
Abstract
Elderly patients with lower extremity fractures are at high risk for deep vein thrombosis (DVT) and its potentially fatal complication, pulmonary embolism. As perioperative physicians, anesthesiologists serve pivotal roles in mitigating thrombosis risk and optimizing patient outcomes, thus requiring a comprehensive understanding of the pathophysiology and management of DVT in this vulnerable population. Despite its significant clinical importance, comprehensive literature on perioperative DVT management for elderly patients with lower extremity fractures remains scarce. This review synthesizes evidence regarding epidemiology, pathophysiology, diagnostic challenges, multimodal prevention strategies for fracture-related thrombosis, and specific anesthetic considerations for this vulnerable population. It emphasizes the importance of routine preoperative Doppler ultrasonography and early DVT prevention. Besides pharmacological prevention, physical prevention and early mobilization constitute essential DVT prophylaxis components. Anesthesiologists must judiciously weigh thromboprophylaxis benefits against hemorrhage risks while addressing the inherent conflict between preoperative comorbidity optimization and timely surgical intervention, striving to perform surgery within 48 h after injury. Intraoperatively, neuraxial anesthesia should be preferred in the absence of contraindications, and anticoagulation and effective analgesia should be resumed early postoperatively to facilitate early mobilization. Through rigorous evaluation of contemporary literature and clinical practice, this review delivers evidence-based recommendations to enhance clinical decision-making and improve perioperative anesthesia management for this high-risk population.
Introduction
Lower extremity fractures account for one-third of all fractures, and most of them occur in the elderly. 1 Elderly patients with fracture are particularly prone to deep vein thrombosis (DVT) and its potentially fatal sequelae, such as pulmonary embolism (PE), due to physiological aging, trauma-induced hypercoagulability, and immobilization. DVT constitutes a severe complication for elderly patients with lower limb fractures, affecting fracture treatment and potentially leading to mortality. 2 The risk of death among elderly patients with hip fracture is threefold higher than their age-matched controls, primarily attributed to perioperative thromboembolic events. Besides the risk of fatality, DVT contributes to long-term sequelae, such as post-thrombotic syndrome, chronic venous insufficiency, and reduced functional recovery, which are outcomes especially detrimental to the already vulnerable elderly population striving to regain activity and independence. Given the aging populations, increasing diabetes/obesity prevalence, increasing cancer incidence, and suboptimal thromboprophylaxis, DVT incidence is growing, 3 and the urgency to address DVT prevention and management has become increasingly critical.
Elderly patients with lower extremity fractures frequently exhibit complex comorbidities such as cardiovascular diseases, chronic kidney diseases, diabetes mellitus, malignancies, and inflammation. Perioperative care necessitates optimization of reversible conditions caused by the primary diseases and their associated thrombotic susceptibility, which may delay surgery. 4 Delayed surgery not only increases the risk of thromboembolism but also prolongs the duration of immobilization, muscle wasting, cognitive decline, delirium, and cardiopulmonary deconditioning. Delayed surgery poses dual clinical challenges: the need for early surgical fixation to restore mobility and reduce complications, and the complexity of perioperative decision-making due to preexisting conditions and DVT risk. Therefore, early diagnosis, preoperative planning and conditioning, vigilant intraoperative maintenance of stable vital signs, and prompt management of unexpected events are of utmost importance.
The perioperative period is a critical time for optimizing DVT management, and anesthesiologists play a pivotal role in this phase. Currently, various countries have guidelines for the prevention of venous thrombosis after hip fractures and hip or knee replacement surgery. However, consensus has yet to emerge on DVT prevention for elderly patients with lower extremity fractures, particularly regarding perioperative management. This work aims to provide a comprehensive review addressing the following: (1) epidemiology and impact; (2) pathophysiological mechanisms and risk factors; (3) diagnostic methods; (4) prevention strategies, including mechanical, pharmacological, and integrated approaches; and (5) timing of surgery; (6) intraoperative management and postoperative considerations. By integrating data from clinical studies, consensus guidelines, and innovative research, it seeks to provide evidence-based guidance for clinical practice and assist anesthesiologists in making informed decisions regarding the management of these complex patients while balancing the risks of thrombosis and bleeding.
Epidemiology and Impact
Limited data exist on perioperative DVT in elderly patients with lower limb fractures, and its incidence remains uncertain. In a retrospective study of 848 patients with lower-extremity fractures by Dashe et al, venous thromboembolism (VTE) occurred in 32 patients (3.8%). 5 In Zhang et al's retrospective cohort study of 462 patients aged 50 years and over with lower extremity fractures, 337 patients (72.9%) were diagnosed with DVT during the perioperative period. 6 Cong et al found preoperative DVT in 821 (29%) of 2831 patients with lower extremity fractures. 7 Li et al's retrospective study found that 68 of 829 patients (8.2%) with lower extremity fractures developed DVT during the perioperative period. 8 The incidence of DVT varies across different studies, possibly due to the following factors: (1) variations in the age range of the study population; (2) differences in the male-to-female ratio, because gender can influence DVT incidence rates; (3) divergent severity and patterns of injury; (4) disparities in the time from injury to hospital admission due to factors such as transfer to higher-level hospitals, economic disparities, and differences in knowledge levels; (5) variations in the time from admission to examination, examination methods, frequency of examinations, and the technical proficiency of diagnostic imaging personnel, depending on hospital resources and expertise; (6) differences in anticoagulation philosophies, methods, and medications used after admission; (7) discrepancies in inclusion criteria such as whether the fracture is pathological, the presence of primary diseases like inflammatory disorders or coagulation abnormalities, and whether anticoagulation therapy is currently being administered; (8) divergent study timeframes, with some studies focusing on DVT incidence at admission, others at pre-operation, and some during the perioperative period. Numerous factors such as these can influence the incidence of DVT.
Although the incidence of DVT varied across studies, this work sought to identify patterns. Taoka et al showed that preoperative VTE occurred in 436 (40%) of 862 elderly patients with hip fractures. 9 A meta-analysis by Wang et al found that the incidence of preoperative DVT in patients with hip fracture was 16.6% (1627/9823). 10 Zhang et al retrospectively analyzed 274 elderly patients with simple hip fractures and detected DVT in 33% of them. 11 Zhang et al followed up 140 patients over 60 years old with closed distal femoral fractures and found that the overall incidence of DVT was 35.0%. 12 In another study, a total of 432 patients with femoral shaft fracture were retrospectively analyzed, of whom 114 patients (26.4%) were diagnosed with DVT before operation. 13 Sun et al studied 237 cases of femoral shaft fractures and found that 54 cases (22.78%) had DVT during the perioperative period. 14 Williams et al reported a 12% incidence of DVT in patients with isolated calcaneal fractures. 4 A retrospective analysis of patients with lower extremity fractures showed that the incidences of DVT in hip, femoral, and tibial fractures were 44.2%, 32.8%, and 16.4%, respectively. 15 Zhang et al conducted a multicenter cohort study showing that the incidence of DVT was 14.36% (50 of 348), 12.06% (28 of 232), 14.28% (44 of 308), 32.33% (54 of 167), 27.65% (86 of 311), and 29.56% (68 of 230) in patients with ankle–foot, tibia–fibula, peri-knee, femoral shaft, peri-hip, and pelvic fractures, respectively. 16 In a retrospective study of 829 cases of lower limb fractures by Li et al, the incidence of DVT in hip, femoral shaft, knee, calf, and foot and ankle fractures were 16.7%, 12.2%, 9%, 3.7%, and 2.3%, respectively, 8 indicating higher incidence of DVT in proximal fractures. 17 In conclusion, the incidence of preoperative DVT is higher than that of postoperative DVT 18 ; the incidence of distal DVT is higher than that of proximal DVT18–20; and the incidence of DVT in the fractured limb is much higher than that of the healthy limb.18,20
Despite advances and the reduced incidence in DVT, it remains one of the most common vascular disorders globally, following coronary artery disease and cerebrovascular disease, ranking third in global economic burden.21,22 When embolized or dislodged, the thrombi from DVT can lead to PE, which is the third leading cause of death in patients who survive the first 24 h after trauma.23,24 The reported mortality associated with complications of DVT, particularly PE, is relatively high, ranging from 5.0% to 23.0%. 25 The clinical influence of DVT in elderly patients with fracture extends far beyond the acute thrombotic event. DVT survivors experience significantly delayed rehabilitation progress, with one study demonstrating 23% lower mobility scores at 6 months compared with non-DVT counterparts. Postthrombotic syndrome (PTS) refers to the chronic venous dysfunction of the lower extremity, which is secondary to DVT. It is generally characterized by swelling and pain, heaviness, pruritus, or pigmentation of the affected legs. 26 Chronic pain, secondary varicose veins, and recurrent and intractable ulcers may occur in severe cases and even after anticoagulant therapy of DVT.17,18 It could severely compromise quality of life and increase the social and economic burden. 27 Effective prevention of DVT is the most critical measure for preventing the occurrence of PTS. Therefore, adherence to current guidelines to avoid DVT can effectively prevent PTS. However, developing effective individualized prevention strategies and perioperative anesthesia protocols tailored to the comorbid conditions and DVT susceptibility of elderly patients with fracture remains challenging. A further in-depth understanding of the complex pathophysiology underlying their thrombotic risk is warranted.
