of the terrestrial and aquatic helicopter rescue activity of a civilian-operated HEMS in the Western Cape, South Africa, from January 1, 2012 through December 31, 2016, was conducted. Data were extracted from the organization’s operational database, aviation documents, rescue reports, and patient care records. Patient demographics and activity at the time of rescue, temporal and geographical distribution, crewing compositions, patient injury, triage, clinical interventions, and rescue techniques were analyzed.
Results
A total of 581 SAR missions were conducted, of which 451 were terrestrial and 130 were aquatic rescues. The highest volume of rescues was conducted within the urban Cape Peninsula. Hoisting using a rescue harness was the most common rescue technique used. A total of 644 patients were rescued, with no or minor injuries representing 79% of the sample. Trauma (33%, 196/644) was the most common medical reason for rescue, with lower limb trauma predominant (15%, 90/644). The most common clinical interventions performed were intravenous access (n=108, 24%), spinal immobilization (n=92, 21%), splinting (n=76, 17%), and analgesia administration (n=58, 13%).
Conclusions
The rescue techniques utilized are similar to those described in high-income settings. Uninjured patients comprised the majority of the patients rescued.
Keywords
Introduction
The use of helicopters for search and rescue (SAR) reduces morbidity and mortality by decreasing time to access to emergency medical care and evacuation to an appropriate medical facility.1,2 Helicopter rescue systems operate predominantly in high-resource settings and have contributed significantly to the capabilities of rescue services in dangerous or inaccessible terrain through rapid patient access, delivery of appropriately trained personnel, and timely transport to medical facilities for critically ill and injured patients.2,3
In Africa, helicopter emergency medical service (HEMS) SAR capabilities are limited and are generally conducted by the military. The Western Cape Province of South Africa is the exception, where a civilian-operated HEMS, subcontracted by the provincial government, has partnered with volunteer rescue organizations and provincial emergency medical services (EMS) to conduct terrestrial and aquatic rescues since 2002. The South African Red Cross Air Mercy Service (SARC AMS), a nonprofit organization, operates 2 helicopter bases in the Western Cape—one in Cape Town in the west of the province and one in Oudtshoorn in the east. Each base has 1 helicopter. The subcontracted model includes air ambulance operations, with a focus on rural aeromedical retrieval as well as rescue operations. Missions are dispatched centrally through a specialized provincial EMS dispatch center, with authorization for dispatch of the HEMS for all missions obtained from a core group of senior medical doctors from provincial EMS management.
The SARC AMS utilizes the single-engine Augusta Westland AW119 helicopter as a rescue platform, with hoisting and longline capabilities. All rescues are conducted under visual flight rules as a single pilot operation with assistance from an external load operator. Rescues are conducted using mission-dependent deployable multidisciplinary teams from various organizations and with varying medical training. The medical crew is primarily EMS personnel with qualifications ranging from basic to advanced life support. Doctors are utilised when specifically required, with limited availability.
The Western Cape is the southernmost of the 9 South African provinces, spanning 129,462 km2, with approximately 6.2 million inhabitants, the majority of whom are located within the Cape Town metropolis. The province is a popular travel destination for local and international travelers with seasonal influxes of visitors over the hot and dry summer months from December to February. Of specific interest to this study, Table Mountain National Park (TMNP) is an open-access national park within the Cape Town metropolis, spanning 212 km2 from Table Mountain to Cape Point, and receives an estimated 4 million visitors per annum, including 1 million summiting Table Mountain via cable car. The role of a helicopter-based rescue service in low-resource settings is not yet well described. A better understanding of this service within a resource-constrained public sector could provide insights to other low-middle income settings with an emphasis on the provision of services with equitable benefit. By bringing an external resource into a limited resource setting, such as in rural health systems, aeromedical services do not deplete limited local resources. This is particularly important when highly skilled resources are required or protracted transport times delay the return of potentially limited local resources to their service area.
In this mixed-service operation, the availability of HEMS must be closely managed to regulate costs and provide maximum benefit to patients and the EMS system. Through an improved understanding of the utilization of the service for SAR operations, multiple factors affecting the rescue operations such as budget allocation, equipment, training, and personnel requirements can be optimized. Of importance, in this setting, helicopters occupied in SAR operations are not available for air ambulance services, and as such, SAR dispatch criteria should be evidence based, as has been developed for HEMS. 4
To our knowledge, there are no published data to understand the overall service demand and delivery of an African HEMS SAR service. The aim of this study was to describe the helicopter rescue activity of a civilian-operated HEMS in the Western Cape, South Africa.
Methodology
A retrospective descriptive analysis was conducted over the 5-y period from January 1, 2012 through December 31, 2016. For the purposes of this study, rescue was defined as a helicopter flight including the search for and/or extrication of persons with medical or situational difficulties in terrestrial (such as mountainous or remote terrain) or aquatic (including sea, river, and any expanse of water) terrain. All helicopter missions that were not rescue related were excluded from analysis.
Multiple primary data sources, including organizational aviation documents, operational rescue reports, and patient care records, were utilized for data collection. The data captured for analysis included geographical, temporal, patient, and operational rescue data. The patient and clinical data collected were limited to age, sex, activity prior/leading to rescue, medical interventions performed, patient acuity, provisional diagnosis, and disposition. Patient acuity was described using the South African Triage Score (SATS), a previously validated triage scale utilized by the Western Cape Emergency Medical Services. 5 Red code patients require immediate medical care; orange code patients require urgent care; yellow code patients and green code patients require less urgent medical attention. Critical patients were defined as patients with initial triage of red or orange code, including patients who died during the rescue. Patients triaged as blue were fatalities. The geographical data included rescue location and terrain. The operational rescue data included rescue crew composition, highest medical crew qualifications, and rescue techniques used to conduct the rescue.