Pathophysiology and Risk Factors for DVT in Elderly Patients with Fracture
The main pathophysiological mechanism of DVT in elderly patients with lower limb fractures is the complex interaction of Virchow triad (venous stasis, endothelial injury, and hypercoagulable state). 28 Understanding these mechanisms is essential for anesthesia providers to assess risk and implement appropriate preventive measures.
Venous stasis occurs dramatically in patients with lower limb fracture due to multiple factors. Immobility preceding and following fracture contributes to venous stasis significantly. 20 Elderly patients often have reduced mobility even before injury due to comorbid conditions, and the fracture itself causes painful limitation of movement. 29 Age-related reductions in venous compliance (up to 30% decreased elasticity in elderly veins) further exacerbate stasis, while comorbid conditions like heart failure or chronic venous insufficiency present in many older adults add to the hemodynamic compromise. 10 During anesthesia, the loss of the “muscle pump” effect from paralyzed skeletal muscles further exacerbates venous stasis, and general anesthesia (GA) with positive pressure ventilation decreases venous return. 30 Bed rest further reduces cardiac output and systemic venous flow. 30 These factors combine to create ideal conditions for thrombus formation in the deep venous system of the lower extremities.
Venous injury occurs at the time of fracture and during subsequent surgical repair. The traumatic disruption of bones and surrounding tissues directly damages adjacent veins, exposing subendothelial collagen and initiating the coagulation cascade. Notably, even minimally displaced fractures can trigger considerable activation of coagulation pathways due to the release of bone marrow contents and fat emboli into the circulation. Surgical manipulation during fracture fixation compounds this injury through local compression, retraction, and potential direct venous trauma. The inflammatory response caused by endothelial cell injury leads to the overexpression and interaction of many cells, molecules, and cytokines, possibly leading to endothelial cell injury and death. 31 Tissue edema and compartment syndrome caused by trauma can lead to limb ischemia and subsequent reperfusion injury, resulting in oxidative stress that further exacerbates vascular endothelial injury. Moreover, hemorrhagic shock, hypoperfusion, and ischemia–reperfusion after fluid resuscitation in patients with multiple trauma contribute to vascular injury. 32
Hypercoagulability in elderly patients with fracture stems from multiple sources. Exposure of subendothelial collagen and tissue factor activates the coagulation cascade, thereby promoting a hypercoagulable state. 33 In addition, inflammation inhibits fibrinolysis through increased plasminogen activator inhibitor-1 (PAI-1). Age-related changes in coagulation factors tilt the balance toward a prothrombotic state even before injury. Comorbidities common in this population, including heart failure, malignancy, and chronic inflammatory conditions, further amplify thrombotic tendencies.
The occurrence of DVT is influenced by multiple factors. First, in the pre-fracture stage, various pre-existing chronic disorders, such as hypertension, cardiovascular disease, diabetes mellitus, rheumatoid arthritis, hematologic diseases, and chronic kidney disease, can affect the development of DVT.6,34–36 A meta-analysis by Qian et al indicated that a history of VTE, age over 60 years, obesity, prolonged bed rest, and heart failure are significant risk factors for DVT in patients with lower limb fractures. 37 Second, during the pre-operative period after fracture, the time from fracture to hospital admission is a risk factor for DVT. 38 A study conducted by Cong et al found that time from injury to surgery (TFITS) is an independent risk factor for preoperative DVT, with each additional day in TFITS increasing the risk of preoperative DVT by 9.3%. 7 Lower limb fracture itself is a risk factor for DVT in patients undergoing orthopedic surgery.30,39 Chang et al suggested that age, presence of diabetes, and fracture site are independent risk factors for preoperative DVT in patients with lower limb fractures. 40 Through univariate analysis, Yang et al identified age, BMI, serum calcium level, multiple fractures, hypertension, hypoproteinemia, and hyperglycemia as factors associated with postoperative DVT in patients with lower limb fractures. 41 Finally, operative procedures during surgery can influence the occurrence of DVT. A retrospective study by Li et al showed that fracture site, advanced age, longer operative time, and joint replacement are risk factors for DVT in patients with lower limb fractures, whereas pre-injury physical activity and postoperative exercise are protective factors. 8 Prolonged bed rest, surgical intervention, trauma, and genetic predisposition have been implicated in DVT development. 42 A retrospective study by Yang et al found that advanced age, hyperglycemia, surgical treatment, and long disease duration are independent risk factors for lower limb DVT in elderly patients with hip fractures. 43 Xie's study suggested that the use of a tourniquet increases the incidence of postoperative DVT. 44 However, other studies indicated that current evidence is insufficient to establish a clear association between tourniquet use and the occurrence of postoperative VTE. 45
Many risk factors are associated with perioperative DVT in elderly patients with lower limb fractures. Table 1 summarizes the possible risk factors in accordance with current research. As research advances, a broader spectrum of risk factors is expected to be elucidated. Understanding these intersecting pathophysiological mechanisms is crucial for developing targeted prevention strategies that address the multiple contributors to thrombosis in elderly patients with fracture rather than focusing solely on single aspects of Virchow's triad. Anesthesia providers must recognize that risk accumulates throughout the perioperative period. The highest-risk periods include the time between injury and surgery (when patients are immobile and in pain) and the first 24–48 h postoperatively (when surgical trauma combines with residual anesthetic effects on mobility).
Key Risk Factors for DVT in Elderly Patients with Lower Limb Fracture.

Diagnosis of DVT
Early and reliable identification of DVT is one of the greatest challenges in clinical practice 24 due to atypical presentations, coexisting conditions that mimic DVT symptoms, and limitations imposed by immobilization and postoperative dressings. Many elderly patients have diminished sensory perception or cognitive impairment, delaying symptom recognition. The complexity of diagnosis emphasizes that a multimodal diagnostic approach integrating clinical assessment, biomarker testing, and imaging is essential for effective diagnosis.
Clinical Assessment
The typical signs of DVT, namely, unilateral limb swelling, pain, and warmth, 60 may be masked by post-traumatic edema or obscured by immobilization devices, 30 with many presenting subtle or nonspecific symptoms such as mild discomfort, unexplained tachycardia, or functional decline. The presence of superficial venous dilatation or Homans’ sign (calf pain on dorsiflexion) may raise suspicion but lacks sufficient sensitivity or specificity for definitive diagnosis.
Biomarker Testing
The increase in D-dimer level indicates the formation and dissolution of thrombosis in vivo, which has certain guiding significance for predicting the occurrence of DVT in patients with lower limb fractures. 40 D-dimer levels are affected by many factors such as inflammation, cancer, trauma, infection, age, surgery, hospitalization, and acute diseases like COPD . The test's specificity decreases dramatically in elderly populations and postoperative settings, leading to many false positives. 61 Numerous studies recommend the use of age-adjusted D-dimer cut-off values or algorithms to improve specificity when ruling out DVT in elderly patients with fractures.19,62 Such usage could be highly valuable for increasing clinical applicability. Although D-dimer is almost universally increased in trauma and subsequent inflammation and has limited utility in patients with fractures, 63 a negative D-dimer can reliably rule out DVT in low-risk patients. 64 As an easily available and inexpensive biomarker, increased D-dimer levels can be used in combination with symptoms and imaging findings to identify or rule out VTE in patients. 65 Other biomarkers may play a role in predicting and diagnosing DVT. Zheng et al believe that dynamic detection of peripheral blood D-D, FIB, FDP, and PLT levels can be used for early screening and diagnosis of DVT in patients with lower extremity fractures. 1 Zhang et al identified PLT count, D-dimer level, FIB level, and SII score as independent risk factors for preoperative DVT in elderly patients with hip fracture. 11 Cui et al suggested that people with low PLT, and prolonged PT have an increased risk of developing DVT. 48 In a retrospective analysis of 2566 eligible elderly patients, Cheng Xinqun et al suggested that RDW, HDL-C,66,67 and RHR are valuable biomarkers for predicting the occurrence of preoperative DVT in elderly patients with hip fracture. 68 Ma et al found in their study of 410 preoperative patients with simple closed foot fractures that PDW < 12%, HDL-C < 1.1 mmol/L, ALP > 100 U/L, and serum Na + < 135 mmol/L are associated with DVT. 67 Another study by Ma on simple tibial shaft fractures showed that serum HBDH > 182 U/L was closely related to the occurrence of DVT. 69 Multivariate analysis showed that CRP > 11 mg/L and PLT > 217 × 109 /L were associated with DVT. 70 These markers not only reflect the hypercoagulable state but also serve as valuable predictors of thrombotic risk when combined with clinical assessment and imaging (Table 2). Extracellular vesicles (EVs) contain various biochemical substances, some of which play important roles in DVT. As such, EVs have been investigated as potential biomarkers for identifying post-traumatic DVT. 24 However, the low abundance of EVs in blood, along with difficulties in extraction and high detection costs, may limit their clinical utility. The current study suggests that some easily available and inexpensive blood markers may suggest the risk of DVT before fracture at specific sites, but more evidence is needed. Finding reliable and specific biomarkers to develop DVT prediction models in elderly patients with lower limb fractures is still a research hotspot.
Annotation of DVT-Specific Biomarker Abbreviation.

Thromboelastography (TEG)
TEG is a widely accepted means of assessing coagulation status. TEG shows a strong diagnostic ability in the early diagnosis of DVT.15,71 TEG measures changes in blood viscosity during coagulation, directly reflecting the dynamic evolution of blood clotting, including the rate of clot formation, clot hardness, and the activity of the fibrinolytic system. It provides comprehensive information on the entire process of platelet aggregation, coagulation, and fibrinolysis. This information enables the assessment of clinical risks for thrombosis or bleeding, allowing timely and accurate monitoring of coagulation changes in patients with traumatic lower extremity fractures. 15 As a result, the type and dosage of anticoagulant drugs can be adjusted, leading to more effective prevention of DVT. 72 Indicators, such as reaction time (R) lower than the reference range, reaction Angle (a) higher than the reference range, and maximum amplitude higher than the reference range, were considered to be in a hypercoagulable state. 72 Brill et al found that the risk of DVT was doubled in patients with TEG conforming to a hypercoagulable state. 73 Another retrospective study of TEG in patients with severe limb fractures concluded that mA values ≥ 65 and 72 were associated with 3.6- and 6.7-fold increases in the risk of DVT, respectively. 74
Doppler Ultrasonography
Although Doppler ultrasound is not the “gold standard,” it is very convenient and non-invasive, and orthopedic surgeons have accepted ultrasound examination as a diagnostic method for DVT.17,40 Portable ultrasound allows for bedside assessment when patient transport is difficult. The examination should include the entire lower extremity because isolated femoral or iliac vein thromboses occur more frequently. Doppler ultrasound has gradually replaced venous angiography in widespread use. 30 Smith et al recommended all patients with hip and femoral fractures with delayed surgical intervention (24 h) to undergo preoperative Doppler ultrasonography to rule out DVT. 75 Lower extremity Doppler ultrasonography should be performed routinely in elderly patients with lower extremity fractures. 76 Given that DVT can occur at any time during the perioperative period, noninvasive vascular ultrasound should be routinely performed, especially at different time points during the perioperative period. 77 The American College of Chest Physicians (ACCP) guidelines recommend screening only for patients with high-risk injuries who are not candidates for pharmacological prophylaxis. Given that advanced age and surgical treatment are high-risk factors for DVT, routine Doppler ultrasound screening is warranted for elderly patients with lower limb fractures who are scheduled to undergo surgical intervention. However, ultrasound requires a change in position, which increases the pain of elderly patients with lower limb fractures and reduces their compliance. Moreover, the accuracy of ultrasonography is affected by the expertise of the performing physician. 19
Venography
Venography is recognized as the gold standard for diagnosing DVT. 24 However, compression ultrasonography has now largely replaced it in clinical practice. Venography is no longer a routine clinical procedure and has been redefined as a “reference standard” in validation studies.
CT venography provides comprehensive evaluation from calves to inferior vena cava (IVC) and is often performed concomitantly with CT pulmonary angiography when PE is suspected. For patients undergoing preoperative CT pulmonary angiography for suspected PE, concomitant CT venography can evaluate the iliac veins and IVC, which are sites that may be poorly visualized on ultrasound. Although Doppler ultrasonography demonstrates sensitivity and specificity exceeding 90% in the detection of DVT, 78 some studies suggest that CT venography of the lower extremities may offer advantages over ultrasonography for diagnosing DVT, 79 despite the lack of specific sensitivity and specificity data. However, such use of CT venography imposes an additional risk for people with contrast nephropathy and those who are allergic to contrast agents. In addition, radiation exposure and contrast medium requirements remain disadvantages.
MRI venography offers several theoretical advantages, including excellent soft tissue contrast, ability to image through casts or dressings, and simultaneous evaluation of pelvic veins and alternative pathologies. Despite its high diagnostic accuracy and avoidance of ionizing radiation, the routine clinical application of MRI remains limited due to factors such as high examination costs, restricted availability of equipment, and logistical challenges in transporting acute trauma patients. Furthermore, supporting evidence for the routine use of MRI venography in cases of traumatic DVT is lacking despite its theoretical benefits.
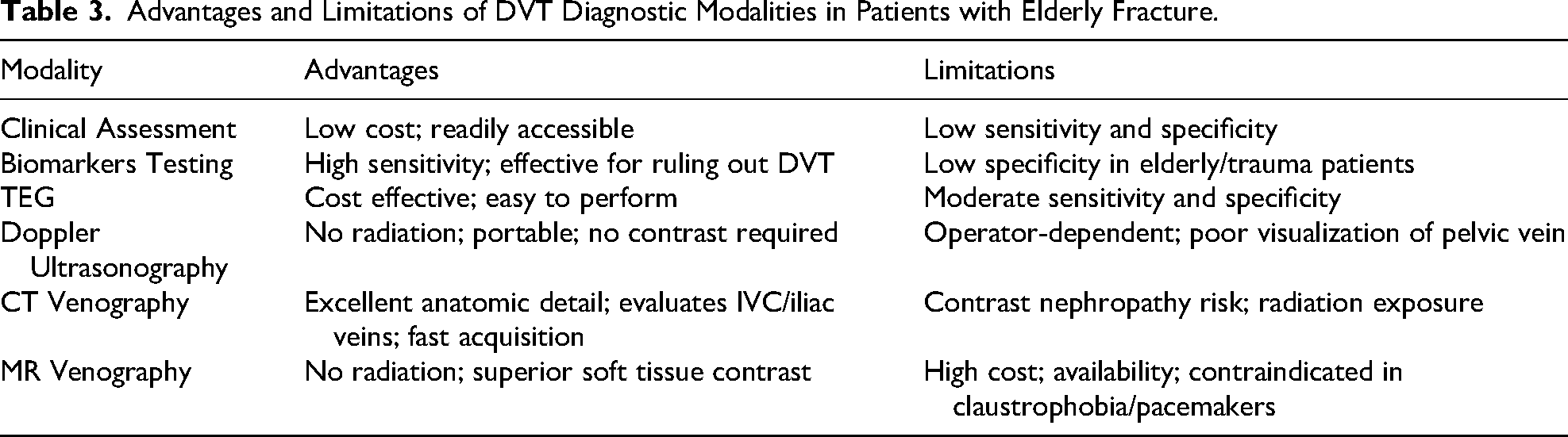
Innovative approaches to DVT diagnosis continue to evolve. Intravascular ultrasound (IVUS) is particularly valuable for evaluating venous stent patency and guiding intervention in chronic post-thrombotic syndrome. Molecular imaging techniques using radiolabeled fibrin-specific drugs or platelets may eventually enable highly specific thrombus detection. However, these technologies remain in the research stage, and they have not yet been routinely integrated into clinical practice. For elderly patients with lower extremity fractures, diagnostic strategies must balance accuracy with practicality while considering mobility limitations, comorbid conditions, and treatment implications (Table 3). A typical algorithm may begin with clinical assessment and biomarkers testing (in low-probability cases), proceeding to vascular ultrasound for positive screens or high-probability presentations, with advanced imaging reserved for inconclusive or complex cases (Figure 1). For anesthesia providers, these diagnostic challenges emphasize the importance of the following: (1) maintaining high suspicion for DVT in all elderly patients with lower limb fracture, (2) advocating for preoperative ultrasound screening when feasible, (3) understanding protocols for managing newly diagnosed preoperative DVT and (4) recognizing that negative imaging does not eliminate risk of subsequent thrombosis. For instance, an observational study conducted by Zhang et al revealed that the preoperative occurrence rate of DVT in patients with lower limb fractures was 35%, which increased significantly to 55% postoperatively. 17 The diagnostic process must be efficient because delays in fracture fixation are associated with increased morbidity and mortality.