The broad criteria for inclusion into the study included the following: helicopter rescue activity of the Cape Town and Oudsthoorn bases of the SARC AMS, including both aquatic and terrestrial helicopter rescues conducted during the defined study period. Cases were excluded if they were terrestrial or aquatic helicopter rescues completed by other organizations, were conducted outside of the Western Cape Province of South Africa, or were service requests for rescue missions during which the helicopter did not take off or reach the rescue scene. When the minimum required patient data were missing or incomplete, the rescue information was included for analysis but not the patient data.
Univariate descriptive analysis was used to summarize and report on the geographical, temporal, patient, and operational rescue data. Means
Results
Between January 1, 2012 and December 31, 2016, a total of 4998 HEMS missions were conducted by SARC AMS in the Western Cape, of which 581 (12%) were rescue missions (Table 1). In general, helicopter rescue activity did not increase per annum over the 5-y sample; however, a reduction in aquatic rescue activity was apparent (Table 1, Figure 1). A seasonal surge was evident in the summer months, with 42% (245/581) of rescues conducted between December and February (Figure 2). Peak rescue times occurred between 1300 and 1800 (Figure 3) and on weekends (45%, 266/581; Figure 4).
Aquatic and terrestrial rescue missions per annum
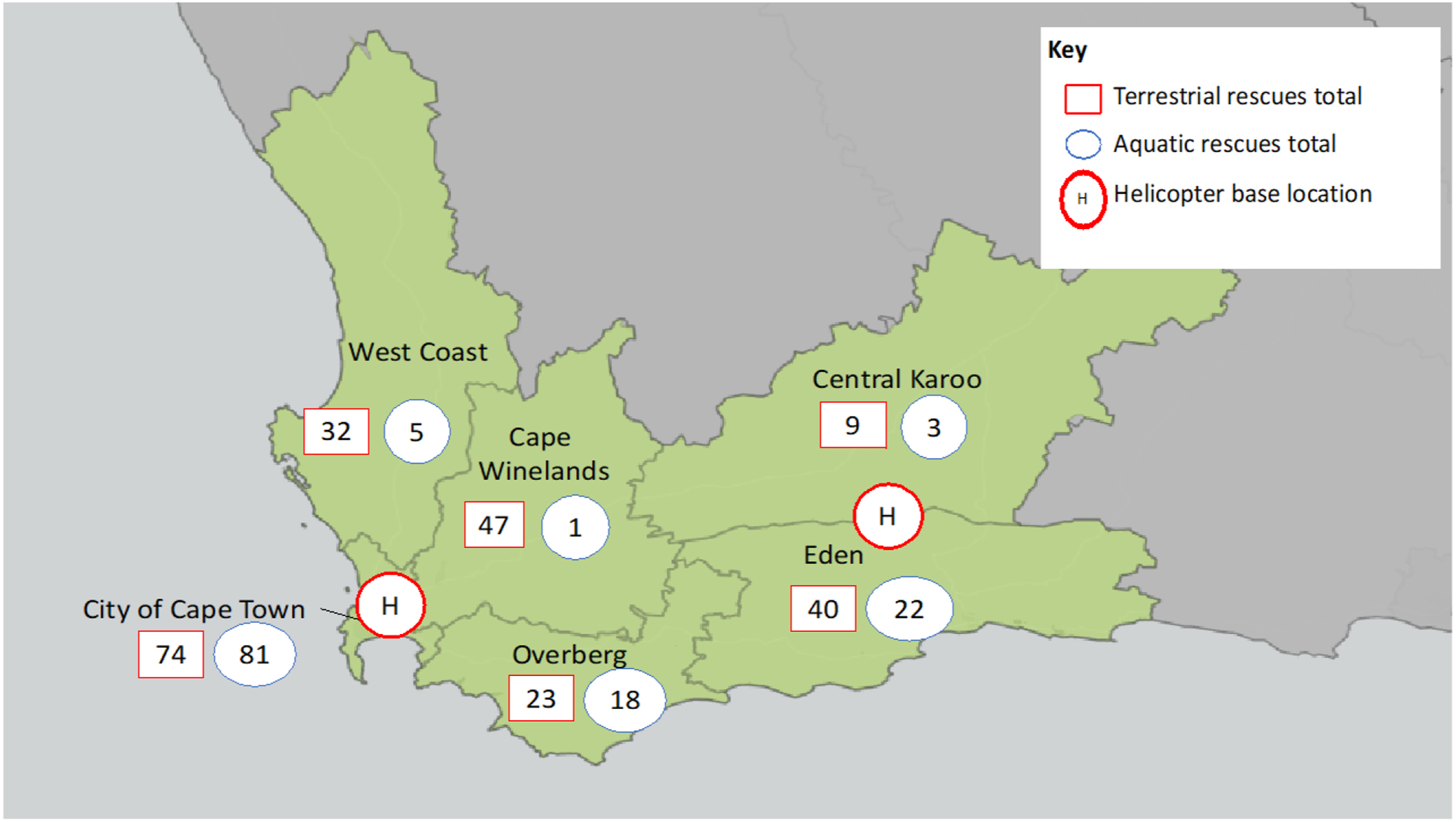
Map of rescue activity over 5 y by the municipal district in the Western Cape. Emergency medical service resources are distributed by municipal district. This figure represents the rescue activity per district, highlighting areas of frequent rescue activity.