Flowchart of diagnostic measures.
Advantages and Limitations of DVT Diagnostic Modalities in Patients with Elderly Fracture.
Prevention Strategies for Perioperative Thrombosis
In recent years, after thrombosis prevention strategies were implemented, the incidence of DVT in patients with lower extremity fractures has decreased from 40%–60% to 10%–20%,30,80 showing the importance of thrombosis prevention. Increasing evidence shows that DVT prophylaxis should be initiated as early as possible in patients with traumatic injury after admission.20,71 A hypercoagulable state is evident within 24 h of trauma and persists for 5–14 days. 81 Active prevention of DVT is the cornerstone of perioperative management in patients with lower extremity fractures, and these measures should begin immediately after admission and continue throughout the postoperative period. 17 Early initiation of DVT prophylaxis preoperatively can shorten the interval from injury to surgery and reduce postoperative complications and mortality.
Mechanical Prophylaxis
Mechanical prophylaxis should be started as early as possible after admission and resumed immediately after surgery when possible. Intermittent pneumatic compression (IPC) provides rhythmic external compression to the calves, mimicking the muscle pump effect and increasing venous flow velocity. Graduated compression stockings create a pressure gradient that reduces venous capacitance and stasis, but guidelines recommend the use of IPC devices over gradient compression stockings, 82 especially in patients at risk for bleeding. 3
Current consensus strongly advocates early mobilization (eg, assisted ambulation, active localized movement, and passive exercises) in the absence of DVT, and it should commence immediately upon hospital admission. 3 Ankle pump motion (dorsiflexion/plantarflexion) was used to simulate the muscle pump action of the calf muscles. Elevating the affected limb at approximately 30 degrees by using wedge pillows optimizes venous drainage. For patients able to tolerate more activity, straight leg raises can begin within 6 h after hip replacement or 1 week after internal fixation surgery. They accelerate venous blood flow in the lower extremities, reduce blood retention, and decrease the incidence of postoperative DVT. 83
Mechanical prophylaxis should be maintained at least until the thrombotic risk is significantly reduced and the patient can perform regular, independent ambulation. For patients undergoing major orthopedic surgery, prophylaxis should be extended up to 35 days postoperatively. In patients in whom physical precautions cannot be used or cannot be applied to the injured limb, these measures should be applied to the healthy limb. 83 For patients at high risk for bleeding, mechanical prophylaxis alone is recommended. 84 However, adherence can be challenging due to discomfort, improper fitting, or interference with wound care. Congestive heart failure, DVT of the lower extremities, thrombophlebitis, PE, and regional anomalies of the lower extremities are contraindications to mechanical prophylaxis. 83
Pharmacological Prophylaxis
For patients with non-high bleeding risk and no contraindications to pharmacological prophylaxis, a combination of mechanical and pharmacological methods is recommended for prevention. 82 First-line agents include low-molecular-weight heparin (LMWH), direct oral anticoagulants (DOACs), and aspirin. Second-line agents include unfractionated heparin (UFH), fondaparinux, and warfarin. Patient- and surgery-specific risk factors should be considered when determining whether to use chemical prophylaxis. Although the 2012 Chinese expert consensus recommended that pharmacological prophylaxis should be initiated preoperatively in patients with femoral fractures, peri-knee fractures, and multiple fractures distal to the knee, anticoagulant therapy may be omitted in those with isolated fractures distal to the knee and no additional risk factors. 85 However, surgical intervention has been identified as a risk factor for DVT, making elderly patients with isolated fractures distant from the knee joint and requiring surgery suitable for pharmacological prophylaxis.86,87 Several studies of fractures below the knee found that pharmacological prophylaxis can significantly reduce the incidence of DVT, and pharmacological prophylaxis is recommended for patients undergoing surgery for fractures below the knee.88,89 The United Kingdom guidelines recommend anticoagulant therapy for single fractures distant from the knee joint. 18 SooHoo et al proposed that elderly patients requiring ankle surgery, those requiring ankle surgery with medical comorbidities, and patients with open ankle fractures should receive pharmacological prophylaxis. 90 For patients with a low risk of bleeding, Ley et al support early pharmacological prophylaxis and recommend initiation within 24 h of injury. 91 For patients with a high clinical suspicion of acute VTE on admission, guidelines recommend parenteral anticoagulation while awaiting diagnostic test results. 92
LMWH
LMWH, such as enoxaparin and nadroparin, remains a first-line drug due to its predictable pharmacokinetics, subcutaneous administration, and extensive evidence base. It is currently the standard treatment for pharmacological prophylaxis. 93 LMWH is derived from UFH through chemical or enzymatic depolymerization, resulting in shortened glycosaminoglycan chains and lessened sulfate groups. It exerts its anticoagulant effect by specifically activating antithrombin to inhibit factor Xa. The half-life of LMWH is approximately 4 h, and its excessive effects can be partially offset by protamine sulfate. The advantages of LMWH include fewer major bleeding complications and a lower risk of heparin-induced thrombocytopenia (HIT) than UFH and absence of routine monitoring.
Existing literature suggests that LMWH is the most effective choice for preventing VTE in patients with multiple orthopedic injuries. 45 ACCP's evidence-based clinical practice guidelines recommend the use of LMWH for the prevention of DVT in patients undergoing major orthopedic surgery, 94 maintaining LMWH as the primary method of pharmacological prophylaxis. 95 However, the optimal timing of initiation remains controversial due to concerns regarding bleeding risk and surgical scheduling. Some studies suggest that LMWH should be administered more than 12 h before or after surgery, whereas others recommend avoiding administration within 4 h of surgery. LMWH is primarily cleared via renal filtration. This consensus recommends a weight-based dosing regimen with adjustments for renal impairment. In patients with renal insufficiency or extreme body weight, monitoring of anti-Xa levels is advised to mitigate a significantly increased risk of bleeding. Drawbacks include the potential for local pain and even subcutaneous induration, and LMWH should generally be avoided in patients with severe renal failure.
For major orthopedic surgery, enoxaparin is administered subcutaneously at a dose of 30 mg every 12 h or 40 mg once daily. The initial dose is given no less than 12 h before or after surgery. Dalteparin is administered subcutaneously at a dose of 5000 U once daily, starting 12–24 h postoperatively. Danaparoid is administered subcutaneously at a dose of 750 U every 12 h, starting 12–24 h after surgery. Nadroparin is administered subcutaneously at a dose of 38 U/kg once daily (maximum dose 3800 U), with the initial dose given no less than 12 h before or after surgery. From the fourth postoperative day onward, the dose is increased to 57 U/kg once daily (maximum dose 5700 U). Tinzaparin is administered subcutaneously at a dose of 75 U/kg once daily, starting 12–24 h postoperatively. For knee surgery, ardeparin is administered subcutaneously at a dose of 50 U/kg every 12 h, starting 12–24 h after surgery. 96
DOACs
As an alternative to LMWH, DOACs are increasingly used to prevent VTE in major orthopedic surgery. 97 They are considered first-line options for postoperative DVT prophylaxis in patients subjected to total hip or knee arthroplasty. The efficacy and safety of DOACs are similar to that of LMWH. 98 Rivaroxaban or apixaban is preferred over edoxaban or dabigatran for perioperative thromboprophylaxis with DOACs. 96 In cases of severe bleeding, specific reversal agents are available to counteract the effects of DOAC. They do not require ongoing monitoring or dose adjustment, and they are suitable for patients with a history of HIT. DOACs should be avoided in patients with severe renal insufficiency.
Rivaroxaban and apixaban are direct factor Xa inhibitors. Their advantages include oral administration, fixed doses, and a lower risk of bleeding than warfarin. These drugs have long half-lives and do not require routine hematologic testing. Oral anticoagulants provide a convenient and continuous treatment strategy for venous thrombosis, and they are commonly used in postoperative anticoagulation. Oral administration of rivaroxaban is started 6–10 h after surgery. Andexanet alfa can be used to antagonize rivaroxaban and apixaban. Rivaroxaban was noninferior to enoxaparin, with a similar risk of bleeding. 83 Its disadvantages include the risk of renal impairment and potential drug interactions.
Dabigatran is a clinically cutting-edge, new-generation oral anticoagulant that functions as a direct thrombin inhibitor. It binds to the fibrin-specific binding site of thrombin, preventing the cleavage of fibrinogen into fibrin. This action blocks the final step of the coagulation cascade and subsequent thrombus formation. Praxbind is an idarucizumab used to antagonize dabigatran. Some studies suggested that dabigatran can be used for the prevention of DVT after total replacement surgery, and its effect is similar to that of low-molecular-weight heparin. 99
Other Medications
UFH activates antithrombin, thereby inhibiting coagulation factors, such as thrombin, factor Xa, factor IXa, and factor XIIa, to exert its anticoagulant effect. Its half-life is relatively short. APTT is used to determine the therapeutic effect of UFH, with a target APTT of 1.2–1.5 times the control value. Routine monitoring of APTT should be performed during treatment, and platelet counts should be monitored to prevent HIT. Protamine sulfate can counteract the excessive effects of UFH, which is administered intravenously or subcutaneously and is predominantly metabolized by the liver and endothelial cells. It may serve as a second-line option for patients who cannot receive LMWH or DOACs, such as those with renal failure. For patients with severe renal impairment, intravenous infusion of UFH combined with routine APTT monitoring can be preferred due to its short and reversible half-life
Fondaparinux, an indirect factor Xa inhibitor by subcutaneous injection, is more effective than enoxaparin in the treatment of DVT. 83 However, its safety profile, particularly regarding bleeding risk, requires further investigation. Its advantages include a fixed dose, a lower risk of bleeding than warfarin, a long half-life, and the absence of routine hematologic testing. Its long half-life (17-21 h) requires careful timing during intravertebral anesthesia. Fondaparinux is recommended to be started 8–12 h after surgery. 100 Its limiting factors include limited reversal options and renal impairing effects. Fondaparinux should be avoided in patients with body weight < 50 kg and those with renal insufficiency.
Vitamin K antagonist (warfarin) is inexpensive, and it can be used for long-term prevention of lower extremity DVT. However, the dose required by different individuals varies greatly, and routine monitoring and dose adjustment are needed to maintain the international normalized ratio (INR) in the range of 2.0–3.0. Warfarin is usually restricted to patients who cannot use LMWH or take DOACs, such as those with severe renal insufficiency. 96 Its limitations include the need for frequent INR monitoring, the potential requirement for vitamin K supplementation in cases of bleeding owing to its exceptionally long half-life, and interactions with other drugs and foods.
Aspirin
An oral antiplatelet agent, aspirin irreversibly inhibits platelet aggregation for the lifespan of platelets, typically 7–10 days. It is not recommended as the sole initial treatment for early-stage thrombosis but is commonly used for long-term prophylaxis in low-risk patients post-surgery. 101 Aspirin effectively inhibits platelet activation and aggregation. Additionally, it reduces the production of thromboxane A2 in platelets, decreases the number of NF-kB positive cells, and downregulates the expression of NF-kB protein, thereby alleviating local inflammatory responses. For patients undergoing total joint replacement surgery, low-dose aspirin (81 mg twice daily orally or 160 mg once daily orally) is recommended as the primary method for preventing DVT postoperatively. 82 For low-risk patients, such as those undergoing elective lower extremity trauma surgery, aspirin can be used postoperatively as a suitable alternative to LMWH. 102
For pharmacological prophylaxis, guidelines recommend preferential use of LMWH. 84 In patients with severe renal failure, UFH is the drug of choice, followed by warfarin. 96 It's worth mentioning that while preventing thrombosis, attention should also be paid to the risk of bleeding. Among several commonly used drugs for thromboprophylaxis, fondaparinux has the highest risk of causing major bleeding events, followed by warfarin, aspirin, and rivaroxaban in order of risk.103–105 When pharmacological prophylaxis was used, warfarin, fondaparinux, and rivaroxaban all appeared to be associated with higher bleeding rates than LMWH. 84 All patients with multiple trauma injuries are recommended to undergo an assessment at the time of admission to mitigate the risks of bleeding and thrombosis. 91 Patients with solid-organ injury can safely receive anticoagulation after 24 h without sustained blood loss if they are hemodynamically stable. 106 For patients with closed craniocerebral injury, if no aggravation of neurological examination occurs within 24–48 h and continuous head CT scan indicates that the condition is stable, anticoagulation therapy can be started after consulting the corresponding specialist. 106
Park and colleagues’ approach to thromboprophylaxis in patients with lower limb fractures can serve as a reference 88 : The prevention strategy is tailored on the basis of bleeding and VTE risk assessments . For patients with a high risk of bleeding, only mechanical thromboprophylaxis is administered before discharge. Patients with low risks of bleeding and VTE are prescribed aspirin. For those with a lower risk of bleeding but a higher risk of VTE, mechanical prophylaxis is initiated immediately after admission, followed by administration of low-molecular-weight heparin 24 h after the initial surgery. The combination of LMWH and IPC is continued during the subsequent hospital stay, and aspirin is prescribed after discharge until 35 days post-operation. A notable detail that this approach assumes surgery within 24–48 h of admission and does not consider preoperative pharmacological prophylaxis. For elderly patients with lower limb fractures who are at increased risk of VTE, have more comorbidities, and may undergo delayed surgery, preoperative pharmacological prophylaxis may be unavoidable.
A retrospective study analyzed 282 patients with traumatic intracranial hemorrhage, among which 94 patients were subjected to prophylactic chemotherapy within 24 h of admission. The results showed no significant difference in the incidence of radiographic expansion of intracranial hematoma. 107 Another small study indicated that administration of LMWH within 24 h after spinal cord injury (SCI) can reduce the risk of DVT without adverse bleeding events. 108 Previous concerns regarding bleeding risks in patients with multiple injuries and the timing of DVT prophylaxis seem to require reevaluation and validation. Until the results of large-scale multicenter clinical trials are available, exercising caution in altering current DVT prevention strategies is prudent.
Combination of Multiple Strategies as Most Effective Prevention
(1) Preoperative Phase: The application of IPC is initiated in the emergency department. If the surgical delay exceeds 12 h, the use of LMWH is commenced. Ankle pump exercises are immediately started. The extremity is elevated using specialized padding. (2) Intraoperative Phase: The use of IPC is continued during surgery. The patient is carefully positioned to avoid venous compression. Compared with GA, spinal anesthesia is associated with a 30%–50% reduction in DVT risk. Normal body temperature (core temperature ≥ 36 °C) is maintained. Reasonable fluid management is implemented to prevent hemodilution. (3) Postoperative Phase: The use of LMWH is resumed after surgery. IPC usage is reinstated when no contraindications are present. Early mobilization is facilitated in combination with physiotherapy. For major orthopedic surgeries, prophylaxis is extended for 4–6 weeks after discharge (Table 4).