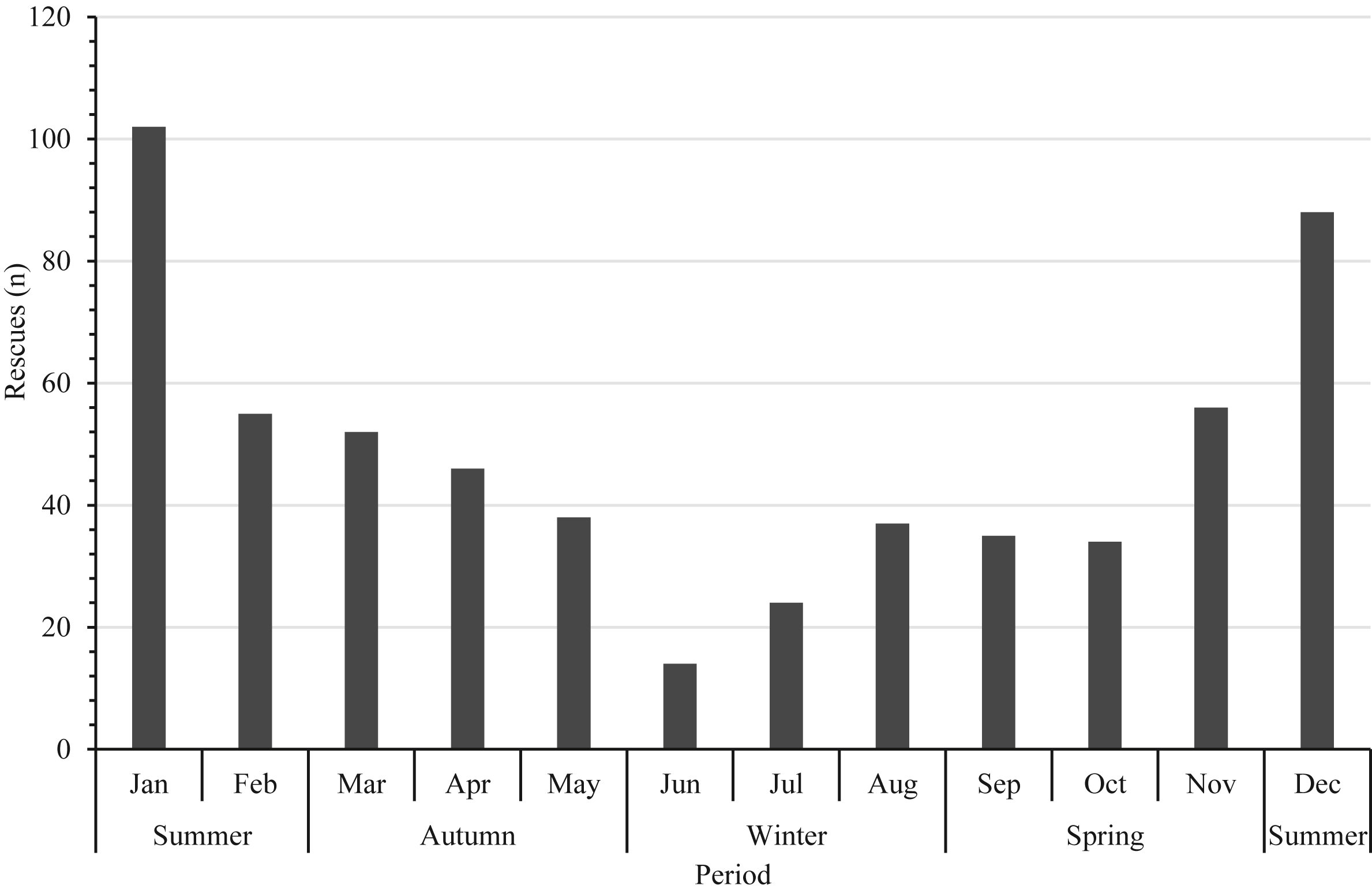
Temporal distribution of rescue activity.