Guidelines recommend regional analgesia to improve preoperative pain. 109 Regional analgesia can increase the range of motion of the patient's joint, reduce the stress response, and maintain the homeostasis of the internal environment, so it is conducive to the prevention of DVT. Dehydration should be avoided before, during, and after surgery, and central venous catheters should be avoided if not clinically necessary. 53 Many medications taken by older patients (eg, antihypertensive medications that cause orthostatic hypotension and psychotropic medications that affect balance) can interact with anticoagulants. Cognitive impairment may require supervised medication or a simplified protocol. The most effective prevention strategy should be determined through individualized assessment, taking into comprehensive consideration the patient's comorbidities, injury mechanisms, and the resource allocation of the medical institution. An integrated nursing approach, which has been demonstrated to reduce the incidence of venous thrombosis in surgical patients, should be adopted. Special attention should be paid to high-risk periods, specifically the inflammatory and immobilization phases during the perioperative period, when the risk of thrombosis is greatest and prevention is most critical. Therefore, early prevention of venous thrombosis is essential.
Multimodal Prevention Strategies.

Timing of Surgery in the Context of DVT
Persistent hemodynamic instability, coagulation system dysfunction, advanced age, and comorbidities are often listed as reasons for postponing surgery. The swelling around the knee and ankle joints necessitates postponement of the procedure to allow time for resolution of the edema, thereby avoiding postoperative wound complications. Preoperative management of diagnosed DVT may necessitate delaying surgery. A prospective study by Smith et al found that despite prophylactic anticoagulation, the risk of thromboembolic disease increases when surgery is delayed, and the duration of surgical delay is directly correlated with the incidence of thromboembolic events. 75 Determining the optimal timing of surgical intervention for elderly patients with lower extremity fractures is a complex clinical decision that significantly affects thrombosis risk and overall outcomes. As perioperative physicians, anesthesiologists play a crucial role in balancing surgical stability with the need for thrombosis risk assessment and management. Current evidence strongly supports early surgical intervention for most elderly patients with hip fractures.7,20,109,110 The physiological rationale for early surgery is to break the vicious cycle of immobility, pain, and inflammation that promotes thrombosis. 111 Surgical stabilization enables patients to mobilize, control pain, and restore baseline activities, all of which can reduce venous stagnation and hypercoagulability. Adequate preoperative preparation may conflict with early surgery, but comprehensive and scientific evaluation and management are key to avoiding unnecessary delays in surgery.
In the absence of preoperative DVT, early surgery is strongly recommended. If DVT is present, the risk of thrombus mobilization during surgical manipulation necessitates tailored perioperative planning.
76
Therefore, when DVT has been diagnosed preoperatively, the timing of surgery and preoperative management must consider thrombus characteristics and embolic risk.
For distal DVT (located below the popliteal vein), fracture fixation can generally be performed within 24–48 h, and therapeutic anticoagulation should be initiated concurrently.92,112 If multiple risk factors for thrombus progression are present (eg, extensive soft tissue injury and history of malignancy), temporary IVC filter placement should be considered.
113
Continuous ultrasound monitoring is recommended to track thrombus progression.
92
Proximal DVT, where the thrombus is located in or near the popliteal vein, poses an increased risk of perioperative PE. If the patient is hemodynamically stable, anticoagulation therapy should be administered for 3–5 days prior to surgery. In cases of hemodynamic instability or when immediate surgery is necessary, preoperative placement of an IVC filter is advisable.
113
During surgery, special care should be taken to minimize limb manipulation and maintain hemodynamic stability. In the presence of free-floating thrombi, extensive DVT, or acute PE, surgery should be postponed, and full anticoagulation therapy (typically for at least 5-7 days) should be administered. Cardiopulmonary stability should be assessed before considering fracture fixation and thrombolysis. The use of an IVC filter is required prior to fracture fixation (Table 5).30,75
Recommended Timing for Surgery Following Thrombosis Diagnosis.

For patients with acute DVT of the leg, guidelines recommend anticoagulation alone over interventional (thrombolysis, mechanical, or pharmacomechanical) treatment. 92 For patients with acute DVT of the leg who undergo thrombectomy or venous filter placement, guidelines recommend anticoagulation of the same intensity and duration as similar patients who do not receive similar treatment.92,114 For most patients with acute PE who are hemodynamically stable, routine thrombolytic therapy following anticoagulation is not recommended. 92 For some patients with acute PE, systemic thrombolytic therapy is recommended when the condition deteriorates and the vital signs are unstable after the initiation of anticoagulant therapy. 115 In patients with acute PE and hypotension (systolic BP < 90 mm Hg or a decrease of ≥ 40 mm Hg from baseline) or selected normotensive patients with signs of shock or respiratory failure, postponing surgery to administer systemic thrombolysis is appropriate if bleeding risk is low. 92 For patients with acute PE treated with thrombolytic agents, systemic thrombolysis via peripheral veins is recommended over catheter-directed thrombolysis. 92 Catheter-assisted thrombectomy is recommended for patients with acute PE and hypotension in the presence of concomitant high bleeding risk, failure of systemic thrombolysis, or shock that may lead to death before systemic thrombolysis takes effect.92,116
Anesthesiologists should note that in patients who require a temporary IVC filter before emergency surgery, IVC filter placement often prolongs the preoperative time by 12–24 h. Anesthesia at the time of IVC filter placement may influence subsequent anesthetic planning. IVC filters reduce the risk for PE but do not eliminate it. When the indication for filter placement no longer exists, the device should be retrieved within 29–54 days. 18 In general, filters should be removed approximately 2 or 3 weeks after orthopedic surgery to reduce the risks of filter migration, tilt, embolism, fracture, and perforation. 117
Intraoperative Anesthetic Considerations in Elderly Patients with Lower Extremity Fractures with Preoperative Thrombosis
The incidence of DVT remains high despite the implementation of recommended preventive measures in patients. 118 The presence of DVT in elderly patients with lower limb fracture profoundly influences anesthetic management, requiring meticulous planning and execution to minimize thrombotic complications while ensuring patient safety and surgical feasibility. Anesthesiologists must navigate a complex landscape of pharmacological interactions, physiological vulnerabilities, and technical challenges unique to this population.
Positioning
Proper positioning can considerably affect venous hemodynamics during the preoperative and intraoperative periods. Using a wedge-shaped positioning device to elevate the affected limb approximately 30 degrees optimizes venous return dynamics. This simple measure reduces venous pressure and stasis in the perioperative period. During fracture fixation, prolonged extreme flexion or compression of the groin or popliteal areas should be avoided because it could impede venous flow. Periodic repositioning of unpadded extremities may be beneficial during lengthy procedures.
Choice of Anesthetic Technique
The decision between GA and neuraxial/regional anesthesia should balance thrombotic risks, anticoagulation status, and surgical requirements.
Neuraxial anesthesia: Advantages include a reduced incidence of DVT (14%–24% lower than GA).
119
Good postoperative analgesia facilitates early mobilization. Airway manipulation should be avoided in patients with frequent pulmonary comorbidities. Absolute contraindications include patient refusal, infection at the puncture site, and severe coagulopathy (INR > 1.4, platelets count < 50 × 109/L). Relative contraindications include a fixed cardiac output state (severe aortic stenosis) and preexisting neurologic deficits. Timing considerations: Anticoagulation drugs should be temporarily discontinued before neuraxial anesthesia to prevent spinal hematoma. Clopidogrel should be discontinued 7 days before surgery, aspirin 5 days before, and rivaroxaban 24–48 h before, with LMWH used as a bridging anticoagulation during this transition period.
100
LMWH should be discontinued 24 h before surgery.
100
The standard dose of LMWH should be administered subcutaneously at least 12 h after surgery.
96
Fondaparinux is recommended to be started 8–12 h after surgery.100,120 DOACs are usually initiated 24 h after surgery, whereas warfarin is typically started within 24 h postoperatively.
100
If heparin is used during the perioperative period, it should be discontinued 8–12 h before surgery and resumed 2–4 h after surgery.