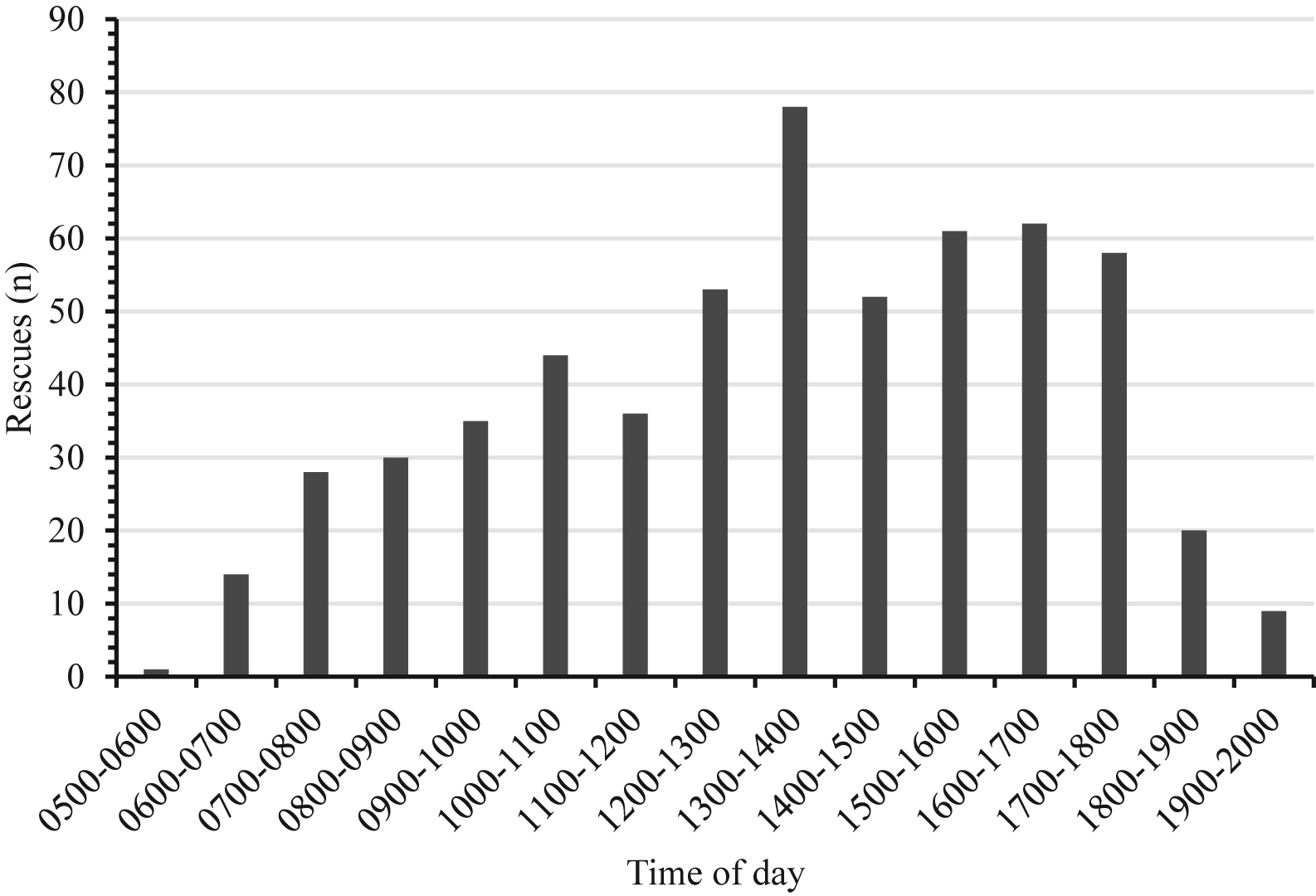
Time of departure for rescue.
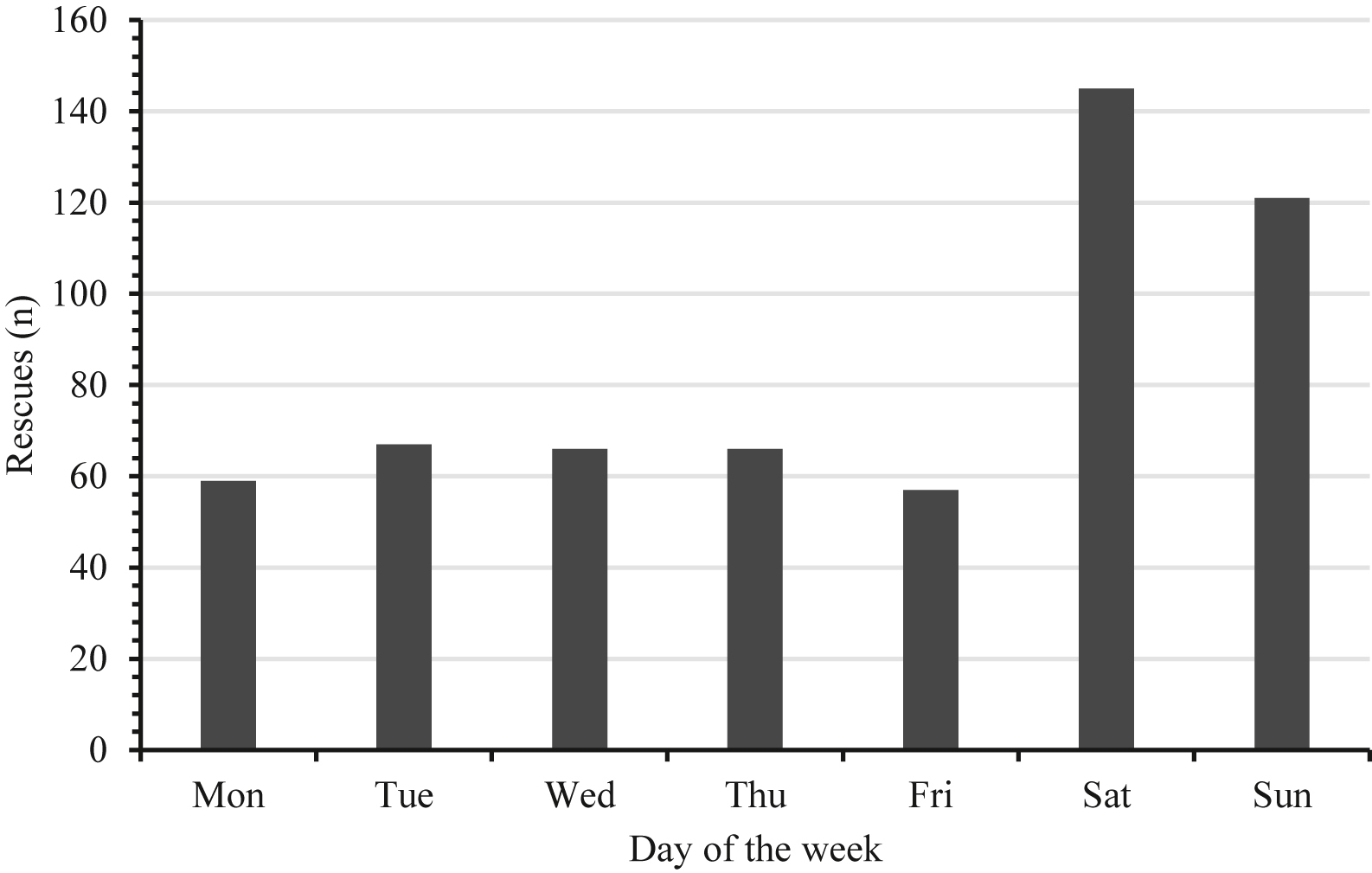
Number of rescues per day of the week.
In 71% (410/581) of the missions, a patient or party was located and extracted by helicopter. In an additional 8% (48/581) of the missions, the rescued patient or party was extricated by alternative means such as a boat or ground crew. No person was found by any party (ground or HEMS) at the conclusion of 19% (108/581) of the SAR missions (Figure 5). In 15 missions, the aircraft was stood down, unable to complete the mission because of safety concerns or because data were missing (Figure 5). The mission time from take-off to mission completion (ie, helicopter returned to base) was 2:15
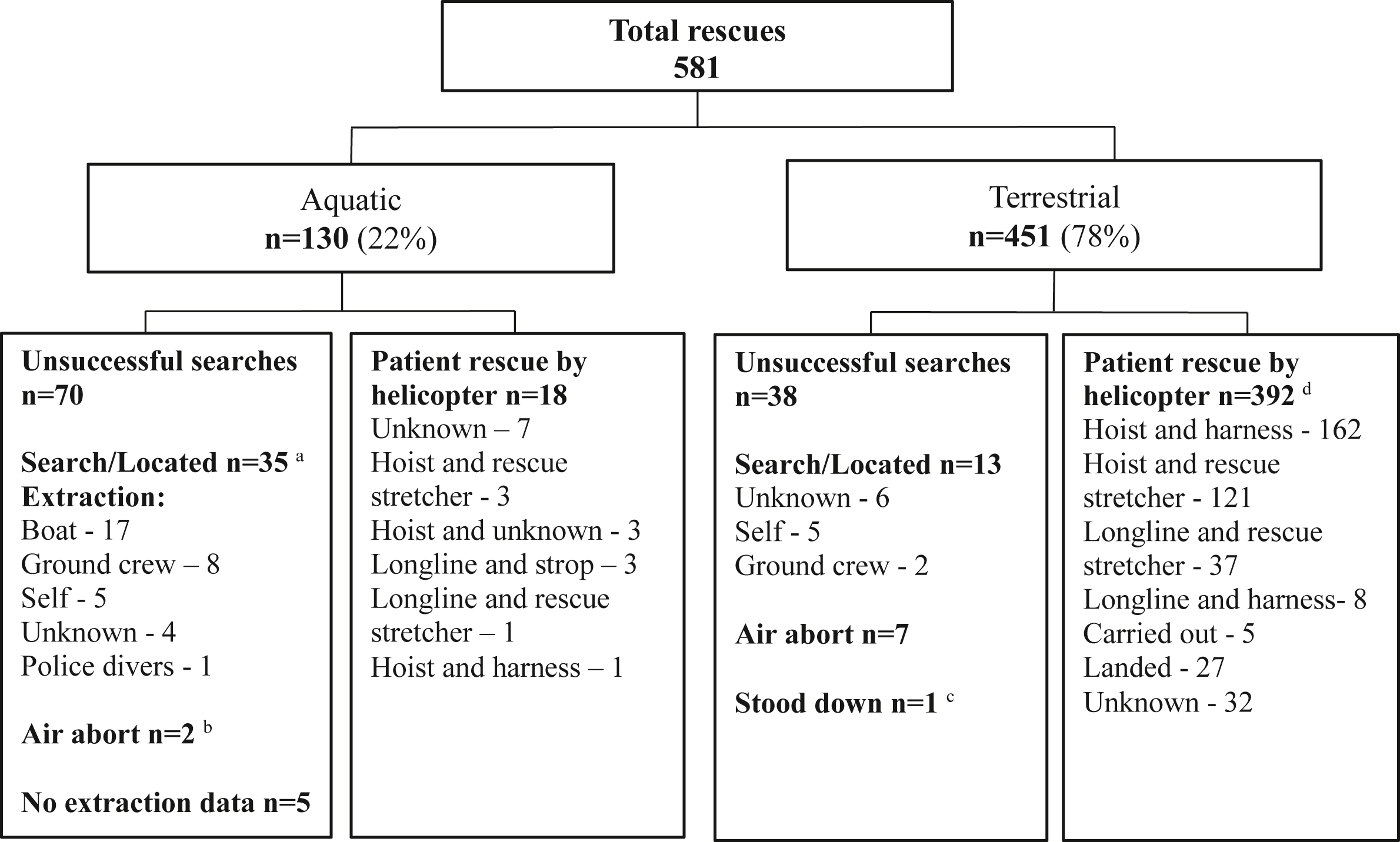
Rescue missions and patient extrication techniques utilized. a On 7 rescues, patients extricated by boat and ground crew required medical intervention from helicopter emergency medical service crew. b Helicopter mission stopped because of unsafe conditions such as weather or technical safety concerns. c Stand down during search as patient found safe elsewhere. d Some rescues involved multiple patients.