83
INR < 1.5 is required when using warfarin; specific drug guidelines should be followed for DOACs, typically 2–5 half-lives. GA: This type of anesthesia is performed when the patient is unable to cooperate with neuraxial anesthesia and surgery due to mental factors or when neuraxial anesthesia has contraindications such as local infection and anticoagulant state. GA can be utilized alone or in combination with regional techniques such as neuraxial anesthesia or peripheral nerve blocks. Peripheral nerve blocks: These have become valuable alternatives, particularly ultrasound-guided nerve blocks, which avoid the anticoagulation issues of neuraxial anesthesia. Continuous catheter techniques at specific sites, selected in accordance with the fracture location, can provide prolonged postoperative analgesia. Peripheral nerve blocks can be used as adjuncts to GA or spinal anesthesia and for preoperative and postoperative analgesia.
121
However, they should only be used as the sole anesthetic technique in situations where neuraxial anesthesia and GA carry special risks due to the incomplete and unsatisfactory pain relief provided by these nerve blocks (Table 6).
122
Advantages and Disadvantages of Different Anesthesia Methods.

Intraoperative Monitoring
Beyond routine monitoring, such as electrocardiography, blood oxygen saturation, and noninvasive blood pressure, additional monitoring modalities may be considered for patients at increased thrombotic risk. Elderly patients are susceptible to intraoperative hypothermia, and temperature monitoring is beneficial for preventing DVT and reducing postoperative complications. For patients with left ventricular dysfunction or heart valve disease, invasive arterial pressure monitoring is particularly advantageous during surgery. Central venous pressure monitoring or echocardiography is recommended for patients suspected of ventricular dysfunction or undergoing revision/periprosthetic fracture surgeries. Capnography, which detects sudden decreases in end-tidal carbon dioxide concentration, can indicate intraoperative PE. Specialized coagulation monitoring, such as TEG or rotational thromboelastometry, guides blood transfusion, and point-of-care platelet function testing is valuable for patients on antiplatelet therapy. Dilution techniques have become increasingly accurate, and they can be employed for invasive blood pressure monitoring. Additionally, bispectral index monitoring aids in optimizing the depth of anesthesia, thereby avoiding potential cardiovascular depression.
Anesthesia Management
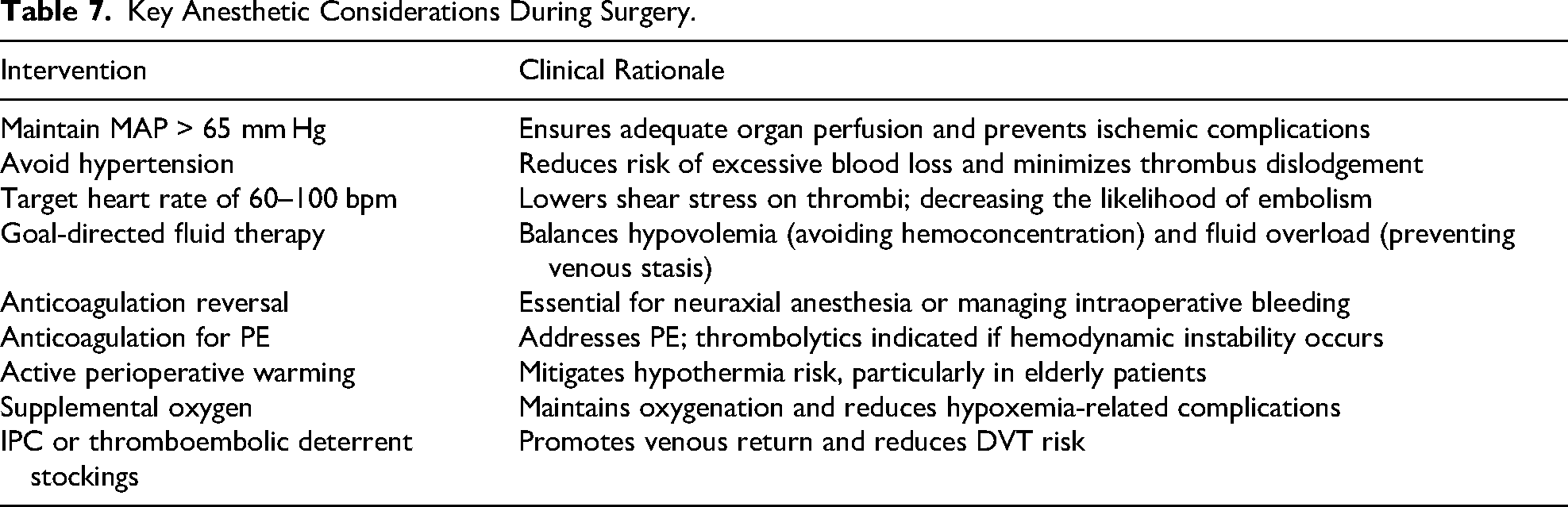
Patients with preexisting DVT or PE are at risk of thrombus detachment during surgery due to positional changes, mechanical manipulations, or hemodynamic fluctuations. The anesthesiologist should maintain hemodynamic stability to prevent thrombus propagation and myocardial ischemia as follows: ensuring that the mean arterial pressure (MAP) is greater than 65 mm Hg to guarantee organ perfusion while avoiding hypertension because it increases the risk of increased venous pressure and thrombus displacement, controlling the heart rate within the target range of 60–100 beats per minute because tachycardia can increase thrombus shear force, and adopting a goal-directed fluid therapy approach (such as stroke volume variation or other dynamic parameters) to prevent hypovolemia (which may lead to hemoconcentration) and fluid overload (which may cause venous stagnation). Anticoagulation reversal therapy should be planned for cases requiring intrathecal techniques or intraoperative bleeding management. Anticoagulation therapy should be administered for PE, and thrombolytic therapy should be considered for hemodynamically unstable patients. 123 During surgery, active warming strategies should be implemented because elderly patients are prone to intraoperative hypothermia. Meanwhile, supplemental oxygen should be continuously provided throughout the surgical procedure to prevent hypoxemia. Additionally, the use of IPC or thromboembolic deterrent stockings during the operation is recommended to enhance blood return and prevent DVT (Table 7).
Key Anesthetic Considerations During Surgery.
Postoperative Considerations
Early mobilization should be carried out under the guidance of a doctor. Mechanical prophylactic measures should be taken as early as possible postoperatively and continued consistently. When the risk of bleeding is low to moderate, postoperative pharmacologic prophylaxis should be continued in accordance with guidelines.82,84 Postoperative attention should be paid to the prevention and treatment of comorbidities. Appropriate postoperative analgesia should be ensured, and postoperative vomiting should be prevented. Suitable thermal insulation measures should be taken to prevent hypothermia. Elderly patients are at risk of postoperative hypoxemia, and they may require postoperative oxygen inhalation for more than 24 h. Guidelines recommend against routine postoperative Doppler ultrasound screening, 84 but prompt examination should be performed when bleeding or thrombotic manifestations are suspected. The catheter should be removed as soon as possible to reduce the risk of urinary tract infection. Postoperative bleeding should be monitored, and fluid or blood transfusion should be administered promptly.