Rescues around the Cape Town metropolis accounted for 66% (299/451) of terrestrial rescues, with 50% (226/451) of all terrestrial rescues occurring in the TMNP (Figures 5 and 6). Nearly half of all rescue activity within TMNP was conducted on the popular hiking trails Platteklip Gorge (n=74, 25%), Lions Head (n=47, 16%), and India Venster (n=14, 5%) on Table Mountain (Figure 6). Dehydration or heat-related illness was the primary reason for rescue in 14% of patients rescued from TMNP.
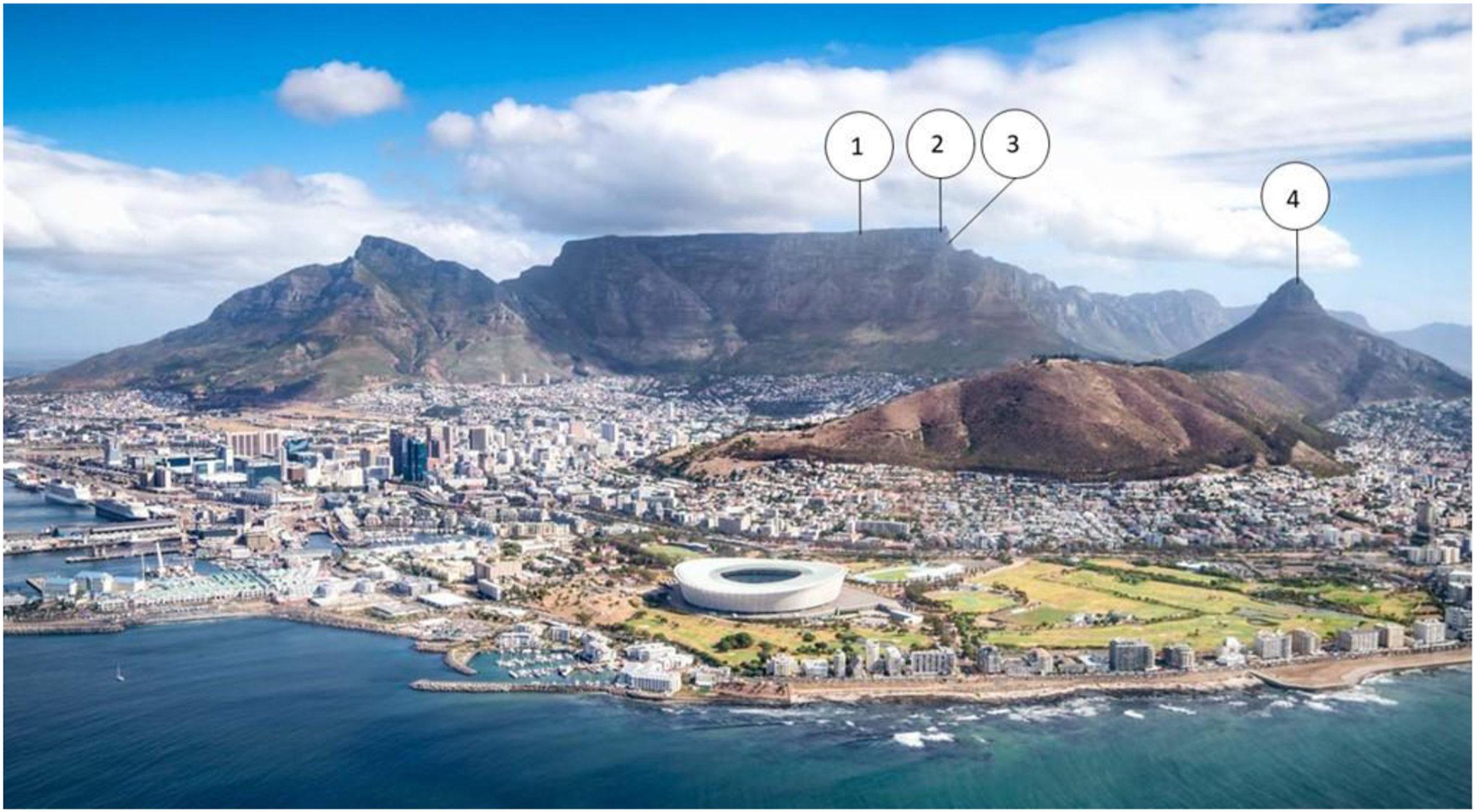
Common rescue sites in Table Mountain National Park. 1, Top of Platteklip Gorge hiking trail; 2, Table Mountain cable car station; 3, Top of India Venster hiking trail; 4, Top of Lions Head hiking trail.
For aquatic activity, patients were rescued using a helicopter in 14% (18/130) of missions undertaken, with 54% (70/130) of the missions resulting in unsuccessful searches in which no patient was found (Figure 5). There was patient contact by the HEMS crew in 41 (32%) of total aquatic rescue cases, of which 50% (20/41) were fatalities.
Patient details were available for 93% (600/644) of persons rescued by helicopter. Adult patients (≥18 y) comprised 93% (551/600) of the sample. The patients were more commonly men (61%, 352/600), with a median age of 40 y (IQR, 19–85 y) for both sexes. The median age of adolescent patients (age, 13–18 y) was 16 y (13–18 y, age recorded for 27/32). Pediatric patients represented 2% (11/600) of the sample, with a median age of 7.5 y (3–11 y, age recorded for 8/11). Hiking and swimming were the most frequent activities, accounting for 71% (429/600) and 7% (40/600), respectively. Single patient rescues accounted for 60% (354/581) of all rescue missions, with multiple patients rescued in 14%. More than 3 persons were rescued in 6% of rescues undertaken, with all patients uninjured in rescues involving 6 to 20 patients.
Uninjured and less urgent patients (SATS triage coded green and yellow) comprised 79% of the sample (Table 2), received the fewest interventions, and were least likely to receive further care. Medical assistance was required for 343 (57%) patients, of whom 230 (60%) were transported to hospital for further care: 73 by helicopter and 157 by ground ambulance. Patient care records were available for 35% (119/343) of the patients treated. Patient care records were not available for 41% (19/45) of patients who were triaged as red code.
Patient diagnosis and triage
Deceased persons.
Includes abdominal pain, anaphylaxis, overdose (unknown substance), shortness of breath, and syncope.
Six patients with no triage or diagnosis documented were excluded from the table.
Lower limb trauma, dehydration, and spinal injury were the most common diagnosis (Table 2). Polytrauma patients comprised 7% (40/600) of all patients and accounted for 38% (22/58) of critical patients triaged orange or red code.
A total of 444 medical interventions were performed on 230 of the 343 patients requiring medical assistance (Table 3). The most common interventions were intravenous access, spinal immobilization, and limb splinting (Table 3). Trauma patients required 77% (340/444) of all interventions. Critical patients (10%, 58/600), defined as patients who triaged orange or red, required 43% (189/444) of the interventions, including endotracheal intubation, assisted ventilation, sedation, drug administration, intraosseous access, and needle thoracentesis. The medications administered included analgesics, sedatives, cardiac drugs, dextrose, antiemetics, and inotropes. Return of spontaneous circulation was achieved in 3 of 7 attempted resuscitations, including 2 children who were successfully resuscitated after drowning. The number of interventions during cardiopulmonary resuscitation was 6 (range, 6–8).
Most frequent clinical interventions performed a
Some patients required multiple interventions.
Warming, cooling, dextrose administration, intraosseous access, and needle thoracentesis.
There were 64 deceased patients recovered, with hiking (41%, 26/64), swimming (16%, 10/64), and fishing (6%, 4/64) accounting for the most activity in this subset. On arrival of rescue personnel, 94% (60/64) were deceased on first contact, and 4 patients died during the rescue.
Discussion
These data suggest that the SAR operations of a civilian-operated HEMS in the Western Cape of South Africa are not unlike rescue operations described in the international literature, most of which are in high-income settings, although the differing methodologies make comparison difficult. Temporal peaks, rescue techniques, and crewing configurations are similar to high-income countries across Europe, North America, and Australia. 6 -10 In this mixed-use aeromedical model, the utilization of HEMS for rescue represented 12% of all missions undertaken, which is higher than other mixed-model operations with similar crewing configurations. 6
The Western Cape is a popular tourist destination for local and international visitors during summer periods, which correlates with the increase in rescue activity. Popular travel destinations in Europe, North America, and Asia have reported similar temporal trends in HEMS rescues. 11 -14 The increase in rescue demands over weekends and afternoons further demonstrates the largely recreational activities, such as hiking and running, requiring rescue efforts.
The usage of helicopters in SAR has demonstrated patient benefit, with rapid rescue preventing further harm and limiting risk for both patients and rescuers and providing expeditious access to medical care. 2 The use of helicopters for SAR has been shown to reduce morbidity and mortality.1,2 Helicopter SAR epidemiology globally demonstrates 2 predominant groups of persons requiring rescue: uninjured persons and those who have sustained trauma.6,7,12,14-18 Over 40% of the persons rescued in this study were uninjured and required situational assistance because of inaccessibility, as reported in other HEMS SAR operations.6,7,14,19 In Australia, persons with minor or no injuries have been reported to constitute 90% of HEMS SAR missions. 6 Male adult patients who had sustained trauma were found to be the most common group requiring rescue, which aligns with trends in international systems.8,12,14,17,20 In Canada, Europe, Australia, Nepal, Taiwan, and the United States, male patients sustaining minor trauma comprise a large proportion of rescues. 6 -8,12-14,17,21-23 The proportion has been reported as high as 78% of all persons rescued. 8
The data highlighted several high-risk areas where frequent helicopter rescues occur, which can inform injury prevention strategies. Most terrestrial rescues occurred on popular hiking trails and tourist destinations in TMNP. Two hiking trails in TMNP, namely, Platteklip Gorge and Lions Head, accounted for one-quarter of all terrestrial rescues undertaken in the province, with the predominant reasons for rescue including dehydration and heat-related illness. One in 10 patients in the Western Cape required rescue for dehydration or heat-related illness, some of whom were critically ill and required advanced life support intervention. The substantial proportion of patients with potentially preventable causes for rescue, such as dehydration and heat-related illness on popular hiking trails and drowning near popular beaches, provide areas of focus for injury prevention strategies. 24 Interventions, such as increased signage and public awareness campaigns, would seem to be viable prevention strategies. 24
Drowning is a significant cause of unintentional death in South Africa, especially among children under the age of 15, with no national drowning prevention strategy in place. In the Western Cape, 42% of fatal drownings occur during the peak summer period, consistent with the increased aquatic rescue activity. 25 The high incidence of drowning around the coastline of the Cape Town metropolis and increases in drowning over weekends align with findings in the provincial drowning prevention framework. Although helicopters have been shown to be effective in aquatic SAR and are used extensively in both military and civilian settings, patients were rescued by helicopter in only a small proportion of aquatic rescue missions in the Western Cape.10,26 The factors affecting the aquatic rescue success may include the time between incident occurrence and request for assistance and response time to the scene. These factors require further investigation to optimize resource utilization and benefit. During aquatic rescue, the multiagency approach was evident in boat and ground crew patient extractions following helicopter location of the patient.