Discussion
The importance of an effective thrombosis risk assessment system has been mentioned in numerous studies; however, no validated stratification system specifically for orthopedic thrombosis risk assessment is currently available.53,124 Presently, commonly used thrombosis risk assessment models include the Caprini Risk Assessment Model (Caprini RAM), Wells Rules, and the Greenfield Risk Assessment Profile. The Greenfield Risk Assessment Profile is a risk stratification scoring system designed to guide the monitoring and prevention of VTE in trauma patients. 125 However, the Greenfield system incorporates variables that may appear long after admission or even after discharge, and it classifies a considerable number of VTE cases as low-risk trauma patients. Thus, its predictive value and clinical utility remain controversial. The Wells score has limited applicability for fracture patients who routinely receive high scores due to immobilization. Some studies have indicated its low sensitivity, and its orthopedic utility warrants further validation. 30 The Wells score is more suitable for outpatient settings rather than inpatient care. 126 The Caprini score not only enables risk assessment but also provides relevant preventive measures. It has been validated for VTE risk assessment in critically ill surgical patients, general surgical patients, and urological patients. 127 Some studies have analyzed the sensitivity of the Caprini score in predicting the risk of DVT in lower extremity fractures, suggesting that it can serve as a risk screening indicator for DVT in these fractures. 15 Some studies suggest that the Caprini score may help identify orthopedic patients who require special attention, such as those with isolated trauma below the knee. 5 Current orthopedic practices in the United States recommend pharmacological prophylaxis for trauma patients with injuries at or above the knee (eg, femoral shaft, hip, and pelvic fractures), and controversy exists regarding patients with isolated trauma below the knee. The Caprini score benefits the trauma population by helping to identify patients who require pharmacological prophylaxis. 5 According to Lin's research, the Caprini RAM demonstrates moderate predictive ability for VTE risk in patients undergoing primary total hip arthroplasty or total knee arthroplasty, indicating the need for further refinement. 128 Therefore, the Caprini score still needs further refinement and validation for its applicability in orthopedic diseases.5,128
In a cohort study evaluating over 25 million patients, the authors observed a gradual decline in filter placement after 2006, without any concurrent change in the incidence of PE. 129 This finding suggests that the benefits of IVC filters in reducing the risk of PE may be limited. Furthermore, guidelines do not recommend IVC filter placement as the preferred preventive option for patients undergoing major orthopedic surgery who have an increased risk of bleeding or contraindications to pharmacological and mechanical thromboprophylaxis. 84 However, for patients with lower extremity fractures and DVT requiring orthopedic surgery, anticoagulation therapy alone appears to be ineffective in preventing PE.113,130–132 Surgery itself is a risk factor for VTE in patients with lower extremity fractures and DVT, and “doing nothing” is considered unacceptable. 113 In the guidelines of the Society of Interventional Radiology, patients with VTE who are considered to have a significantly high risk of PE despite anticoagulation therapy are viewed as having a relative indication for IVC filter placement. 133 Due to procedures, such as the use of tourniquets, frequent movement of the affected limb, fracture reduction and fixation, and positional changes during orthopedic surgery, patients with DVT undergoing orthopedic surgery have an increased risk of PE. 113 Consequently, many hospitals opt for IVC filter implantation before surgery for patients with DVT. Over years of development and progress, the reported incidence of complications after filter placement is currently very low, and the percutaneous placement convenience has increased the use of filters. 134 The indications for IVC filter placement include the following: (1) pelvic and/or lower extremity fractures requiring surgical treatment, complicated by DVT, with the proximal end of the thrombus located above the knee; (2) detection of free-floating thrombus by ultrasonography; and (3) peripheral DVT of the lower extremity with planned fracture surgery at or below the knee.93,117 Some studies have indicated that below-knee DVT carries a high risk of progression to above-knee DVT, and the risk of PE associated with below-knee DVT is not lower than that of above-knee DVT.113,130,135 Pan and colleagues recommend filter placement for below- and above-knee DVT, which can significantly reduce the incidence of PE. Therefore, they suggest filter placement for patients with lower extremity fractures complicated by DVT, including those with peripheral DVT.113,117 The expert consensus on DVT diagnosis and management from the Chinese Orthopaedic Association recommends filter placement, in addition to anticoagulation therapy, for patients with DVT who require orthopedic surgery after admission. 136 Although significant progress has been achieved in filter placement techniques and post-placement management, and the incidence of complications is already low, 134 attitudes toward filters differ among different hospitals and patients. Moreover, most guidelines do not recommend filter implantation for patients without contraindications to anticoagulation. Further studies must establish the cost-benefit ratio of filter placement and continuously update guidelines and consensus on filter implantation.
No significant differences in mortality, pneumonia, myocardial infarction, cerebrovascular accident, acute confusional state, nor length of hospital stay were found between GA and neuraxial anesthesia for hip fracture surgery in adults, and only very low-certainty evidence links neuraxial anesthesia to a decreased incidence of DVT when used without potent thromboprophylaxis. 122 Guidelines consider a strong evidence supporting similar outcomes between general and spinal anesthesia for hip-fracture surgery. 109 However, evidence suggests that compared with GA, the use of neuraxial anesthesia during joint replacement reduces the possibility of VTE after lower extremity joint replacement, causes less systemic perturbation in elderly patients, and is associated with decreased postoperative complications and enhanced postoperative outcomes, Therefore, neuraxial anesthesia is recommended whenever feasible. 119 A retrospective propensity-score matched-pairs cohort study by Malhas et al showed that spinal anesthesia was associated with lower rates of PE and major bleeding and shorter hospital stays after hip fracture surgery than GA. 137 Regional anesthesia is associated with improved perioperative outcomes in elderly patients undergoing hip fracture surgery, and regional anesthesia reduces the risks of in-hospital death, acute respiratory failure, prolonged hospital stay, and readmission compared with GA.138–140 Memtsoudis et al analyzed data from 400 hospitals and found that compared with GA, the application of neuraxial anesthesia in primary joint replacement surgery was significantly associated with a reduced 30-day mortality rate, shorter hospital stays, lower costs, and a significantly reduced incidence of in-hospital complications. They concluded that neuraxial anesthesia is associated with the most favorable complication risk profile. 141 The Scottish Intercollegiate Guidelines Network recommends that spinal/epidural anesthesia should be considered for all patients undergoing hip fracture repair unless contraindicated. 142 Further research is needed to determine the optimal anesthesia method for elderly patients undergoing lower extremity fracture surgery. Until clear results are available, the choice of anesthesia method should be based on the hospital's available resources, the anesthesiologist's proficiency in different techniques, and individual patient factors. Nevertheless, when neuraxial anesthesia is technically feasible, contraindication-free, and performed by proficient practitioners, it remains the authors’ recommended priority approach.
Despite early and adequate assessment and prophylactic treatment of the risk of DVT in elderly patients with lower extremity fractures, the current incidence of DVT remains high. Refinement in the existing thrombosis risk assessment systems, bleeding risk assessment systems, and pharmacological prevention strategies has remarkable potential. Further research should focus on developing an artificial intelligence (AI)-based risk assessment system for thrombosis and bleeding, incorporating newly identified risk factors and biomarkers. This system should provide safer and more effective prevention recommendations, ultimately enhancing the safety of surgical procedures for elderly patients with lower extremity fractures.
Conclusion
DVT is a common, high-risk complication in elderly patients with lower extremity fractures during the perioperative period. Early identification, prevention, and management of DVT are crucial for reducing perioperative morbidity and mortality. Anesthesiologists should be well-versed in the pathophysiological mechanisms of thrombogenesis, recognize DVT risk factors, and utilize standardized protocols for routine DVT screening. While maintaining vigilance regarding bleeding risks, the implementation of early, multimodal, and individualized prophylactic or therapeutic measures is essential. Anesthesiologists must carefully weigh the benefits of thromboprophylaxis against the risk of hemorrhage while addressing the inherent conflict between preoperative comorbidity optimization and timely surgical intervention, striving to perform surgery within 48 h post-injury. Key strategies include selecting the appropriate anesthetic technique, ensuring safe and effective intraoperative management, optimizing early mobilization with adequate postoperative analgesia, initiating early anticoagulation, and preventing complications. Multidisciplinary collaboration with surgeons and other specialists should be emphasized. Anesthesiologists, surgeons, and relevant professionals should jointly develop standard protocols for elderly patients with lower extremity fractures in accordance with different risk stratifications, which should be based on evidence-based medicine that is updated in a timely manner. Besides, in case of emergency PE occurring perioperatively, a rescue team that includes interventional physicians, radiologists, anesthesiologists, and surgeons should be established. AI-based risk assessment systems should be developed on the basis of big data models regarding meta-analyses and guidelines from authoritative sources. They can be applied to advise clinical professionals before admission, surgery, and discharge.
Footnotes
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All authors gave their consent for publication.
Author Contributions
Yanping Jian: Conceptualization, Formal analysis, Methodology, Visualization, Validation, Writing–original draft, and Writing–review and editing.
Zhendong Huang: Conceptualization, Project administration, Validation, and Writing–review and editing.
Qing Liu and Fei Wang: Review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data and materials generated and analyzed in this study are available from the corresponding author upon reasonable request
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT to improve the readability and language of the manuscript. Afterwards, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.