The rescue configuration and standard crewing of the SARC AMS meets international helicopter medical rescue recommendations. 2 Although many international systems use doctors for HEMS rescue, the availability of doctors in the prehospital setting in South Africa is limited. The most common medical interventions performed in HEMS SAR include analgesia, intravenous fluid administration, and oxygen administration in international HEMS rescue,2,6,21 with splinting and spinal immobilization also frequently performed in the Western Cape. Critical care interventions, such as endotracheal intubation, are uncommon in the HEMS rescue setting. 27 Advanced life support paramedics were most commonly utilized as the primary medical provider in this setting and would seem to be appropriate given that they are able to perform all common interventions as well as critical interventions such as rapid sequence intubation.
Patients with an initial SATS triage code of red, including 4 in-care deaths during rescue, comprised 10% of the sample and required more clinical interventions than the other triage groups. Nearly half of red triage patients sustained significant polytrauma requiring advanced life support interventions. Although critical advanced life support skills such as advanced airway management are infrequently performed in the rescue environment before extraction, these skills are important to prevent further morbidity and reduce mortality. 28 International guidelines on the determination of death in the wilderness environment detail the difficulties experienced in patient examination, access, poor patient history, and access to cardiac monitoring. 29
Multipatient incidents accounted for 14% of rescues, and although not as frequent as single-patient rescues, multipatient rescues of >3 persons pose significant logistical and operational challenges for rescue personnel, including carrying limited equipment for extrication. It is of note that the large multipatient rescues undertaken in this sample involved largely uninjured patients, requiring primarily situational assistance. Helicopters are beneficial for multipatient incidents and can be used to both deploy extra assistance at the scene as well as in patient evacuation. 30
The SARC AMS HEMS operation serves as a rescue platform and an aeromedical service, performing interfacility transfers and primary emergency scenes and servicing a vast low-resource rural population. The selection of cases for dispatch of this resource must be considered in the light of beneficence, and further research is required to describe the case-mix of the operation. Rescue missions may require several hours of dedicated time, limiting the availability of the resource for medical missions. Although some data describe no trauma mortality benefit for the use of HEMS in the South African setting, 31 further research on dispatch criteria and benefit in the rescue setting is needed.
Limitations
Only missions conducted utilizing the SARC AMS helicopters were described, with the exclusion of the South African Air Force and any ground rescue operations. The South African Air Force performed only 10 terrestrial helicopter rescues during the sample period, which were not included in this research. This research represents the activity of a single civilian-operated service providing both aeromedical and rescue services in a state service within a single province with unique and varied geography, which may limit applicability to other settings.
Data were limited by the consistency of the records kept and the availability of records, particularly patient care records. Clinical information was limited by the availability of the records, with missing records possibly because of patients being handed over to EMS staff for transport or further treatment. More than half of records for patients requiring medical treatment or who triaged red were not available, which limits the strength of data in this area.
As the research was retrospective, the data set was not designed for the purpose of this research. Records were captured as found, with incomplete data detailed in the results. The challenges in data capture included incompleteness of records and records being kept in different sites in the organization, prolonging the time period required for data capturing because of travel.
Conclusions
Rescue techniques and crewing configurations are similar to those described in high-income settings. Uninjured and less urgent patients comprised the majority of the sample, with trauma the most common medical reason for rescue. Evidence-based prevention strategies should be considered to strategically decrease rescue demand. Improved understanding of the SAR operations of this service can inform beneficent and fair utilization of resources in a mixed-model aeromedical and rescue HEMS operation in a resource-constrained prehospital setting.
Footnotes
Acknowledgment
We acknowledge the contributions of Wayne Smith who provided invaluable insight into the writing of this manuscript.
Author Contributions: Study concept and design (JFPR, IH, PH); data acquisition (JFPR); data analysis (JFPR, IH, PH); drafting of the manuscript (JFPR, IH, PH); critical revision of the manuscript (JFPR, IH, PH); approval of final manuscript (JFPR, IH, PH).
Financial/Material Support: None.
Disclosures: JPR and IH are former employees of the SA Red Cross Air Mercy Service and as such recognize the potential for organizational bias.